Open Access Library Journal
Vol.03 No.08(2016), Article ID:69790,10 pages
10.4236/oalib.1102404
Impact of Patent and Proprietary Medicine Vendors Training on the Delivery of Malaria, Diarrhoea, and Family Planning Services in Nigeria
Chukwunonso Iheoma1*, Babajide Daini1, Suliatu Lawal1, Mukhtar Ijaiya2, Wole Fajemisin1
1Measurement, Research and Evaluation Department, Society for Family Health, Abuja, Nigeria
2Monitoring and Evaluation Department, Association for Reproductive and Family Health, Abuja, Nigeria

Copyright © 2016 by authors and OALib.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/


Received 25 May 2016; accepted 12 August 2016; published 15 August 2016

ABSTRACT
This study aimed to investigate the impact of PPMV training on their expertise to deliver quality healthcare services to the Nigerian public. The participants were trained on counseling and dispensing of family planning products diarrhea, and malaria products. The study adopted a multistage sampling method and selected a random sample of 1133 PPMVs trained by SFH between 2011 and 2014 who were interviewed between May and June 2015. Data were analyzed using descriptive statistics and logistic regression methods. Results reveal that training attendance was significantly associated with adequate knowledge of diarrhea treatment and knowledge of family planning counseling services. PPMVs who attended training twice, and those who attended more than twice over the four years preceding the study were more likely to have adequate knowledge of diarrhea treatment than those who attended only once. Similarly, within the same four-year period, PPMVs who attended training twice and those who attended more than twice were more likely to have adequate knowledge of family planning counseling services than those attending once. Significant association between training attendance and knowledge of malaria treatment was not found. Adequate PPMV training program should be streamlined into the national primary healthcare development program.
Keywords:
Healthcare, Diarrhea, Malaria, Family Planning, PPMV
Subject Areas: Public Health

1. Introduction
With a population of about 170 million people, Nigeria is considered as the most populous black nation on earth, and has the largest economy in Africa. Over 50% of the country’s population still live below poverty level. Majority of the Nigerian population living in the rural areas survive solely on subsistence agriculture and face limited access to healthcare facilities. It is estimated that there are about 17,000 pharmacists serving over 170 million Nigerians, implying that there is one pharmacist for every 10,000 citizens. This leaves the urban areas with better access to pharmaceutical services as most pharmaceutical shops operate in that area. The inequalities between the urban and rural areas in terms of access to healthcare services informed the decision of the Federal Government of Nigeria to commence the licensing of the Patent and Proprietary Medicine Vendors (PPMVs) so that they can extend healthcare products and services to the rural population.
PPMVs play an important role in increasing access to health services for communities. In Nigeria, like in many other developing countries, small commercial drug stores provide the first line of healthcare. They are accessible, affordable and are valuable sources of healthcare services, products and information. Despite that most PPMVs possess low educational qualification, they are still seen as the most reliable sources of healthcare in most rural and hard-to-reach areas. This explains the utilization of their services by about 33% of Nigerians [1] .
PPMVs provide a wide range of healthcare products and services including malaria and diarrhoea treatment as well as family planning services. Interest is growing in the use of PPMV for malaria control and prevention. When faced with symptoms of malaria, over half of Nigerians visit PPMVs for treatment. In Nigeria, PPMVs are allowed to sell antimalarials according to Nigeria’s 2011 National Policy on Malaria Diagnosis and Treatment but are not allowed to provide rapid diagnostic testing (RDT) to clients with fever.
In Nigeria, about 50% of oral contraceptive pill users obtain their products and counseling services from PPMVs, although the counseling services offered by PPMVs often fall short of safety guidelines related to the use of oral contraceptive pills. This capacity gap highlights the need to continuously update the counseling knowledge of PPMVs to ensure that they provide quality oral contraceptive services as they bridge the gap between medical experts and healthcare seekers in rural communities.
Regarding diarrhoea treatment, PPMVs play important role in stocking and recommending diarrhoea treatment drugs, especially oral rehydration therapy (ORS) and Zinc tablets to caregivers. A study in two Nigerian states shows that about 89.9% of PPMV shops stocked ORS for treatment of diarrhoea, and this was associated with having formal health training [2] .
