 Pharmacology & Pharmacy, 2011, 2, 101-108 doi:10.4236/pp.2011.23013 Published Online July 2011 (http://www.scirp.org/journal/pp) Copyright © 2011 SciRes. PP 101 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients Ehab Said El-Desoky, Ashraf M. A. El-Tantawy, Yasser M. Raya, Abdulhameed Al-Yahya Pharmacology Department, Faculty of Medicine, Assiut University, Asyut, Egypt. Email: ehegypt@yahoo.com, ehegypt@gmail.com Received January 14th, 2011; revised March 5th, 2011; accepted May 15th, 2011. ABSTRACT Background: Amphetamines are illicit psychostimulant drugs that can induce psychotic symptoms. Very few studies have been conducted in Kingdom of Saudi Arabia (SA) on amphetamine abuse and related psychosis. Recently, the pat- tern of amphetamine abuse in SA showed a significant trend of increased frequency. Objectives: To investigate the ex- tent of amphetamine abuse in a sample of Saudi patients hospitalized for first episode of acute psychosis. Also, to com- pare in that sample between amphetamine psychosis and other psychoses regarding demographic data, premorbid per- sonality and symptoms profile. Method: 106 patients with acute psychosis were hospitalized and screening of urine for amphetamine was conducted for all. Patients’ psychiatric evaluation included interviewing, and ICD-10 criteria for personality disorders. 30 healthy subjects were also included for comparison with patients. Results: 34/106 of psychotic patients (32%) were positive for amphetamine in urine (≥ 1000 ng/ml). The frequency of personality disorders was sig- nificantly higher (P < 0.01) in the patients (54/106; 51%) compared with healthy subjects (6/30; 20%). Also, the inci- dence of personality disorders was significantly higher (P < 0.01) in amphetamine positive psychosis (25/34; 73.5%) compared with amphetamine negative psychosis (29/72; 40%). Cluster B personality disorders particularly the antiso- cial and borderline were significantly higher in amphetamine positive psychosis (13/34; 38%) compared with am- phetamine negative psychoses (6/72; 8%). The symptom profile showed significant difference between amphetamine positive and amphetamine negative psychosis as regards ideas of reference (50% vs. 14%), suspiciousness (44% vs. 11%), suicidal ideation (38% vs. 23%), paranoid delusions (29% vs. 17%) and increased pulse or blood pressure (29% vs. 7%) respectively. Conclusion: Screening of amphetamine in urine among patients with first episode of acute psycho- sis can help and support the clinical distinction of amphetamine psychosis from other types of psychosis. This is thera- peutically critical since the line of treatment may be different between the two types of psychoses. Keywords: Amphetamine, First Episode Psychosis 1. Introduction In patients with psychosis like schizophrenia and/or bi- polar disorder, substance abuse has been reported [1-4]. Previous studies have found high prevalence of schizo- phrenia and other psychotic disorders among users of illicit substances like cannabis [5] and amphetamines [6, 7]. Recently, a common co-occurrence of first episode psychosis and substance use disorders like cannabis, al- cohol and amphetamines has been reported [8-10]. In Saudi Arabia, the rapid development of socioecono- mic status and the “oil boom” have led to the adoption of novel recreational attitudes including drug abuse [11]. The annual incidence number of Saudi patients newly admitted to the hospitals with abused drugs is increasing especially for amphetamine at the expense of other sub- stances like heroin, alcohol, and sedatives. The fre- quency of amphetamine use among Saudi people of 40 years old or less increased markedly in the period 2000-2006 in comparison with the period 1986-1999 [12]. Different sources are available for abused am- phetamine preparations by youth in Saudi Arabia like clandestine laboratories and near by countries like Yemen. The high incidence of amphetamine use in Saudi population of young age in addition to the unavailability of any previous studies regarding amphetamine use Saudi psychotic patients have led to designing of this study. The primary aim was to describe the current am- phetamine use in a sample of Saudi patients experiencing first episode of acute psychosis through urine screening for the drug. Secondary aims were to find out any points of difference in demographics and clinical picture that  102 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients can help differentiation between first episode psychotic patients who were amphetamine positive and those who were negative for amphetamine. 