The Impact of a Drug Safety Warning on Discussions Between Doctors and Their Patients; the Case of Rosiglitazone 171
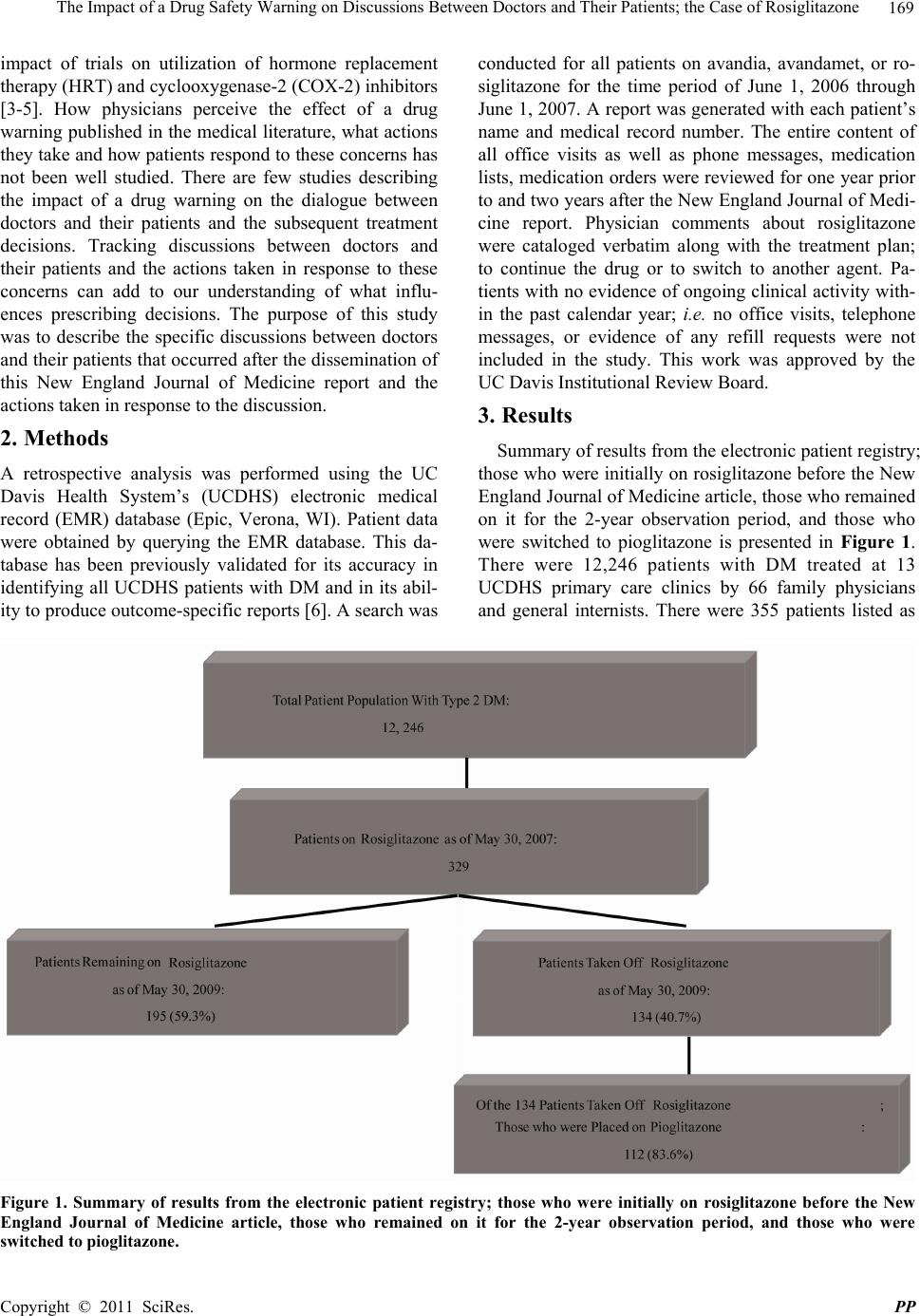
article. For the 40.7 percent who were switched to an-
other medication, the most common theme abstracted
from the comments was that the patient was concerned
about the reports and preferred to make the change.