Despite the major role PPMVs play in delivering healthcare products and services to the urban poor and rural dwellers, their capacity to effectively carry out this role is limited and this can be attributed to their level of formal health training. For example, a study in Kaduna state found that 80% of customers bought malaria drugs from PPMVs without prescriptions. Only 29.5% were given instructions about doses. In another study in Tanzania [3] , it was found that PPMVs in drug shops recommended use of ORS less frequently (3%) for a combination of diarrhea. The study showed that antibiotics were overused in both the urban and rural settings and that was due to both clinicians’ and drug sellers’ prescribing practices in public and private facilities. Whilst the optimal action to be taken when faced with complications arising from intake of oral contraceptive is to refer such client to a health facility, [4] found that 51% of clients reporting such case to PPMVs were instead treated by them, depicting their poor knowledge of the right course of action.
Poor quality of service delivery by the PPMV amidst the growing demand for their services remains a source of concern for public health stakeholders. However, despite their poor educational background, it has been observed that with adequate training, PPMVs will be able to gain adequate knowledge to deliver quality health care services to their clients. In realization of this fact, the Society for Family Health (SFH) through the Expanded Social Marketing Project in Nigeria (ESMPIN) provides comprehensive periodic training (focusing on family planning, malaria, and diarrhoea) and learning opportunities to proprietors of drug stores and pharmacies in Nigerian in order to strengthen their provision of quality healthcare services to the poor and vulnerable. SFH assists drug store proprietors and pharmacies to conform to quality and performance standards required to provide appropriate services.
It is important to ensure that the trainings offered so far are achieving the desired effects and to provide valid information in guiding future programming in similar projects. This study therefore assesses the impact of the PPMV capacity development programme on the quality of malaria, diarrhoea, and family planning services provided by the PPMVs.
2. Literature Review
This section reviews the findings of various studies conducted on this subject. Various related studied so far conducted had differing objectives. While some focused on understanding the knowledge of PPMVs on malaria and diarhoea treatment, others studied PPMVs’ family planning counseling skills. Overall, there seem to be an empirical consensus that knowledge of optimal treatments for malaria, diarrhoea, provision of quality family planning services, as well as stocking of essential products by the PPMVs are critical for ensuring adequate provision of healthcare services to the vulnerable population.
A study conducted in two Nigerian states (Kogi and Kwara) revealed that wholesale of drugs and participation in any training in the previous year were associated with a higher likelihood of naming the correct treatment for malaria, and having formal health training was associated with stocking ORS. About 89% of shops stocked ORS for treatment of diarrhoea, while 61% of shops stocked artemisinin-based combination therapies (ACTs) for treatment of malaria, although stocking patterns varied by state, urban/rural location, and according to whether or not the shop was headed by someone with formal health training (e.g. having a professional health education degree) [2] .
In a related study that examined the care-seeking behavior of patients from the PPMVs in two Nigerian states (Kogi and Kwara), [2] reported that most customers sought care for headache (30.5%), fever (22.9%), cough/ cold (18.1%), or diarrhea (8.4%). Customers with fever were less likely to discuss the illness with and be examined by the shop worker. Equally, customers with headache symptoms were less likely to experience this outcome. Those reporting cough or cold symptoms were less likely to wait longer before visiting the PPMV shop, and were more likely to discuss the illness with the shop worker. If a sick child was brought to the shop, a discussion of the illness and an exam were more likely and more money was spent on drugs.
Due to high incidence of malaria in Nigeria, management of presumptive malaria in children by the PPMVs has been widespread. A study in Kaduna state found that 80% of customers bought malaria drugs from PPMVs without prescriptions. Only 29.5% were given instructions about doses. Further analysis show that between 40% - 100% doses of PPMV-recommended anti-malaria drugs were incorrect [5] .
A comparative analysis of the level of knowledge of malaria management between PPMVs and general shop- keepers in Tanzania revealed that shopkeepers in drug stores were able to name more malaria symptoms and were more knowledgeable about malaria treatment than their peers in general shops. In drug stores, 52% mentioned the correct child-dosage of sulphadoxine-pyrimethamine compared to only 3% in general shops [6] .
