Paper Menu >>
Journal Menu >>
 Surgical Science, 2011, 2, 248-251 doi:10.4236/ss.2011.25055 Published Online July 2011 (http://www.SciRP.org/journal/ss) Copyright © 2011 SciRes. SS Surgical Technique Used for Portal Vein Thrombosis when Thrombectomy is not Possible during Liver Transplantation José Roberto Alves1, Ilka de Fátima Santana Ferreira Boin2, Anaísa Portes Ramos3, Catherine Puliti Hermida Reigada3, Ne lso n Caserta2, Adilson Roberto Cardoso2, Cristina Arrivabene Caruy2, Elaine Cristina Ataíde1, Jazon Romilson Souza Almeida2 1Surgical Scie n ces , Facul t y of Medi cal Sci e nc es, State Unive rsi t y of Campinas, Campinas, Brazil 2Unit of Liver Transplantation, Faculty of Medical Scienc es, State University of Campinas, Campinas, Brazil 3Unit of Liver Transplantation, Faculty of Medical Scienc es, State University of Campinas, Campinas, Brazil E-mail: ilkaboin@yahoo.com Received April 26, 2011; revised May 28, 2011; accepted June 13, 2011 Abstract Portal vein thrombosis (PVT) was for a long time considered a barrier to liver transplantation. The aim of this study is to demonstrate the surgical technical options for portal vein reconstruction during liver trans- plantation in patients with PVT in which thrombectomy was not possible. Between September 1991 and March 2009, 420 liver transplanted patients were retrospectively analyzed, identifying 29 cases with PVT (6.9%). Preoperative diagnosis, preoperative risk factors, surgical technique options to treat various forms (grades) of PVT, postoperative recurrence and actuarial survival rates were studied. In three cases of PVT grade II and in one case PVT grade III the thrombectomy was insufficient, requiring some surgical technique options (13.79%). In two cases placement of iliac vein graft was performed, in one an anastomosis of the portal vein with collateral splenorenal vein and in the other with left gastric varicose. The actuarial survival rate for patients without PVT and patients with PVT and effective thrombectomy was 73.8% while those with PVT who needed some type of surgical option was 75%. Our results suggest that actuarial survival rates were similar among patients with PVT or PVT with effective thrombectomy when compared with PVT that required some surgical options. Keywords: Liver Transplantation, Portal Vein Thrombosis, Surgical Technique 1. Introduction Portal vein thrombosis (PVT) is an entity that occurs in the general population at around 1% and may be caused by a variety of conditions including cirrhosis, cancer, myeloproliferative diseases, inflammation, and abdomi- nal infection, among others [1,2]. Considering cirrhotic patients with worsening liver function (expressed by Child- Pugh score) it may occur in up to 26% [3] of the patients and when concomitant to the hepatocellular carcinoma it can reach 44% [2]. In patients who are being prepared for liver transplantation it might affect between 5 and 15% [4-12]. When we find PVT during a surgery in its various grades, often due to low sensitivity of tests performed p re - operatively, the surg eon is fa c ed with a co nd ition in wh ich various surgical strategies may need to be used: throm- bectomy, use of graft (autologous or