2. Patients and Methods One hundred six adult Saudi patients attended the Psy- chiatric Emergency Service of Buraidah Mental Health Hospital in Al-Qassim Governorate, Kingdom of Saudi Arabia in the period from January to July; 2008 and di- agnosed as first episode of acute psychosis. Following admission of each patient, one urine sample was col- lected for amphetamine screening. It was sent immedi- ately to the Toxicology Center of the Ministry of Health. The Axsym analyzer of Abbott using the fluorescence immunoassay technique was used in the screening and a cutoff value ≥1000 ng/ml was considered positive for amphetamine screening. Positive samples then were con- firmed by Gas Chromatography Mass Spectrometry (GC- MS) technique with cutoff values of ≥300 ng/ml for posi- tive amphetamine samples [13]. 2.1. Clinical Assessment Each patient was interviewed (at admission, and then daily) by an expert psychiatrist for clinical and psychiat- ric assessment. The interview included questionnaire about the socio-demographic data including educational history, employment, socio-economic status, substance use history and family history. Missing data was ob- tained from patient’s relatives to complete the patient profile. Questionnaire about family history included in- quiry about family support (e.g. provision of housing, food, clothing and money), parental substance abuse and parental mental illness. All data were analyzed according to the criteria of psychotic illness for diagnosis of acute psychosis, and possible psychoactive substance use as defined by the International Classification of Diseases (ICD-10) [14]. The severity of psychotic symptoms in each patient was evaluated by applying the positive and negative syndrome scale (PANSS). The PANSS scale is a 30-item standardized instrument that measures positive symptoms such as hallucination and delusions, negative symptoms such as affective blunting, emotional with- drawal, and general symptoms such as motor retardation, anxiety, disorientation) using a semi-structured interview and chart review [15,16]. 2.2. Personality Assessment During admission period, and once the patient became stable as regards psychotic symptoms, he was assessed by the same expert psychiatrist for any personality disor- der and its cluster according to a semi structured inter- view for personality disorder evaluation [17,18]. The clusters examined for personality disorders included: Cluster A (e.g. schizoid, schizotypal or paranoid), Clus- ter B (e.g. antisocial, borderline, histrionic or narcissis- tic) and Cluster C (e.g. avoidant, dependent or obses- sive). The study was carried out after approval from the ethical committee, General Directorate of Health Affairs, Al-Qassim Province, Ministry of Health, Kingdom of Saudi Arabia and getting the acceptance of the responsi- ble relatives concerning each patient. 2.3. Statistical Analysis Data analysis was performed with a personal computer using the SPSS statistical software program, version 13 (SPSS, 2002). The comparison of data between the psy- chotic patients who were amphetamine positive and or negative was based on whether the measurement of the variable was categorical or scaled. Chi-square ( 2) test or Fisher’s exact test (whenever appropriate) and un- paired t-tests were used to determine the statistical sig- nificance of the difference between the variables. Statis- tical significance was considered at p < 0.05. 3. Results Screening of urine samples for amphetamine in all pa- tients (n = 106) revealed positive results in 34 subjects (32%). The average concentration of amphetamine in positive urine samples was 6189.8 ± 634.7 ng/ml. Table 1 showed the demographic features of the psychotic pa- tients whether they were amphetamine positive or nega- tive. Male gender was the most common sex in all pa- tients (79/106; 74.5%) and all amphetamine positive cas- es were males. The poor family support and history of parental substance abuse were significantly recorded (p < 0.05) in amphetamine positive group while the parental mental illness was significantly evident (p < 0.01) in amphetamine negative psychotic group. However, low education, unemployment, unmarried status and socio- economic standard were not different between the two groups. Analysis