Due to the growing threat of antibiotic resistance partly due to inappropriate medicine use by healthcare providers in northern Nigeria, [7] investigated PPMVs’ treatment of children under 5 years in northern Nigeria in order to determine whether the training of PPMVs influence antibiotic prescriptions. Some 117 (23.8%) PPMVs had training in western medicine (mainly in nursing) and most of them prescribed antibiotics more often than PPMVs without such training. PPMVs prescribed antibiotics because the drugs were thought to be effective. Another reason for prescribing antibiotics even when not needed was to meet expectations of the parents. Thirty- seven percent of responding PPMVs used substandard doses.
A study of PPMVs prescription practice in Tanzania reveals that fever (14%), and diarrhoea (13%) reported in under-5 children were treated with or without prescriptions at drug shops. The majority of drug sellers prescribed or dispensed branded drugs for most caregivers who visited these drug shops. In addition, antibiotics in total were prescribed for 31% of the caregivers. Of the antibiotics dispensed, 38% were not prescribed by clinicians. Of the diarrhoea cases presented by simulated clients at the drug shops, only 35% of the bloody diarrhoea scenarios were accurately diagnosed for getting antibiotics as compared with 44% for watery diarrhoea for which the use of antibiotics were wrongly advised. Furthermore, PPMVs in these drug shops recommended use of ORS less frequently (3%) for a combination of diarrhoea, The study showed that antibiotics are overused in both the urban and rural settings and that this is due to both clinicians’ and drug sellers’ prescription practices in public and private facilities, [3] .
In a study to access PPMVs practices and awareness of new Nigerian Artemisinin Combination Therapy (ACT) policy in three Nigerian states, [8] find that some PPMVs (43.1%) were aware of the 2005 government policy that changed the recommended first-line treatment for malaria from chloroquine (CQ) to ACT, but significant differences were found between states. PPMV shops stocked many brands of anti-malarial drugs (average 5.5 brands), with ACTs stocked in only 8.5% of the stores at a mean price of N504 ($2) per treatment, compared to sulfadoxine-pyrimethamine found in 92% of the shops (at a mean price of N90 ($0.7) and even monotherapy artesunates reported in 32% of shops (at a mean price of N39 ($0.3).
A study to determine the level of utilization of ACT by caregivers for malaria treatment among under-five children in Nigeria found that 51.2% of respondents bought affordable medicine facility-malaria (AMFm-ACTs) without prescription. Awareness of ACT was low as only 9.1% had heard about the product. Overall, 29.2% used AMFm-ACTs as their first line choice of antimalarial drug. On bivariate analysis, age, respondents with tertiary education, respondents with high socioeconomic status, respondents with poor knowledge of symptoms of malaria, awareness of AMFm-ACTs, availability of AMFm-ACTs, and sources of drug were found to be significantly associated with utilization of AMFm-ACTs [9] .
[10] investigated the interaction between PPMVs and their customers in Oyo state, Nigeria and found that the most common PPMV behaviours are: selling the requested medicine (69%), giving their own suggestions to the customer (30%), asking questions about the illness (19%) and providing instructions on how to take the medicine (21%). Only three referrals were observed. The large number of specific drug requests was evidence of a public that was actively involved in self-care, and thus the major role of the PPMVs appeared to be one of salesperson meeting that need. A second role became evident when the customer actually complained about his/ her illness, a practice associated with the more active PPMVs who asked questions, gave suggestions and provided information.
[4] assessed the quality of advice provided by PPMVs to users of oral contraceptive pill in urban Nigeria. Findings revealed that majority of the PPMVs had pills in stock on the day of the survey and resupplied pills to the clients. PPMVs also understood the reason and importance of referring clients who were new adopters of oral contraceptive methods to a health facility; 30% of the PPMVs referred new adopters to a health facility. However, demand from clients who do not want to go to healthcare facilities (for various reasons) necessitated the provision of oral contraceptive pills to 41% of the first time users. Some PPMVs prescribed treatment to mystery clients who presented with perceived complications arising from the use of pills, while 49% were referred to a health facility.