The timeframe of response and decline in use of rosig-
litazone in this study is similar to that reported in studies
of other medications after reports of concerning adverse
side effects. Previous work on reports of adverse events
related to calcium channel blockers in the setting of
myocardial infarction demonstrated a 20 percent reduc-
tion of the use of this class of medications within months
of the published report [7]. A similarly rapid, but larger
reduction (66 percent) in the use of Prempro was noted
over a 6-month period after reports of increased risk of
breast cancer and cardiovascular disease were linked
with estrogen/progestin combination therapy [3].
Another important finding from this study is how phy-
sicians’ perceive a drug side effect as being unique to the
drug and not class specific. The majority of patients who
were changed to another medication were placed on
pioglitazone. Given this information, it seems likely that
many providers felt that this is not a class effect. This
finding is supported by a recent study by Cohen and as-
sociates [8]. They found that while rosiglitazone use de-
clined sharply from 0.42 million monthly treatment visits
(February 2007) to 0.13 million monthly treatment visits
(May 2008); pioglitazone use remained stable. Given
that the FDA adviso ry was “class-level” for these agen ts,
it is unclear how physicians ca me to make the distinction
between rosigl it azone a n d pi o gl it azone.
Following the patients over a 2-year period demon-
strated that there was little change over time for those
who were advised to continue rosiglitazone. However,
there were few new starts of rosiglitazone. Only 4 pa-
tients on the registry were started on this drug during the
two-year period observation period; from June 14, 2007
through June 14, 2009. Again, this is consistent with the
findings of Cohen and associates [8].
This study has a number of limitations. The informa-
tion was abstracted from the medical records and relied
on documentation. It is likely that this led to underre-
porting of discussions between doctors and their patients.
This study cannot reliably determine the source of in-
formation which led to the discussion. Some of the ab-
stracted comments attributed to patients’ suggest that
concerns solely came from the newsmedia; however,
there may have been other sources that prompted patients
to express their concerns; e.g. family members, pharma-
cists, and the internet. This study cannot determine the
extent of concern exhibited by the patient to the provider
and the extent to which that influenced the physician’s
response. Further, there may have been other characteris-
tics of patients such as age, gender, ethnicity, socioeco-
nomic status, level of diabetes control, and prior treat-
ments which could have influenced the physician’s re-
sponse to these concerns. Length of use may also play a
role. Patients on rosiglitazone for longer periods of time
with no adverse side effects may perceive their risk for
harm differently. This response was described by Faber
and associates in their study on the influence of studies
on harm associated with HRT [9]. Specifically, long-
term HRT users were less likely to discontinue their
medication. This study could not determine the role of
style differences among physicians in the outcome of this
study. While all providers were primary care physicians;
i.e. family physicians and general internists; it is likely
that these physicians view risk and assess the literatu re in
a different manner or are more strongly influenced by
other sources; e.g. opinions of colleagues, specialists, or
pharmaceutical representatives. Again, this study could
not determine how the decision was finally made. It ap-
pears that many patient concerns were met with recom-
mendations to continue the drug.
This study also provides important lessons learned for
future research on the practice effects when faced with
the report of potential harm. There is a need for more
research on the factors which influence decision-making
and the role of the patient in this process. For example,
the documented comments suggest that patients were the
ones who initiated the discussion about adverse side ef-
fects with their providers in many of these cases. How-
ever, the majority of patients remained on rosiglitazone.
This finding is somewhat contrary to the findings of prior
research on how patients influence physicians. Kravitz
and associates demonstrated that patients may have a
substantial influence on physicians prescribing behavior
[10]. In this community-based randomized trail, antide-
pressants were prescribed far more often when standard-
ized patients requested them. This might potentially
mean that there is a different perception among physi-
cians in starting versus discontinuing a medication.
Future research should also consider the influence of
the media; including the journal source. High impact
journals are perceived as having more influence on pro-
viders. While the impact factor was not intended to be a
marker for likelihood of practice change, this study
brings into focus the question of what sources a physi-
cian trusts when concerns for harm are reported and
warrants further investigation [11]. The expansion in use
of social media Web sites, the credibility of this informa-
tion, and how it may influence doctor/patient discussions
also warrants further investigat i on.
Finally, future research should assess the influence of
consensus statements by specialty organizations and
warnings by the Food and Drug Administration (FDA).
For example, despite statements from the American Di-
Copyright © 2011 SciRes. PP