of psychotic symptoms showed qualitative similarity in many of the psychiatric symptoms tested (though some incidence differences) between the two psychotic groups. The observation indicates the difficulty of symptoms-based discrimination between ampheta- mine positive and amphetamine negative acute psychosis (Table 2). Hallucinations including visual, auditory and paranoid were evident in both although the incidence of paranoid type of hallucination was significantly higher in amphetamine positive group in comparison with the oth- er group (19 % vs. 10 %; p < 0.05 respectively). As re- gards other psychotic symptoms, significant incidence (p < 0.001) of depression (44% vs. 13%), ideas of reference (50% vs. 14%), and suspiciousness (44% vs. 11%) was also observed in amphetamine positive psychosis in C opyright © 2011 SciRes. PP 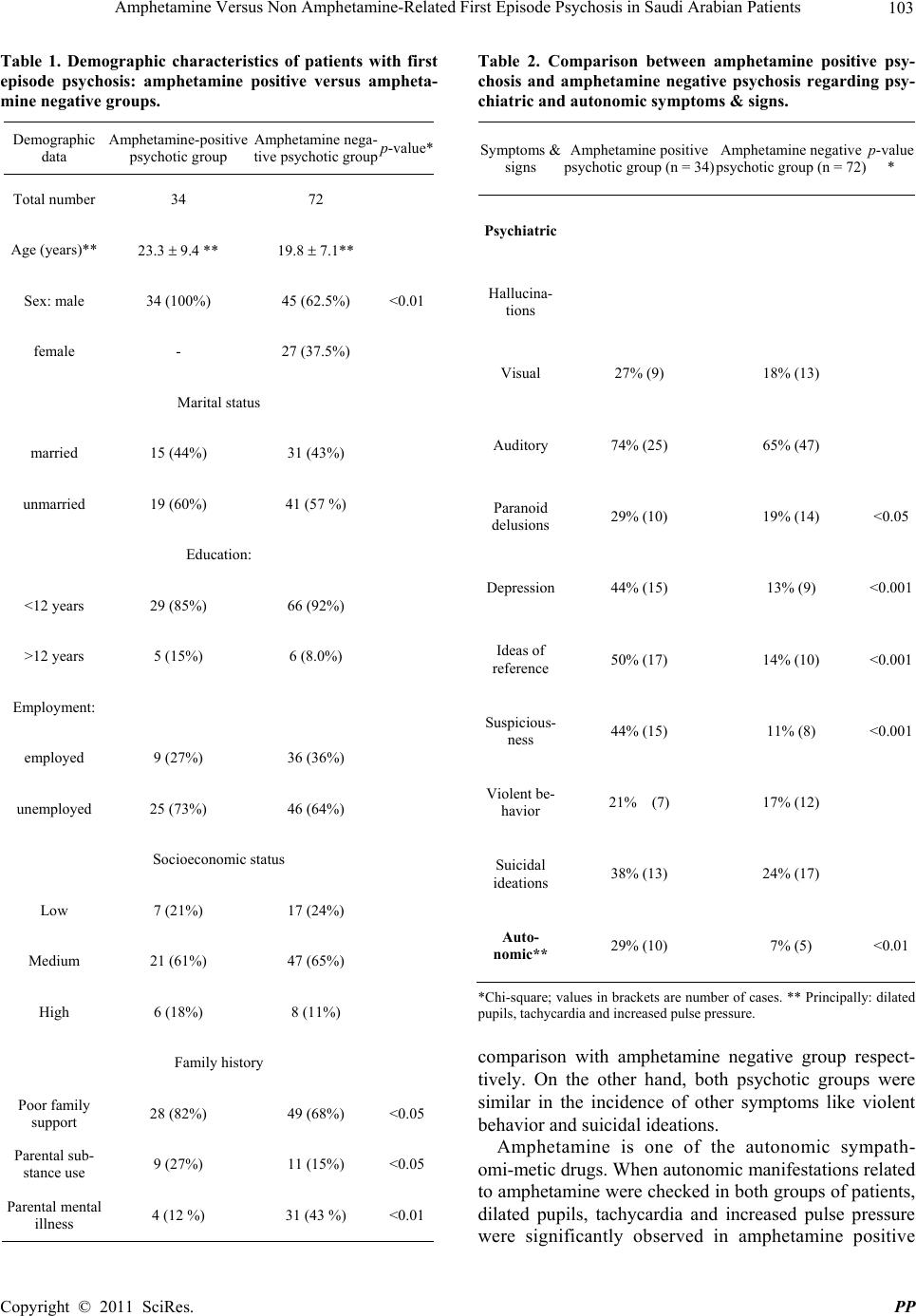 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients 103 Table 1. Demographic characteristics of patients with first episode psychosis: amphetamine positive versus ampheta- mine negative groups. Table 2. Comparison between amphetamine positive psy- chosis and amphetamine negative psychosis regarding psy- chiatric and autonomic symptoms & signs. Demographic data Amphetamine-positive psychotic group Amphetamine nega- tive psychotic groupp-value* Total number 34 72 Age (years)** 23.3 9.4 ** 19.8 7.1** Sex: male 34 (100%) 45 (62.5%) <0.01 female - 27 (37.5%) Marital status married 15 (44%) 31 (43%) unmarried 19 (60%) 41 (57 %) Education: <12 years 29 (85%) 66 (92%) >12 years 5 (15%) 6 (8.0%) Employment: employed 9 (27%) 36 (36%) unemployed 25 (73%) 46 (64%) Socioeconomic status Low 7 (21%) 17 (24%) Medium 21 (61%) 47 (65%) High 6 (18%) 8 (11%) Family history Poor family support 28 (82%) 49 (68%) <0.05 Parental sub- stance use 9 (27%) 11 (15%) <0.05 Parental mental illness 4 (12 %) 31 (43 %) <0.01 Symptoms & signs Amphetamine positive psychotic group (n = 34) Amphetamine negative psychotic group (n = 72) p-value * Psychiatric Hallucina- tions Visual 27% (9) 18% (13) Auditory 74% (25) 65% (47) Paranoid delusions 29% (10) 19% (14) <0.05 Depression44% (15) 13% (9) <0.001 Ideas of reference 50% (17) 14% (10) <0.001 Suspicious- ness 44% (15) 11% (8) <0.001 Violent be- havior 21% (7) 17% (12) Suicidal ideations 38% (13) 24% (17) Auto- nomic** 29% (10) 7% (5) <0.01 *Chi-square; values in brackets are number of cases. ** Principally: dilated pupils, tachycardia and increased pulse pressure. comparison with amphetamine negative group respect- tively. On the other hand, both psychotic groups were similar in the incidence of other symptoms like violent behavior and suicidal ideations. Amphetamine is one of the autonomic sympath- omi-metic drugs. When autonomic manifestations related to amphetamine were checked in both groups of patients, dilated pupils, tachycardia and increased pulse pressure were significantly observed in amphetamine positive Copyright © 2011 SciRes. PP 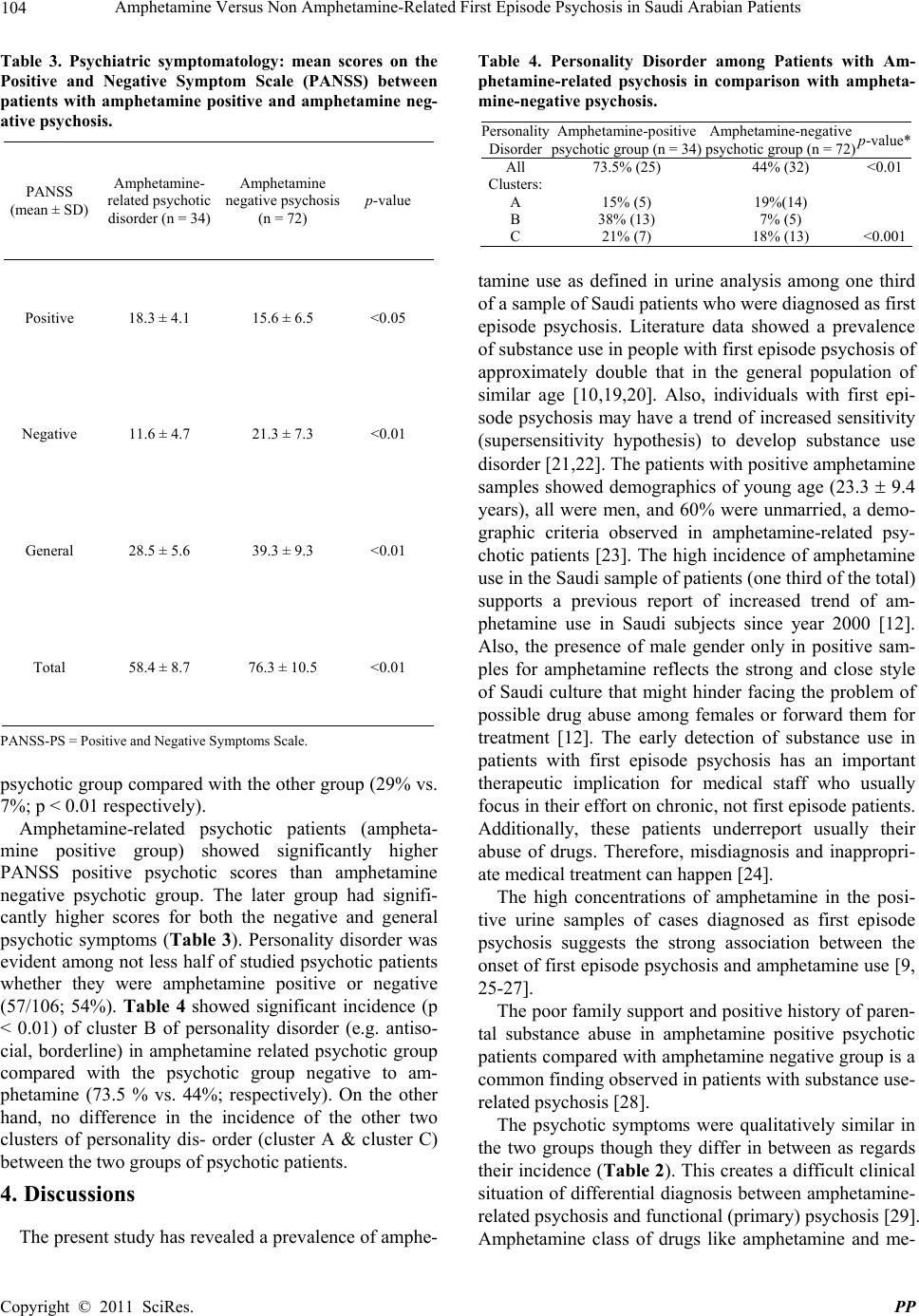 104 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients Table 3. Psychiatric symptomatology: mean scores on the Positive and Negative Symptom Scale (PANSS) between patients with amphetamine positive and amphetamine neg- ative psychosis. Table 4. Personality Disorder among Patients with Am- phetamine-related psychosis in comparison with ampheta- mine-negative psychosis. PANSS (mean ± SD) Amphetamine- related psychotic disorder (n = 34) Amphetamine negative psychosis (n = 72) p-value Positive 18.3 ± 4.1 15.6 ± 6.5 <0.05 Negative 11.6 ± 4.7 21.3 ± 7.3 <0.01 General 28.5 ± 5.6 39.3 ± 9.3 <0.01 Total 58.4 ± 8.7 76.3 ± 10.5 <0.01 PANSS-PS = Positive and Negative Symptoms Scale. psychotic group compared with the other group (29% vs. 7%; p < 0.01 respectively). Amphetamine-related psychotic patients (ampheta- mine positive group) showed significantly higher PANSS positive psychotic scores than amphetamine negative psychotic group. The later group had signifi- cantly higher scores for both the negative and general psychotic symptoms (Table 3). Personality disorder was evident among not less half of studied psychotic patients whether they were amphetamine positive or negative (57/106; 54%). Table 4 showed significant incidence (p < 0.01) of cluster B of personality disorder (e.g. antiso- cial, borderline) in amphetamine related psychotic group compared with the psychotic group negative to am- phetamine (73.5 % vs. 44%; respectively). On the other hand, no difference in the incidence of the other two clusters of personality dis- order (cluster A & cluster C) between the two groups of psychotic patients. 