K. TERAMOTO ET AL.361
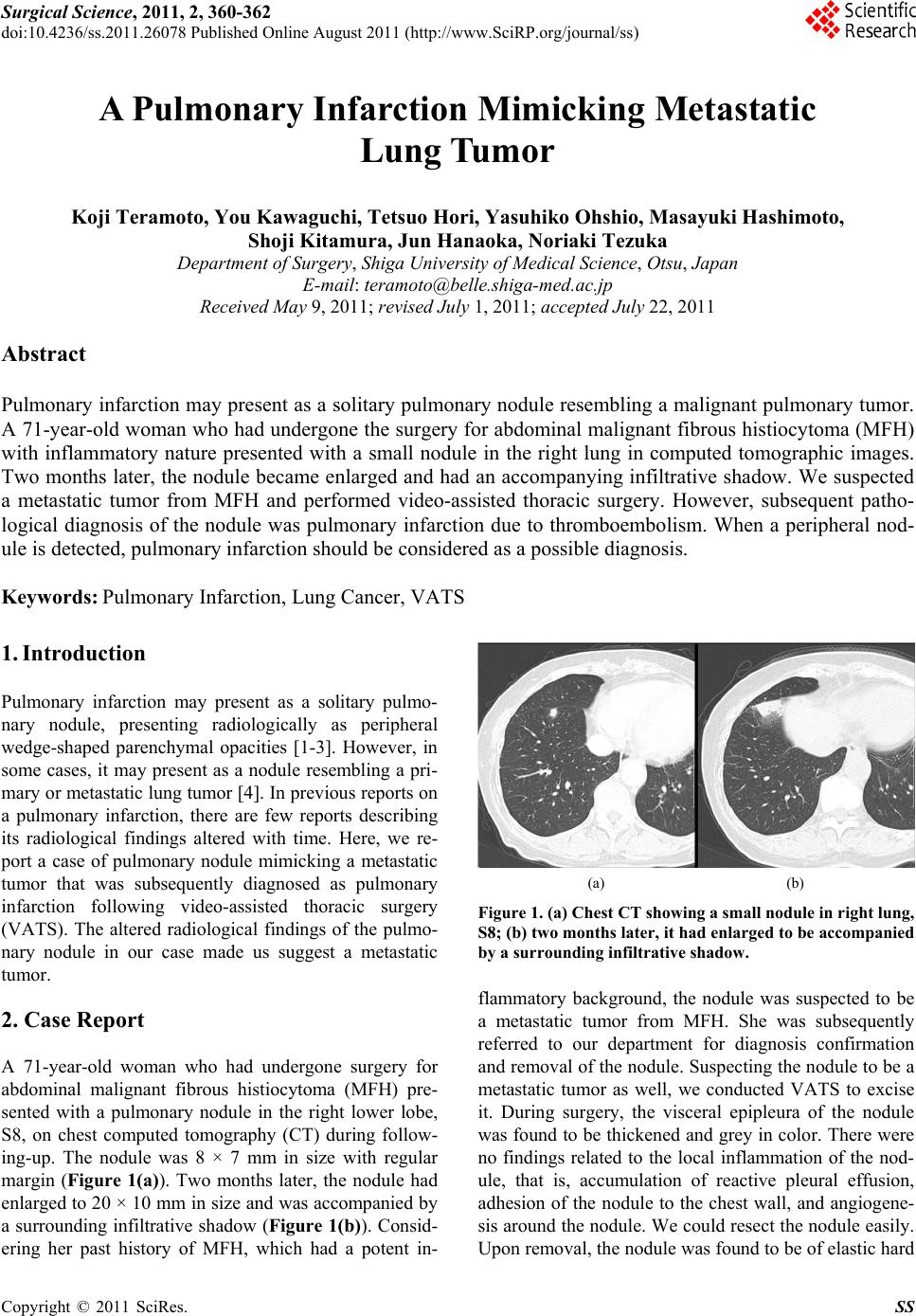
consistency and 20 × 20 × 15 mm in size. The cut sur-
face of the nodule was dark red in color (Figure 2(a))
and it was pathologically diagnosed as a pulmonary in-
farction caused by thromboembolism (Figure 2(b)). Ma-
lignant cells were not detected in the resected specimen.