heterologous), an- astomosis with collateral vessels to bypass so me obstruct tion or maybe a cavoportal he mitransposition will enable a successful orthotopic liver transplantation (OLT) [8, 12-20]. Therefore, the aim of this study is to retrospec- tively review our experience of performing OLT in order to demonstrate the surgical technical options for v ein po r- tal reconstruction in patients with PVT when thrombec- tomy is not possible, as well as to compare actuarial sur- vival among pat ients without PVT, thos e with successful thrombectomy or patients with PVT who needed some type of surgical opti ons for port al vein reconstructi on. 2. Methods This is a retrospective observational study of 420 pa- 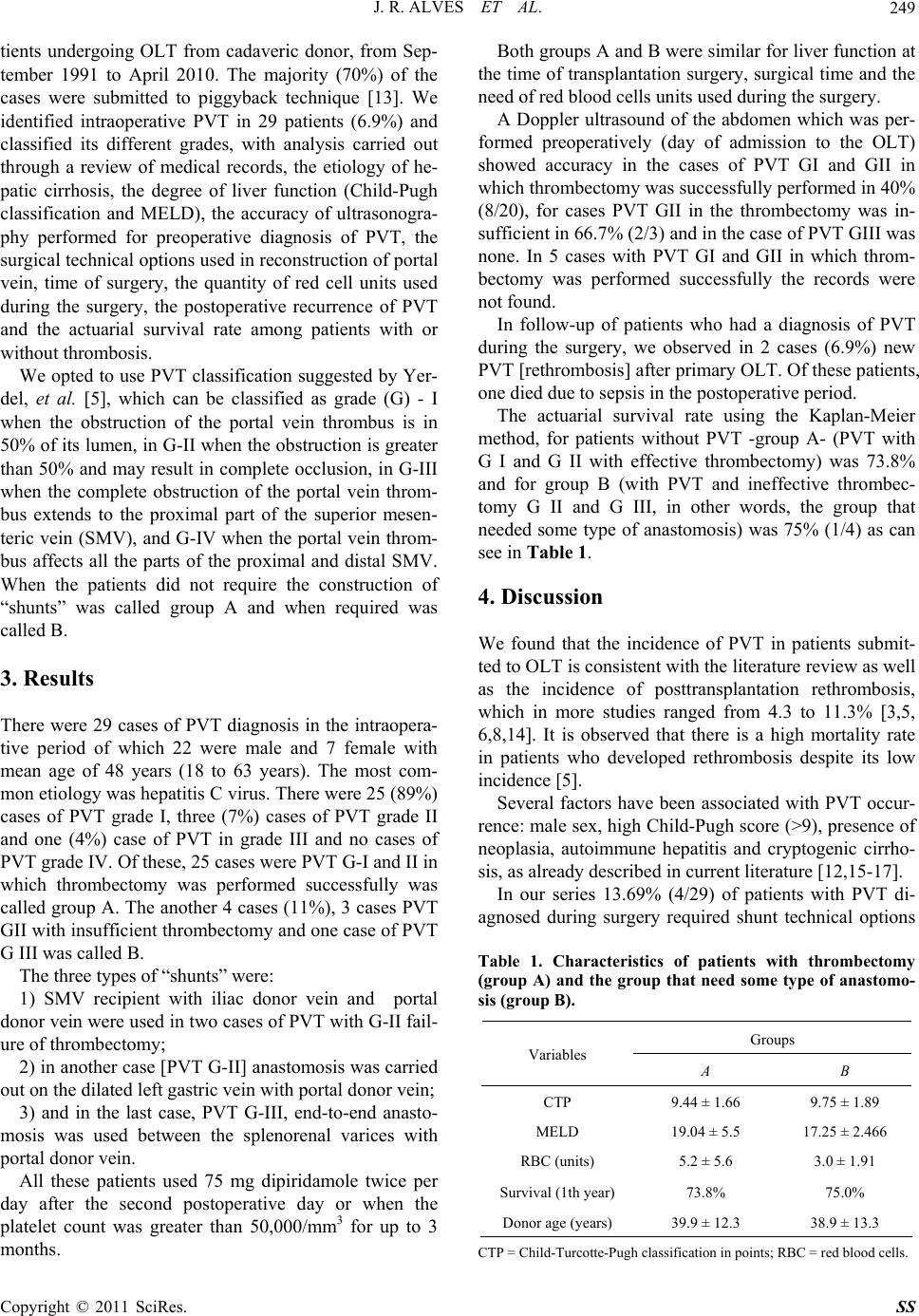 J. R. ALVES ET AL. Copyright © 2011 SciRes. SS 249 tients undergoing OLT from cadaveric donor, from Sep- tember 1991 to April 2010. The majority (70%) of the cases were submitted to piggyback technique [13]. We identified intraoperative PVT in 29 patients (6.9%) and classified its different grades, with analysis carried out through a review of medical records, the etiology of he- patic cirrhosis, the degree of liver function (Child-Pugh classification and MELD), the accuracy of ultrasonogra- phy performed for preoperative diagnosis of PVT, the surgical technical options used in reconstruction of portal vein, time of surgery, the quantity of red cell units used during the surgery, the postoperative recurrence of PVT and the actuarial survival rate among patients with or without thrombosis. We opted to use PVT classification suggested by Yer- del, et al. [5], which can be classified as grade (G) - I when the obstruction of the portal vein thrombus is in 50% of its lumen, in G-II when the obstruction is greater than 50% and may result in complete occlusion, in G-III when the complete obstruction of the portal vein throm- bus extends to the proximal part of the superior mesen- teric vein (SMV), and G-IV when the portal vein throm- bus affects all the parts of the proximal and distal SMV. When the patients did not require the construction of “shunts” was called group A and when required was called B. 3. Results There were 29 cases of PVT diagnosis in the intraopera- tive period of which 22 were male and 7 female with mean age of 48 years (18 to 63 years). The most com- mon etiology was hepatitis C viru s. There were 2 5 (89%) cases of PVT grade I, three (7%) cases of PVT grade II and one (4%) case of PVT in grade III and no cases of PVT grad e IV . Of th e s e, 25 cas es we r e PV T G- I and II in which thrombectomy was performed successfully was called group A. The another 4 cases (11%), 3 cases PVT GII with insufficient thrombectomy and one case of PVT G III was called B. The three types of “shunts” were: 1) SMV recipient with iliac donor vein and portal donor vein were used in two cases of PVT with G-II fail- ure of thrombectomy; 2) in another case [PVT G-II] anastomosis was carried out on the dilated left gastric vein with portal donor vein; 3) and in the last case, PVT G-III, end-to-end anasto- mosis was used between the splenorenal varices with portal donor vein. All these patients used 75 mg dipiridamole twice per day after