4. Discussions The present study has revealed a prevalence of amphe- Personality Disorder Amphetamine-positive psychotic group (n = 34) Amphetamine-negative psychotic group (n = 72)p-value* All 73.5% (25) 44% (32) <0.01 Clusters: A 15% (5) 19%(14) B 38% (13) 7% (5) C 21% (7) 18% (13) <0.001 tamine use as defined in urine analysis among one third of a sample of Saudi patients who were diagnosed as first episode psychosis. Literature data showed a prevalence of substance use in people with first episode psychosis of approximately double that in the general population of similar age [10,19,20]. Also, individuals with first epi- sode psychosis may have a trend of increased sensitivity (supersensitivity hypothesis) to develop substance use disorder [21,22]. The patients with positive amphetamine samples showed demographics of young age (23.3 9.4 years), all were men, and 60% were unmarried, a demo- graphic criteria observed in amphetamine-related psy- chotic patients [23]. The high incidence of amphetamine use in the Saudi sample of patients (one third of the total) supports a previous report of increased trend of am- phetamine use in Saudi subjects since year 2000 [12]. Also, the presence of male gender only in positive sam- ples for amphetamine reflects the strong and close style of Saudi culture that might hinder facing the problem of possible drug abuse among females or forward them for treatment [12]. The early detection of substance use in patients with first episode psychosis has an important therapeutic implication for medical staff who usually focus in their effort on chronic, not first episode patients. Additionally, these patients underreport usually their abuse of drugs. Therefore, misdiagnosis and inappropri- ate medical treatment can happen [24]. The high concentrations of amphetamine in the posi- tive urine samples of cases diagnosed as first episode psychosis suggests the strong association between the onset of first episode psychosis and amphetamine use [9, 25-27]. The poor family support and positive history of paren- tal substance abuse in amphetamine positive psychotic patients compared with amphetamine negative group is a common finding observed in patients with substance use- related psychosis [28]. The psychotic symptoms were qualitatively similar in the two groups though they differ in between as regards their incidence (Ta ble 2). This creates a difficult clinical situation of differential diagnosis between amphetamine- related psychosis and functional (primary) psychosis [29]. Amphetamine class of drugs like amphetamine and me- C opyright © 2011 SciRes. PP 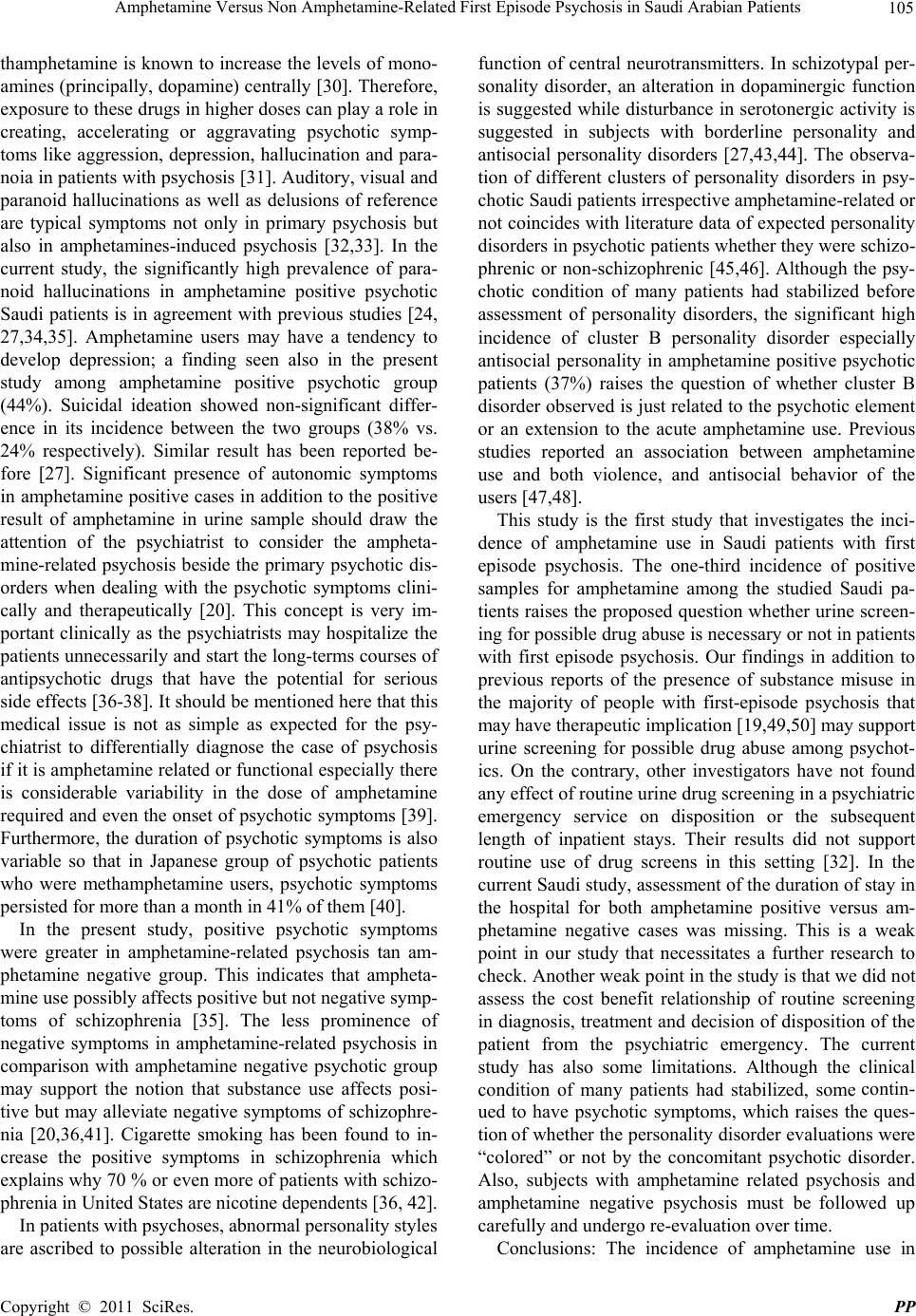 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients 105 thamphetamine is known to increase the levels of mono- amines (principally, dopamine) centrally [30]. Therefore, exposure to these drugs in higher doses can play a role in creating, accelerating or aggravating psychotic symp- toms like aggression, depression, hallucination and para- noia in patients with psychosis [31]. Auditory, visual and paranoid hallucinations as well as delusions of reference are typical symptoms not only in primary psychosis but also in amphetamines-induced psychosis [32,33]. In the current study, the significantly high prevalence of para- noid hallucinations in amphetamine positive psychotic Saudi patients is in agreement with previous studies [24, 27,34,35]. Amphetamine users may have a tendency to develop depression; a finding seen also in the present study among amphetamine positive psychotic group (44%). Suicidal ideation showed non-significant differ- ence in its incidence between the two groups (38% vs. 24% respectively). Similar result has been reported be- fore [27]. Significant presence of autonomic symptoms in amphetamine positive cases in addition to the positive result of amphetamine in urine sample should draw the attention of the psychiatrist to consider the ampheta- mine-related psychosis beside the primary psychotic dis- orders when dealing with the psychotic symptoms clini- cally and therapeutically [20]. This concept is very im- portant clinically as the psychiatrists may hospitalize the patients unnecessarily and start the long-terms courses of antipsychotic drugs that