The study by [11] characterized the differences in care-seeking behaviour and dispensing outcomes between adults and children purchasing drugs for malaria at retail shops in Nasarawa state, Nigeria. Their findings revealed that caregivers of sick children were more likely to obtain a prescription prior to visiting a drug retailer than adults seeking care for themselves and waited a shorter time before seeking care. Caregivers of sick children were also more likely than sick adults to have been asked about symptoms by the retailer, to have been given an examination, and to have purchased an ACT. Only 14% of adults, but 27% of children were RDT-positive; RDT-positive children were more likely to have had an ACT purchased for them than RDT-positive adults.
Although various researches have been carried out on the subject, none of those studies was comprehensive in terms of service coverage. While some studies concentrated only on malaria, others focused only on diarrhoea, while family planning received mild attention. This study will cover this empirical gap by integrating the three service areas into the study. In terms of geographical coverage, previous studies on the subject were limited. This study will maintain a national coverage in the sample size distribution. Also, none of the studies considered the impact of PPMV training on their knowledge level, which is the hallmark of this study.
3. Methodology
The study methodology was designed to focus on PPMVs trained by SFH between 2011 and 2014. Since 2011, SFH has trained a total of 47387 PPMVs and is committed contractually to train 60,000 PPMVs in five years. A systematic random sampling technique was employed to determine sample of locations and of respondents. Our sampling frame was based on the geo-political zone (GPZ) strategy, and followed a multi-stage procedure. The multi-stage sampling procedure was implemented as follows: All states where trainings were conducted within the four year period (2011-2014) were grouped into their GPZs. One-third (2) of the 6 states in each GPZ was selected, that is, 2 states per GPZ, totaling 12 states. A random sample of 1133 PPMVs trained within the sample period was selected for the study from the 12 states.
Between May and June 2015, an interviewer administered questionnaire was used to collect data on the levels of knowledge and practice on the subject matter and the perceptions of the quality and possible benefits of the training. The questionnaires were structured to focus on the specific components of the training and how these have increased knowledge that are being utilized by the PPMVs to improve their service delivery. PPMVs were disaggregated by the number of trainings attended. The knowledge of malaria and diarrhea was indicated by their prescription practices, while utilization of the knowledge was indicated by stocking of malaria and diarrhoea treatment drugs. Equally, knowledge of family planning was indicated by family planning counseling practices, while utilization of the knowledge was represented by stocking of family planning products. Eligible respondents were PPMVs that had attended at least one SFH PPMV training sessions, currently selling family planning/reproductive health, and maternal and child health products, and were willing to participate in the survey.
In each selected location, four research assistants were hired to administer and retrieve questionnaires using personal directory assistants. PPMV locations were identified and grouped together as contiguous as possible for ease of identification and location. Data were analyzed using descriptive statistics and logistic regression methods. All tests were set to be significant at 5% level.
To facilitate the determination of the relationship between training on the one hand, and knowledge acquisition and utilization on the other hand, we present the functional model to be estimated. The model hypothesizes that the provision of quality diarrhoea and malaria treatment, and family planning counseling services depend on the number of trainings received by a PPMV, and the level of educational attainment of the PPMV. Statistically, the model is represented as follows:
 (1)
(1)
 (2)
(2)
where Qi represents a vector of indicators of knowledge of selected healthcare services (diarrhoea, malaria, and family planning services), PT signifies number of training attended by a PPMV,ED stands for education attainment of trained PPMVs, and µt is the error term.
Next, we present the product stocking model. The model hypothesis that stocking of malaria and diarrhoea treatment drugs, as well as family planning products is a function of PPMV training, and location of a PPMV shop. The model is expressed thus:
SKi = ʎo + ʎ1PT + ʎ2LN + α (3)
 (4)
(4)
where SKi represents a vector of stocking of selected healthcare products (co-packaged ORS/Zinc, ACT, and Postinor 2), PT signifies number of trainings attended by a PPMV, while LN represents the location of a PPMV shop, and α is the errorterm.