the second postoperative day or when the platelet count was greater than 50,000/mm3 for up to 3 months. Both groups A and B were similar for liver function at the time of transplan tation surgery, surgical time and the need of red blood cells units used dur ing the surgery. A Doppler ultrasound of the abdomen which was per- formed preoperatively (day of admission to the OLT) showed accuracy in the cases of PVT GI and GII in which thrombectomy was successfully p erformed in 40 % (8/20), for cases PVT GII in the thrombectomy was in- sufficient in 66.7% (2/3) and in the case of PVT GIII was none. In 5 cases with PVT GI and GII in which throm- bectomy was performed successfully the records were not found. In follow-up of patients who had a diagnosis of PVT during the surgery, we observed in 2 cases (6.9%) new PVT [rethrombosis] after primary OLT. Of these p atients, one died due to sepsis in the postoperative period. The actuarial survival rate using the Kaplan-Meier method, for patients without PVT -group A- (PVT with G I and G II with effective thrombectomy) was 73.8% and for group B (with PVT and ineffective thrombec- tomy G II and G III, in other words, the group that needed some type of anastomosis) was 75% (1/4) as can see in Table 1. 4. Discussion We found that the incidence of PVT in patients submit- ted to OLT is consistent with the literature review as well as the incidence of posttransplantation rethrombosis, which in more studies ranged from 4.3 to 11.3% [3,5, 6,8,14]. It is observed that there is a high mortality rate in patients who developed rethrombosis despite its low incidence [5]. Several factors have been associated with PVT occur- rence: male sex, high Child-Pugh score (>9), presence of neoplasia, autoimmune hepatitis and cryptogenic cirrho- sis, as already described in current literature [12,15-17]. In our series 13.69% (4/29) of patients with PVT di- agnosed during surgery required shunt technical options Table 1. Characteristics of patients with thrombectomy (group A) and the group that need some type of anastomo- sis (group B). Groups Variables A B CTP 9.44 ± 1.66 9.75 ± 1.89 MELD 19.04 ± 5.5 17.25 ± 2.466 RBC (units) 5.2 ± 5.6 3.0 ± 1.91 Survival (1th year) 73.8% 75.0% Donor age (years ) 39.9 ± 12.3 38.9 ± 13.3 CTP = Child-Turcotte-Pugh classification in points; RBC = red blood cells.  J. R. ALVES ET AL. Copyright © 2011 SciRes. SS 250 due to thrombectomy failure. As is known, there is a tendency to try the thrombec- tomy procedure first before using the venous anastomo- sis technique option that could be performed for different degrees of PVT. Apparently, the first option is throm- bectomy when related to PVT GI and GII; in PVT GIII the use of grafts (interposition with iliac vein graft)] could be needed and in GIV an anastomosis to the splanchnic tributaries may be needed or even a cavopor- tal hemitransposition. This was proposed firstly by Tza- kis et al. [4,7-9]. It is valid to emphasize that in our study the 3 cases of PVT GII, 10.34% (3/29) and another PVT GIII required some kind of “shunt” anastomosis. There- fore, we can see that it is difficult to standardize a tech- nical option. It is recommended that surgeons who choose to act