have the potential for serious side effects [36-38]. It should be mentioned here that this medical issue is not as simple as expected for the psy- chiatrist to differentially diagnose the case of psychosis if it is amphetamine related or functional especially there is considerable variability in the dose of amphetamine required and even the onset of psychotic symptoms [39]. Furthermore, the duration of psychotic symptoms is also variable so that in Japanese group of psychotic patients who were methamphetamine users, psychotic symptoms persisted for more than a month in 41% of them [40]. In the present study, positive psychotic symptoms were greater in amphetamine-related psychosis tan am- phetamine negative group. This indicates that ampheta- mine use possibly affects positive but not negative symp- toms of schizophrenia [35]. The less prominence of negative symptoms in amphetamine-related psychosis in comparison with amphetamine negative psychotic group may support the notion that substance use affects posi- tive but may alleviate negative symptoms of schizophre- nia [20,36,41]. Cigarette smoking has been found to in- crease the positive symptoms in schizophrenia which explains why 70 % or even more of patients with schizo- phrenia in United States are nicotine dependents [36, 42]. In patients with psychoses, abnormal personality styles are ascribed to possible alteration in the neurobiological function of central neurotransmitters. In schizotypal per- sonality disorder, an alteration in dopaminergic function is suggested while disturbance in serotonergic activity is suggested in subjects with borderline personality and antisocial personality disorders [27,43,44]. The observa- tion of different clusters of personality disorders in psy- chotic Saudi patients irrespective amphetamine-related or not coincides with literature data of expected personality disorders in psychotic patients whether they were schizo- phrenic or non-schizophrenic [45,46]. Although the psy- chotic condition of many patients had stabilized before assessment of personality disorders, the significant high incidence of cluster B personality disorder especially antisocial personality in amphetamine positive psychotic patients (37%) raises the question of whether cluster B disorder observed is just related to the psychotic element or an extension to the acute amphetamine use. Previous studies reported an association between amphetamine use and both violence, and antisocial behavior of the users [47,48]. This study is the first study that investigates the inci- dence of amphetamine use in Saudi patients with first episode psychosis. The one-third incidence of positive samples for amphetamine among the studied Saudi pa- tients raises the proposed question whether urine screen- ing for possible drug abuse is necessary or not in patients with first episode psychosis. Our findings in addition to previous reports of the presence of substance misuse in the majority of people with first-episode psychosis that may have therapeutic implication [19,49,50] may support urine screening for possible drug abuse among psychot- ics. On the contrary, other investigators have not found any effect of routine urine drug screening in a psychiatric emergency service on disposition or the subsequent length of inpatient stays. Their results did not support routine use of drug screens in this setting [32]. In the current Saudi study, assessment of the duration of stay in the hospital for both amphetamine positive versus am- phetamine negative cases was missing. This is a weak point in our study that necessitates a further research to check. Another weak point in the study is that we did not assess the cost benefit relationship of routine screening in diagnosis, treatment and decision of disposition of the patient from the psychiatric emergency. The current study has also some limitations. Although the clinical condition of many patients had stabilized, some contin- ued to have psychotic symptoms, which raises the ques- tion of whether the personality disorder evaluations were “colored” or not by the concomitant psychotic disorder. Also, subjects with amphetamine related psychosis and amphetamine negative psychosis must be followed up carefully and undergo re-evaluation over time. Conclusions: The incidence of amphetamine use in Copyright © 2011 SciRes. PP 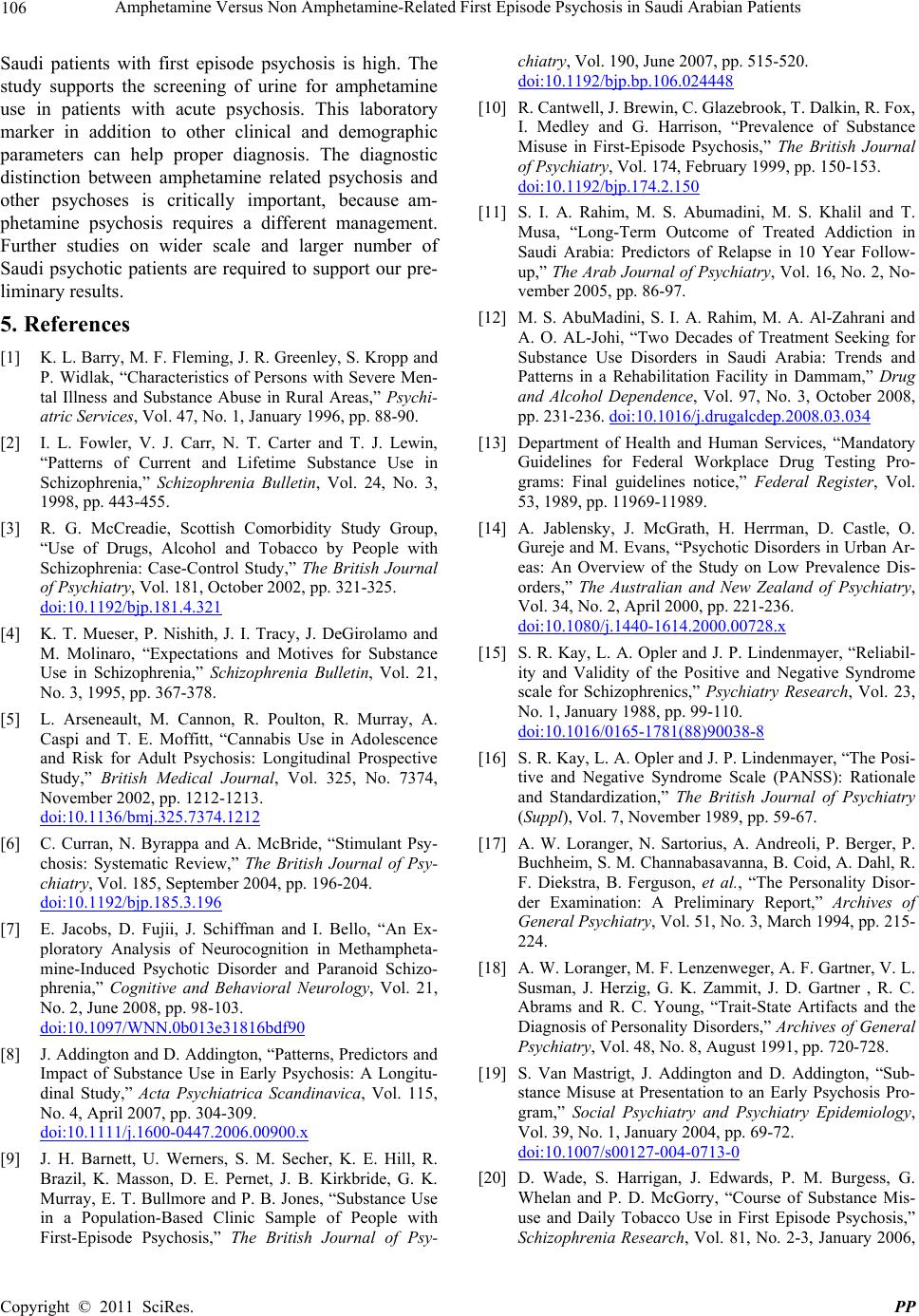 106 Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients Saudi patients with first episode psychosis is high. The study supports the screening of urine for amphetamine use in patients with acute psychosis. This laboratory marker in addition to other clinical and demographic parameters can help proper diagnosis. The diagnostic distinction between amphetamine related psychosis and other psychoses is critically important, because am- phetamine psychosis requires a different management. Further studies on wider scale and larger number of Saudi psychotic patients are required to support our pre- liminary results. 