4. Results
Approximately 3.2% of the responding PPMVs had only primary education, 61.3% attended secondary school, while 35.5% had tertiary education. More PPMVs (61%) operated in the rural area than in the urban area (39%) (Table 1).

Table 1. Social demographics of respondents (percentage).
As shown in Figure 1, about 49.5% of responding PPMVs attended the training once in the past four years, 26% attended twice, while 24.5% attended the training more than twice. In 2014 alone, 84.4% attended the training once, 13.8% attended twice, while 1.8% attended more than twice.
Findings as highlighted in Table 2 show that number of trainings appear to be a factor determining the impact of training on desired outcome. Participating in training for several times appears to be correlated with improvement in the quality of healthcare services offered. This is expected as most of the PPMVs interviewed who participated in the training twice and more than twice over four years were by far more than those who participated twice and more than twice in just one year. Specifically, About 26% of responding PPMVs attended the training twice in the past four years, while 24.5% attended more than twice. In 2014, 13.8% attended twice, while 1.8% attended more than twice.
About 68.2% of PPMVs had adequate knowledge of diarrhea treatment. This varied from 64.4% for those who attended once; 71.8% for those with two trainings and 72.2% for those with more than two trainings. Training attendance was significantly associated with adequate knowledge of diarrhea treatment and knowledge of family planning services. PPMVs who attended the training twice, and those who attended more than twice over the four years were more likely to have adequate knowledge of diarrhea treatment than those who attended only once.
Similarly, adequate knowledge of family planning counseling was 86.4%. This varied from 66.6% for those who attended once; 72.5% for those with two trainings and 73.3% for those with more than two trainings. Within the same four year period, PPMVs who attended training twice and those who attended more than twice were more likely to have adequate knowledge of family planning counseling service than those attending once.
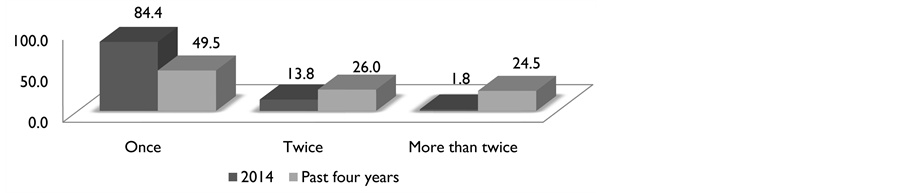
Figure 1. Percentage of respondents who attend training over the past four years.
Table 2. Adequate knowledge of diarrhoea, malaria and family planning services.
***Significant at 5%. **Significant at 10%. Figure in brackets are the confidence intervals.
Although we did not find any significant association between training attendance and adequate knowledge of malaria treatment, overall, the knowledge level for malaria treatment was admitted by 73% of the PPMVs. This varied from 71.4% for those who attended once; 74.4% for those with two and more than two trainings.
Compared with only primary education, PPMVs with secondary and tertiary education were more likely to have adequate knowledge of family planning counseling services. We found no significant association between education attainment and adequate knowledge of diarrhoea, and malaria treatment.
Table 3 presents findings on factors influencing the utilization of knowledge as indicated by stocking of diarrhoea, malaria and family planning products. Participating in the training in the previous year was associated with stocking and selling of diarrhoea, malaria, and family planning products. Specifically, PPMVs who attended twice were more likely to stock and sell co-packaged ORS/Zinc, whereas those who attended more than twice were more likely to stock and sell Postinor 2 than those who attended once.
PPMVs who attended the training twice and those that attended more than twice in four years were more likely to stock and sell co-packaged ORS/Zinc and Postinor 2. The impact of location of shops on stocking and selling of products varied according to product. PPMV in the rural areas were more likely to stock and sell co-packaged ORS/Zinc than those in the urban area, whereas they are less likely to stock and sell Postinor 2. Significant impact of location of shops on stocking and selling of ACT was not found.