in this area of liver transplantation know all the technical options available to choose the best proce- dure in every case. Despite our small sample, only 4 cases of PVT required an option to “shunt”. It can be seen that the option of the use of autologous grafting of iliac vein was safe and feasible, and there was no nega- tive impact on patient surv ival [11]. Usually the ultrasound was performed in the pre-op- erative transplantation time. It was shown with low ac- curacy to detect PVT [14,15]. Classic studies such as Yerdel et al. [5] have demonstrated a great sensitivity to the method as the most advanced degree of PVT, reach- ing values of 100% in cases of PVT GIII and GIV. In this study we could not verify similar results in our sam- ple. Perhaps the justification for medical ultrasound has not identified the case for PVT GIII, despite the absence of portal flow, which is due to the presence of large as- citis, a great collateral circulation or the presence of in- testinal gases observed in those patients. The four patients with PVT that required some kind of “shunt” had good liver function after the transplantation procedure and no statistically significant difference in the time of surgery or blood requirement units during the surgery were observed. This was d escribed by Tao et al. [6], although other stud ies have demonstrated the longest operative time or the greater necessity for red blood cell transfusion in such cases [3,10,14,18-20]. The actuarial survival rate for the patien ts submitted to a venous shunt was 75%. There was no statistical differ- ence between patients without PVT or those with PVT GI and GII with successful thrombectomy or patients PVT GII and GIII who required some type of “shunt”, as already observed in other studies [6,10,18-20]. In conclusion, we confirm that the surgical technical options with or without the use of grafts are feasible and portal venous reconstr uction in patients with and without PVT grade I, II and III showed similar survival rates de- spite shunt requirements during the surgery. 5. References [1] M. Ogren, D. Bergqvist, M. Bjorck, S. Acosta, H. Eriks- sonet and N. H. Sternby, “Portal Vein Thrombosis: Pre- valence, Patient Characteristics and Lifetime Risk—A Population Study Base on 23796 Consecutive Autopsies,” World Journal of Gastroenterol, Vol. 12, No. 13, 2006, pp. 2115-2119. [2] J. Hoekstra and H. L. A. Janssen, “Vascular Liver Disorders: Portal Vein Thrombosis,” Netherlands Journal of Medici ne, Vol. 67, No. 2, 2009, pp. 46-52. [3] J. Lendoire, G. Raffin, N. Cejas, F. Duek, P. Barros Schelotto, P. Trigo, et al., “Liver Transplantation in Adult Patients with Portal Vein Thrombosis: Risk Factors, Ma- nagement and Outcome,” The Official Journal of the International Hepato Pancreato Biliary, Vol. 9, No. 5, 2007, pp. 352-356. [4] R. Charco, et al., “Portal Vein Thrombosis in Liver Transplantation,” Transplantation Proceedings, Vol. 37, No. 9, 2005, pp. 3904-3905. doi:10.1016/j.transproceed.2005.09.120 [5] M. A. Yerdel, et al., “Portal Vein Thrombosis in Adults Undergoing Liver Transplantation,” Transplantation, Vol. 69, No. 9, 2000, pp. 1873-1881. doi:10.1097/00007890-200005150-00023 [6] Y. F. Tao, et