5. References [1] K. L. Barry, M. F. Fleming, J. R. Greenley, S. Kropp and P. Widlak, “Characteristics of Persons with Severe Men- tal Illness and Substance Abuse in Rural Areas,” Psychi- atric Services, Vol. 47, No. 1, January 1996, pp. 88-90. [2] I. L. Fowler, V. J. Carr, N. T. Carter and T. J. Lewin, “Patterns of Current and Lifetime Substance Use in Schizophrenia,” Schizophrenia Bulletin, Vol. 24, No. 3, 1998, pp. 443-455. [3] R. G. McCreadie, Scottish Comorbidity Study Group, “Use of Drugs, Alcohol and Tobacco by People with Schizophrenia: Case-Control Study,” The British Journal of Psychiatry, Vol. 181, October 2002, pp. 321-325. doi:10.1192/bjp.181.4.321 [4] K. T. Mueser, P. Nishith, J. I. Tracy, J. DeGirolamo and M. Molinaro, “Expectations and Motives for Substance Use in Schizophrenia,” Schizophrenia Bulletin, Vol. 21, No. 3, 1995, pp. 367-378. [5] L. Arseneault, M. Cannon, R. Poulton, R. Murray, A. Caspi and T. E. Moffitt, “Cannabis Use in Adolescence and Risk for Adult Psychosis: Longitudinal Prospective Study,” British Medical Journal, Vol. 325, No. 7374, November 2002, pp. 1212-1213. doi:10.1136/bmj.325.7374.1212 [6] C. Curran, N. Byrappa and A. McBride, “Stimulant Psy- chosis: Systematic Review,” The British Journal of Psy- chiatry, Vol. 185, September 2004, pp. 196-204. doi:10.1192/bjp.185.3.196 [7] E. Jacobs, D. Fujii, J. Schiffman and I. Bello, “An Ex- ploratory Analysis of Neurocognition in Methampheta- mine-Induced Psychotic Disorder and Paranoid Schizo- phrenia,” Cognitive and Behavioral Neurology, Vol. 21, No. 2, June 2008, pp. 98-103. doi:10.1097/WNN.0b013e31816bdf90 [8] J. Addington and D. Addington, “Patterns, Predictors and Impact of Substance Use in Early Psychosis: A Longitu- dinal Study,” Acta Psychiatrica Scandinavica, Vol. 115, No. 4, April 2007, pp. 304-309. doi:10.1111/j.1600-0447.2006.00900.x [9] J. H. Barnett, U. Werners, S. M. Secher, K. E. Hill, R. Brazil, K. Masson, D. E. Pernet, J. B. Kirkbride, G. K. Murray, E. T. Bullmore and P. B. Jones, “Substance Use in a Population-Based Clinic Sample of People with First-Episode Psychosis,” The British Journal of Psy- chiatry, Vol. 190, June 2007, pp. 515-520. doi:10.1192/bjp.bp.106.024448 [10] R. Cantwell, J. Brewin, C. Glazebrook, T. Dalkin, R. Fox, I. Medley and G. Harrison, “Prevalence of Substance Misuse in First-Episode Psychosis,” The British Journal of Psychiatry, Vol. 174, February 1999, pp. 150-153. doi:10.1192/bjp.174.2.150 [11] S. I. A. Rahim, M. S. Abumadini, M. S. Khalil and T. Musa, “Long-Term Outcome of Treated Addiction in Saudi Arabia: Predictors of Relapse in 10 Year Follow- up,” The Arab Journal of Psychiatry, Vol. 16, No. 2, No- vember 2005, pp. 86-97. [12] M. S. AbuMadini, S. I. A. Rahim, M. A. Al-Zahrani and A. O. AL-Johi, “Two Decades of Treatment Seeking for Substance Use Disorders in Saudi Arabia: Trends and Patterns in a Rehabilitation Facility in Dammam,” Drug and Alcohol Dependence, Vol. 97, No. 3, October 2008, pp. 231-236. doi:10.1016/j.drugalcdep.2008.03.034 [13] Department of Health and Human Services, “Mandatory Guidelines for Federal Workplace Drug Testing Pro- grams: Final guidelines notice,” Federal Register, Vol. 53, 1989, pp. 11969-11989. [14] A. Jablensky, J. McGrath, H. Herrman, D. Castle, O. Gureje and M. Evans, “Psychotic Disorders in Urban Ar- eas: An Overview of the Study on Low Prevalence Dis- orders,” The Australian and New Zealand of Psychiatry, Vol. 34, No. 2, April 2000, pp. 221-236. doi:10.1080/j.1440-1614.2000.00728.x [15] S. R. Kay, L. A. Opler and J. P. Lindenmayer, “Reliabil- ity and Validity of the Positive and Negative Syndrome scale for Schizophrenics,” Psychiatry Research, Vol. 23, No. 1, January 1988, pp. 99-110. doi:10.1016/0165-1781(88)90038-8 [16] S. R. Kay, L. A. Opler and J. P. Lindenmayer, “The Posi- tive and Negative Syndrome Scale (PANSS): Rationale and