5. Discussion
Our findings reveal that PPMV trainings remain a potent tool in building the capacity of PPMVs towards providing improved healthcare services to heir community of care. While PPMV training can be useful in managing some sicknesses, its effectiveness in managing others may be limited. Results from our study indicate that while training attendance exhibits positive and significant association with adequate knowledge of treat of diarrhoea as well as provision of family planning services, it is not associated with adequate knowledge of malaria treatment. Possible explanation for this could stem from the fact that the Nigerian drug market is saturated with assorted kinds of malaria treatment drugs. This provides wide range of treatment options other than the option that represented the possession of the adequate knowledge of malaria treatment in our study. Although the training emphasizes on the use of ACTs (the use of which indicates adequate knowledge of malaria treatment in our study) for malaria treatment, PPMVs are not under compulsion to adopt this treatment option except on request by their client. Even when demand for ACTs is made by clients, its usage depends on availability. Thus, frequent stock-outs of the product also contributes to its low usage by the PPMVs.
Both PPMVs that attended the training twice, and those that attended it more than twice demonstrated adequate knowledge of diarrhoea treatment, and family planning counseling. These findings owes to the new formulation
Table 3. Stocking and selling of product.
***Significant at 5%. **Significant at 10%. Figure in brackets are the confidence intervals.
for diarrhoea treatment (co-packaged ORS/Zinc). The tendency to learn the appropriate usage of this new method and to ensure its adoption by their clients implies that PPMVs should strive to posses its knowledge, and use it for diarrhoea management. Also, the absence of any other known effective alternative to this combined therapy makes its usage inevitable.
On the other hand, current increases in the demand for family planning services make the knowledge of appropriate family planning counseling a market promotion tool and confer a competitive advantage to its possessor. Hence, the tendency for PPMVs to posses adequate knowledge of family planning counseling becomes imperative for their business survival. This finding provides insight on the existence of an ample opportunity for increasing family planning uptake through the PPMVs.
Education attainment of PPMVs also showed a positive correlation with adequate knowledge of family planning counseling. PPMVs with secondary and tertiary education proved to posses adequate knowledge of family planning counseling than those with only primary education. Gaining post-primary educational qualification remains important for proper understanding of the training module. As a policy concern, government licensing of PPMV should be dependent, among other considerations, on the educational attainments of prospective PPMVs [12] .
Just like possession of adequate knowledge for the treatment of diarrhoea, malaria, and family planning counseling, training attendance is significantly associated with utilization of knowledge of only diarrhoea, and family planning products. This finding corroborates that of [2] . The authors had reported that about 89.9% of PPMV shops in two Nigerian states stocked (utilized their knowledge) oral rehydration solution (ORS) for treatment of diarrhoea. PPMVs with two or more trainings stocked and sold those products than those who trained once. Increasing the frequency of training can be helpful in enhancing accessibility and coverage of product distribution [13] . Stocking and selling of products as well as possessing adequate knowledge of the correct treatment makes PPMVs an effective platform for optimum healthcare delivery, and this depends on their continuous training [14] .
Location of PPMV shops plays critical role in the stocking and sell of products. PPMV shops in rural areas are more likely to stock and sell co-packaged ORS/Zinc. This may be attributed to the widespread cases of diarrhoea in the rural areas. On the other hand, PPMV shops in rural areas were less likely to stock and sell Postinor 2 than those in the urban area. Being unaware of the availability of family planning products, as well as constant stock-outs of those products in the rural areas may have accounted for this result.
6. Conclusion
Refresher trainings for PPMVs have the effect of increasing the level of knowledge and practices in some area including appropriate prescription practices for diarrhea treatment and family planning counseling. Interventions to reduce the burden of disease and mortality in Nigeria must recognize the important role drug retailers play in delivering basic healthcare services. In Nigeria, owner-operated drug retail outlets are a main source of medicines for acute conditions, but their practices are not well understood. Greater understanding of the role of PPMVs and the quality of care they provide is needed in order to inform on-going national health initiatives that aim to streamline PPMVs into the national primary healthcare delivery system.
Cite this paper
Chukwunonso Iheoma,Babajide Daini,Suliatu Lawal,Mukhtar Ijaiya,Wole Fajemisin, (2016) Impact of Patent and Proprietary Medicine Vendors Training on the Delivery of Malaria, Diarrhoea, and Family Planning Services in Nigeria. Open Access Library Journal,03,1-10. doi: 10.4236/oalib.1102404
References
- 1. National Population Commission (NPC) [Nigeria] and ICF Macro (2009) Nigeria Demographic and Health Survey 2013. National Population Commission and ICF Macro, Abuja.