3. Discussion
Pulmonary infarctions typically result from pulmonary
thromboembolism. Other than this, non-thromboembolic
causes of pulmonary infarctions include pulmonary in-
fections, diffuse alveolar damage, pulmonary torsion,
lung cancer, amyloidosis, bronchial artery embolization
therapy, and intravenous catheter embolization [5]. In
this case, pulmonary infarctions resulted from pulmonary
thromboembolism but causes of thrombus were not fully
revealed. The patient had lower risk to occur the throm-
bus, that is, she had neither varix of the lower limb nor
atrial fibrillation. And sh e took an or al anti-co ag lant drug
(a)
(b)
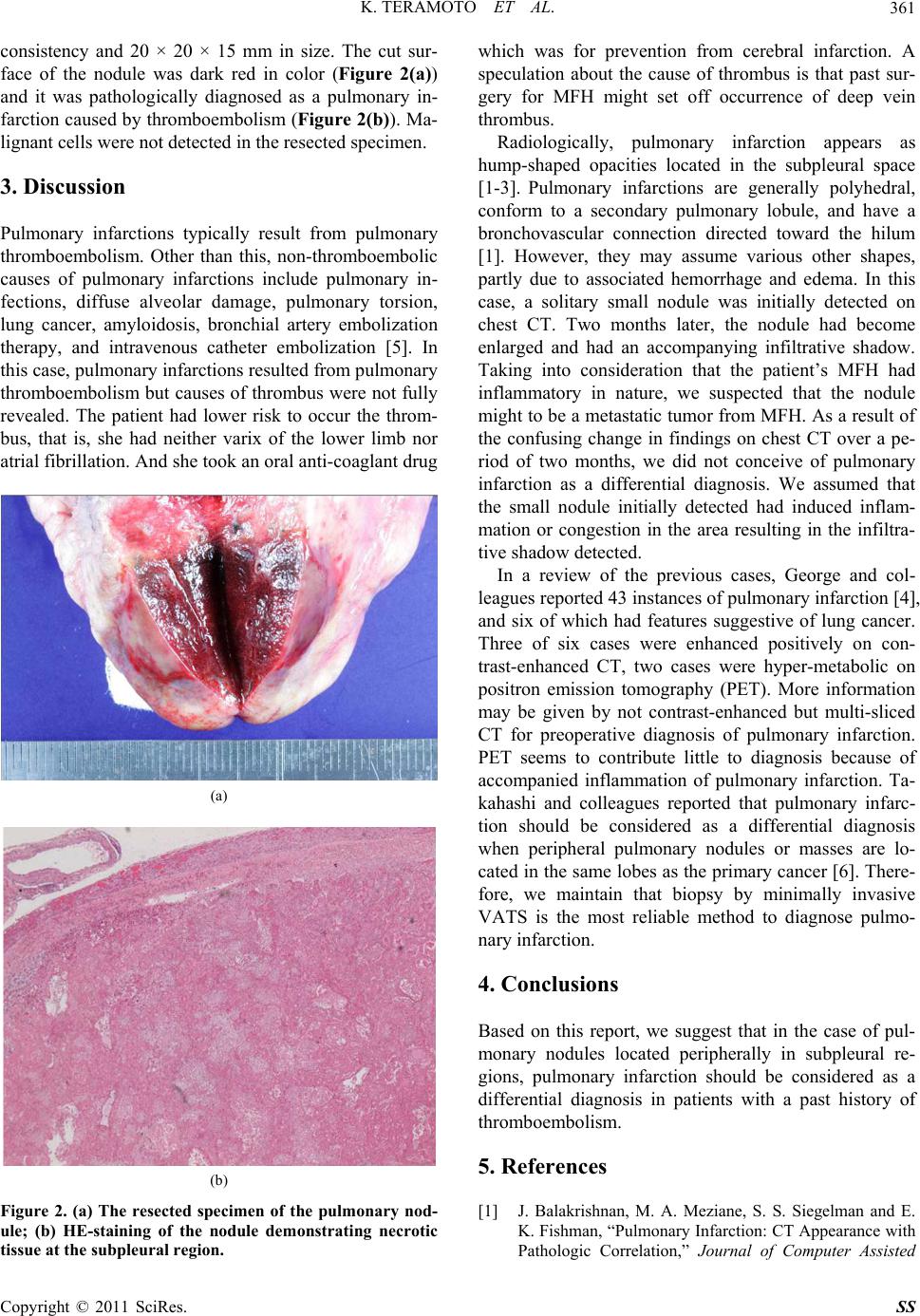
Figure 2. (a) The resected specimen of the pulmonary nod-
ule; (b) HE-staining of the nodule demonstrating necrotic
tissue at the subpleural region.
which was for prevention from cerebral infarction. A
speculation about the cause of thrombus is that past sur-
gery for MFH might set off occurrence of deep vein
thrombus.
Radiologically, pulmonary infarction appears as
hump-shaped opacities located in the subpleural space
[1-3]. Pulmonary infarctions are generally polyhedral,
conform to a secondary pulmonary lobule, and have a
bronchovascular connection directed toward the hilum
[1]. However, they may assume various other shapes,
partly due to associated hemorrhage and edema. In this
case, a solitary small nodule was initially detected on
chest CT. Two months later, the nodule had become
enlarged and had an accompanying infiltrative shadow.
Taking into consideration that the patient’s MFH had
inflammatory in nature, we suspected that the nodule
might to be a metastatic tumor fro m MFH. As a result of
the confusing change in findings on chest CT over a pe-
riod of two months, we did not conceive of pulmonary
infarction as a differential diagnosis. We assumed that
the small nodule initially detected had induced inflam-
mation or congestion in the area resulting in the infiltra-
tive shadow detected.
In a review of the previous cases, George and col-
leagues reported 43 instances of pulmonary infarction [4],
and six of which had features suggestive of lung cancer.
Three of six cases were enhanced positively on con-
trast-enhanced CT, two cases were hyper-metabolic on
positron emission tomography (PET). More information
may be given by not contrast-enhanced but multi-sliced
CT for preoperative diagnosis of pulmonary infarction.
PET seems to contribute little to diagnosis because of
accompanied inflammation of pulmonary infarction. Ta-
kahashi and colleagues reported that pulmonary infarc-
tion should be considered as a differential diagnosis
when peripheral pulmonary nodules or masses are lo-
cated in the same lobes as the primary cancer [6]. There-
fore, we maintain that biopsy by minimally invasive
VATS is the most reliable method to diagnose pulmo-
nary infarction.
4. Conclusions
Based on this report, we suggest that in the case of pul-
monary nodules located peripherally in subpleural re-
gions, pulmonary infarction should be considered as a
differential diagnosis in patients with a past history of
thromboembolism.
5. References
[1] J. Balakrishnan, M. A. Meziane, S. S. Siegelman and E.
K. Fishman, “Pulmonary Infarction: CT Appearance with
Pathologic Correlation,” Journal of Computer Assisted
Copyright © 2011 SciRes. SS