Standardization,” The British Journal of Psychiatry (Suppl), Vol. 7, November 1989, pp. 59-67. [17] A. W. Loranger, N. Sartorius, A. Andreoli, P. Berger, P. Buchheim, S. M. Channabasavanna, B. Coid, A. Dahl, R. F. Diekstra, B. Ferguson, et al., “The Personality Disor- der Examination: A Preliminary Report,” Archives of General Psychiatry, Vol. 51, No. 3, March 1994, pp. 215- 224. [18] A. W. Loranger, M. F. Lenzenweger, A. F. Gartner, V. L. Susman, J. Herzig, G. K. Zammit, J. D. Gartner , R. C. Abrams and R. C. Young, “Trait-State Artifacts and the Diagnosis of Personality Disorders,” Archives of General Psychiatry, Vol. 48, No. 8, August 1991, pp. 720-728. [19] S. Van Mastrigt, J. Addington and D. Addington, “Sub- stance Misuse at Presentation to an Early Psychosis Pro- gram,” Social Psychiatry and Psychiatry Epidemiology, Vol. 39, No. 1, January 2004, pp. 69-72. doi:10.1007/s00127-004-0713-0 [20] D. Wade, S. Harrigan, J. Edwards, P. M. Burgess, G. Whelan and P. D. McGorry, “Course of Substance Mis- use and Daily Tobacco Use in First Episode Psychosis,” Schizophrenia Research, Vol. 81, No. 2-3, January 2006, C opyright © 2011 SciRes. PP  Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients 107 pp. 145-150. doi:10.1016/j.schres.2005.09.010 [21] V. M. Gonzalez, C. M. Bradizza, P. C. Vincent, P. R. Stasiewicz and N. D. Paas, “Do Individuals with a Severe Mental Illness Experience Alcohol and Drug-Related Problems? A Test of the Supersensitivity Hypothesis,” Addictive Behaviors, Vol. 32, No. 3, March 2007, pp. 477-490. doi:10.1016/j.addbeh.2006.05.012 [22] D. Harris and S. L. Batki, “Stimulant Psychosis: Symp- tom Profile and Acute Clinical Course,” The American Journal on Addiction, Vol. 9, No. 3, Winter 2000, pp. 28-37. [23] N. Chivite-Matthews, A. Richardson, J. O’Shea, J. Bec- ker, N. Owen, S. Roe, et al., “Drug Misuse Declared: Findings from 2003/2004 British Crime Survey,” Home Office Statistical Survey, 2005. [24] C. L. Caton, R. E. Drake, D. S. Hasin, B. Dominguez, P. E. Shrout, S. Samet and B. Schanzer, “Differences be- tween Early Phase Primary Psychotic Disorders with Concurrent Substance Use and Substance-Induced Psy- choses,” Archives of General Psychiatry, Vol. 62, No. 2, February 2005, pp. 137-145. doi:10.1001/archpsyc.62.2.137 [25] M. J. Schiller, M. Shumway and S. L. Batki, “Patterns of Substance Use among Patients in an Urban Psychiatric Emergency Service,” Psychiatric Services, Vol. 51, No. 1, January 2000, pp. 113-115. [26] M. Lambe rt, P. Conus, D. I. Lubman, D. Wade, H. Yuen, S. Moritz, D. Naber and B. G. Schimmelmann, “The Im- pact of Substance Use Disorders on Clinical Outcome in 643 Patients with First Episode Psychosis,” Acta Psy- chiatrica Scandinavics, Vol. 112, No. 2, August 2005, pp. 141-148. doi:10.1111/j.1600-0447.2005.00554.x [27] L. Hides, S. M. Cotton, G. Berger, J. Gleeson, C. O’Donnell, T. Proffitt, P. D. McGorry and D. I. Lubman, “The Reliability and Validity of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in First Episode Psychosis,” Addictive Behaviors, Vol. 34, No. 10, October 2009, pp. 821-25. doi:10.1016/j.addbeh.2009.03.001 [28] C. L. Caton, R. E. Drake, D. S. Hasin, B. Dominguez, P. E. Shrout, S. Samet and B. Schanzer, “Differences be- tween Early Phase Primary Psychotic Disorders with Concurrent Substance Use and Substance-Induced Psy- choses,” Archives of General Psychiatry, Vol. 62, No. 2, February 2005, pp. 137-145. doi:10.1001/archpsyc.62.2.137 [29] J. M. Brown, G. R. Hanson and A. E. Fleckenstein, “Regulation of the Vesicular Monoamine Transporter-2: A Novel Mechanism for Cocaine and Other Psycho- stimulants,” Journal of Pharmacology and Experimental Therapeutics, Vol. 286, No. 3, March 2001, pp. 762-767. [30] A. M. Barr, W. J. Panenka, G. W. MacEwan, A. E. Thornton, D. J. Lang, W. G. Honer and T. Lecomte, “The Need for Speed: An Update on Methamphetamine Addic- tion,” Journal of Psychiatry & Neuroscience, Vol. 31, No. 5, September 2006, pp. 301-313. [31] C. K. Chen, S. K. Lin, P. C. Sham, D. Ball, E. W. Loh, C. C. Hsiao, Y. L. Chiang, S. C. Ree, C. H. Lee and R. M. Murray, “Premorbid Characteristics and Co-Morbidity of Methamphetamine Users with and without Psychosis,” Psychological Medicine, Vol. 33, No. 8, November 2003, pp. 1407-1414. doi:10.1017/S0033291703008353 [32] C. C. Cruickshank and K. R. Dyer, (2009). “A Review of the Clinical Pharmacology of Methamphetamine,” Addic- tion, Vol. 104, No. 7, July 2009, pp. 