- 2. Treleaven, E., Liu, J., Prach, L.M. and Isiguzo, C. (2015) Seeking at Patent and Proprietary Medicine Vendors in Nigeria. BMC Health Services Research, 15, 231.
http://dx.doi.org/10.1186/s12913-015-0895-z - 3. Nsimba, S.E. (2007) Assessing the Performance, Practices and Roles of Drug Sellers/Dispensers and Mothers’/Guar-dians’ Behaviour for Common Childhood Conditions in Kibaha District, Tanzania. Tropical Doctor, 37, 197-201.
http://dx.doi.org/10.1258/004947507782333099 - 4. Ujuju, C., et al. (2014) An Assessment of the Quality of Advice Provided by Patent Medicine Vendors to Users of Oral Contraceptive Pills in Urban Nigeria. Journal of Multidisciplinary Healthcare, 7, 163-171.
- 5. Akuse, R.M., Eseigbe, E.E., Ahmed, A. and Brieger, W.R. (2010) Patent Medicine Sellers: How Can They Help Control Childhood Malaria? Malaria Research and Treatment, 2010, 1-7.
http://dx.doi.org/10.4061/2010/470754 - 6. Hetzel, M.W. (2008) Malaria Treatment in the Retail Sector: Knowledge and Practices of Drug Sellers in Rural Tanzania. BMC Public Health, 8, 157.
http://dx.doi.org/10.1186/1471-2458-8-157 - 7. Rosamund, M.A., Eseigbe, E.E., Ahmed, A. and Brieger, W.R. (2010) Patent Medicine Sellers: How Can They Help Control Childhood Malaria? Malaria Research and Treatment, 2010, Article ID: 470754.
- 8. Oladepo, O., et al. (2011) Awareness of Anti-Malarial Policy and Malaria Treatment Practices of Patent Medicine Vendors in Three Nigerian States. African Journal of Medical Sciences, 40, 345-352.
- 9. Ajayi, I.O., Soyannwo, T. and Akpa, O.M. (2013) Awareness and Utilization of Affordable Medicine Facility-Malaria among Caregivers of Under-Five Children in Ibadan North-West Local Government Area, Oyo State. Malaria Research and Treatment, 2013, Article ID: 176096.
http://dx.doi.org/10.1155/2013/176096 - 10. Brieger, R.W., et al. (2004) Strengthening Patent Medicine Vendors’ Associations in Nigeria for Improved Malaria Management. Health Policy and Planning, 19, 177-182.
http://dx.doi.org/10.1093/heapol/czh021 - 11. Liu, J., Isiguzo, C. and Sieverding, M. (2015) Differences in Malaria Care Seeking and Dispensing Outcomes for Adults and Children Attending Drug Vendors in Nasarawa, Nigeria. Tropical Medicine & International Health, 20, 1081-1092.
http://dx.doi.org/10.1111/tmi.12520 - 12. Brieger, W., Unwin, A., Greer, G. and Meek, S. (2005) Interventions to Improve the Role of Medicine Sellers in Malaria Case Management for Children in Africa. London, UK and Arlington, VA, USA: The Malaria Consortium and BASICS for the United States Agency for International Development; Prepared for Roll Back Malaria’s Sub-Group for Communication and Training and Malaria Case Management Working Group.
- 13. Ikeoluwapo, O.A., Soyannwo, T. and Akpa, O.M. (2013) Awareness and Utilization of Affordable Medicine Facility-Malaria among Caregivers of Under-Five Children in Ibadan North-West Local Government Area, Oyo State. Malaria Research and Treatment, 2013, Article ID: 176096.
- 14. Beyeler, N., Liu, J. and Sieverding, M. (2015) A Systematic Review of the Role of Proprietary and Patent Medicine Vendors in Healthcare Provision in Nigeria.
www.researchgate.net/journal/1932-6203_PLoS_ONE
NOTES

*Corresponding author.