al., “Liver Transplant Recipients with Portal Vein Thrombosis: A Single Center Retrospective Study,” Hepatobiliary & Pancreatic Diseases International, Vol. 8, No. 1, 2009, pp. 34-39. [7] R. Robles, et al., “Eversion Thromboendovenectomy in Organized Portal Vein Thrombosis during Liver Trans- plantation,” Clinical Transplantation, Vol. 18, No. 1, 2004, pp. 79-84. doi:10.1111/j.1399-0012.2004.00120.x [8] M. Paskonis, et al., “Surgical Strategies for Liver Trans- plantation in the Case of Portal Vein Thrombosis – Cur- rent Role of Cavoportal Hemitransposition and Renopor- tal Anastomosis,” Clinical Transplantation, Vol. 20, No. 5, 2006, pp. 551-562. doi:10.1111/j.1399-0012.2006.00560.x [9] C. Pan, et al., “Single-Center Experience of 253 Portal Vein Thrombosis Patients Undergoing Liver Transplanta- tion in China,” Transplantation Proceedings, Vol. 41, No. 9, 2009, pp. 3761-3765. doi:10.1016/j.transproceed.2009.06.215 [10] L. Lladó, et al., “Management of Portal Vein Thrombosis in Liver Transplantation: Influence on Morbidity and Mortality,” Clinical Transplantation, Vol. 21, No. 6, 2007, pp. 716-721. [11] D. Nikitin, et al., “Twenty Years’ Follow-Up of Portal Vein Conduits in Liver Transplantation,” Liver Trans- plantation, Vol. 5, No. 4, 2009, pp. 400-406. doi:10.1002/lt.21698 [12] J. Dumortier, et al., “Eversion Thrombectomy for Portal Vein Thrombosis During Liver Transplantation,” Ameri- can Journal of Transplantation, Vol.2, No.10, 2002, pp. 934-938. doi:10.1034/j.1600-6143.2002.21009.x [13] A. Tzakis, S. Todo and T. E. Starzl, “Orthotopic Liver Transplantation with Preservation of the Inferior Vena  J. R. ALVES ET AL. Copyright © 2011 SciRes. SS 251 Cava,” Annals of Surgery, Vol. 21, No. 6, 1989, pp. 649-652. doi:10.1097/00000658-198911000-00013 [14] G. Manzanet, et al., “Liver Transplantation in Patients with Portal Vein Thrombosis,” Liver Transplantation, Vol. 7, No. 2, 2001, pp. 125-131. doi:10.1053/jlts.2001.21295 [15] A. C. Stieber, et al., “The Spectrum of Portal Vein Thrombosis in Liver Transplantation,” Annals of Surgery, Vol. 213, No. 3, 1991, pp. 199-206. doi:10.1097/00000658-199103000-00003 [16] B. R. Davidson, M. Gibson, R. Dick, A. Burroughs and K. Rolles, “Incidence, Risk Factors, Management, and Out- come of Portal Vein Abnormalities at Orthotopic Liver Transplantation,” Transplantation, Vol. 57, No. 8, 1994, pp. 1174-1177. doi:10.1097/00007890-199404270-00006 [17] R. Quarrie and S. P. Stawicki, “Portal Vein Thrombosis: What Surgeons Need to Know,” OPUS 12 Scientist, Vol. 2, No. 3, 2008, pp. 30-33. [18] B. Pérez-Saborido, et al., “Incidence, Management, and Results of Vascular Complications after Liver Transplan- tation,” Transplantation Proceedings, Vol. 43, No. 3, 2011, pp. 749-750. doi:10.1016/j.transproceed.2011.01.104 [19] M. Ravaioli, et al., “Portal Vein Thrombosis and Liver Transplantation: Evolution during 10 Years of Experi- ence at the University of Bologna,” Annals of Surgery, Vol. 253, No. 2, 2011, pp. 378-384. doi:10.1097/SLA.0b013e318206818b [20] A. P. Ramos, et al., “Portal Vein Thrombosis and Liver Transplantation: Long Term,” Transplantation Proceed- ings, Vol. 42, No. 2, 2010, pp. 498-501. doi:10.1016/j.transproceed.2010.01.038 |