1085-1099. doi:10.1111/j.1360-0443.2009.02564.x [33] M. J. Schiller, M. Shumway and S. L. Batki, “Utility of Routine Drug Screening in a Psychiatric Emergency Set- ting,” Psychiatric Servoces, Vol. 51, No. 4, April 2000, pp. 474- 478. doi:10.1176/appi.ps.51.4.474 [34] R. McKetin, J. McLaren, D. Lubman and L. Hides, “The Prevalence of Psychotic Symptoms among Metham- phetamine Users,” Addiction, Vol. 101, No. 4, April 2000, pp. 1473-1478. [35] A. Baker, S. Bucci, T. J. Lewin, R. Richmond and V. J. Carr, “Comparisons between Psychosis Samples with Different Patterns of Substance Use Recruited for Clini- cal and Epidemiological Studies,” Psychiatry Research, Vol. 134, No. 3, April 2005, pp. 241-250. doi:10.1016/j.psychres.2005.02.006 [36] H. C. Margolese, L. Malchy, J. C. Negrete, R. Tempier and K. H. Gill, “Drug and Alcohol Use among Patients with Schizophrenia and Related Psychoses: Levels and Consequences,” Schizophrenia Research, Vol. 67, No. 2-3, April 2004, pp. 157-66. [37] A. Davies, M. A. Adena, N. A. Keks, S. V. Catts, T. Lambert and I. Schweitzer, “Risperidone Versus Halop- eridol: Meta-Analysis of Efficacy and Safety,” Clinical Therapeutics, Vol. 20, No. 1, January-February 1998, pp. 58- 71. doi:10.1016/S0149-2918(98)80034-9 [38] C. D. Carlson, P. A. Cavazzoni, P. H. Berg, H. Wei, C. M. Beasley and J. M. Kane, “An Integrated Analysis of Acute Treatment-Emergent Extrapyramidal Syndrome in Patients with Schizophrenia during Olanzapine Clinical Trials: Comparisons with Placebo, Haloperidol, Risperi- done, or Clozapine,” Journal of Clinical Psychiatry, Vol. 64, 2003, pp. 898-906. doi:10.4088/JCP.v64n0807 [39] B. M. Schanzer, M. B. First, B. Dominguez, D. S. Hasin and C. L. Caton, “Diagnosing Psychotic Disorders in the Emergency Department in the Context of Substance Use,” Psychiatric Services, Vol. 57, No. 10, October 2006, pp. 1468-1473. doi:10.1176/appi.ps.57.10.1468 [40] D. S. Bell, “The Experimental Reproduction of Am- phetamine Psychosis,” Archives of General Psychiatry, Vol. 29, No. 1, July 1973, pp. 35-40. [41] H. Ujiki and M. Sato, “Clinical Features of Sensitization to Methamphetamine Observed in Patients with Me- thamphetamine Dependence and Psychosis,” Annals of the New York Academy of Sciences, Vol. 1025, October 2004, pp. 279-87. doi:10.1196/annals.1316.035 [42] M. A. Test, L. S. Wallisch, D. J. Allness and K. Ripp, “Substance Use in Young Adults with Schizophrenic Disorders,” Schizophrenia Bulletin, Vol. 15, No. 3, 1989, pp. 465-4765. Copyright © 2011 SciRes. PP  Amphetamine Versus Non Amphetamine-Related First Episode Psychosis in Saudi Arabian Patients Copyright © 2011 SciRes. PP 108 [43] C. J. Van Dongen, “Smoking and Persistent Mental Ill- ness: An Exploratory Study,” Journal of Psychosocial. Nursing and Mental Health Services, Vol. 37, No. 11, November 1999, pp. 26-34. [44] M. Srisurapanont, R. Ali, J. Marsden, A. Sunga, K. Wada and M. Monteiro, “Psychotic Symptoms in Methamphe- tamine Psychotic in-Patients,” The International Journal of Neuropsychopharmacology, Vol. 6, No. 4, December 2003, pp. 347-352. doi:10.1017/S1461145703003675 [45] D. Harris and S. L. Batki, “Stimulant Psychosis: Symp- tom Profile and Acute Clinical Course,” The American Journal on Addiction, Vol. 9, No. 1, Winter 2000, pp. 28-37. doi:10.1080/10550490050172209 [46] I. I. Solano and M. G. DeChavez, “Premorbid Personality Disorders in Schizophrenia,” Schizophrenia Research, Vol. 44, No. 2, August 2000, pp.137-144. doi:10.1016/S0920-9964(99)00203-0 [47] D. Lichtermann, E. Karbe and W. Maier, “The Genetic Epidemiology of Schizophrenia and of Schizophrenia Spectrum Disorders,” European Archives of Psychiatry and Neuroscience, Vol. 250, No.6, 2000, pp. 304-310. doi:10.1007/s004060070005 [48] M. S. Keshavan, H. S. Duggal, G. Veeragandham, N. M. McLaughlin, D. M. Montrose, G. L. Haas and N. R. Schooler, “Personality Dimensions in First-Episode Psy- choses,” The American Journal of Psychiatry, Vol. 162, No. 1, January 2005, pp. 102-109. doi:10.1176/appi.ajp.162.1.102 [49] J. C. Maxwell, “Emerging Research on Methampheta- mine,” Current Opinion in Psychiatry, Vol. 18, No. 3, May 2005, pp. 235-242. doi:10.1097/01.yco.0000165592.52811.84 [50] S. D. Gray, D. M. Fatovich, D. L. McCoubrie and F. F. Daly, “Amphetamine-Related Presentations to an Inner- City Tertiary Emergency Department: A Prospective Evaluation,” The Medical Journal of Australia, Vol. 186, No. 7, April 2007, pp. 336-339.
|