J. CHAPIN
358
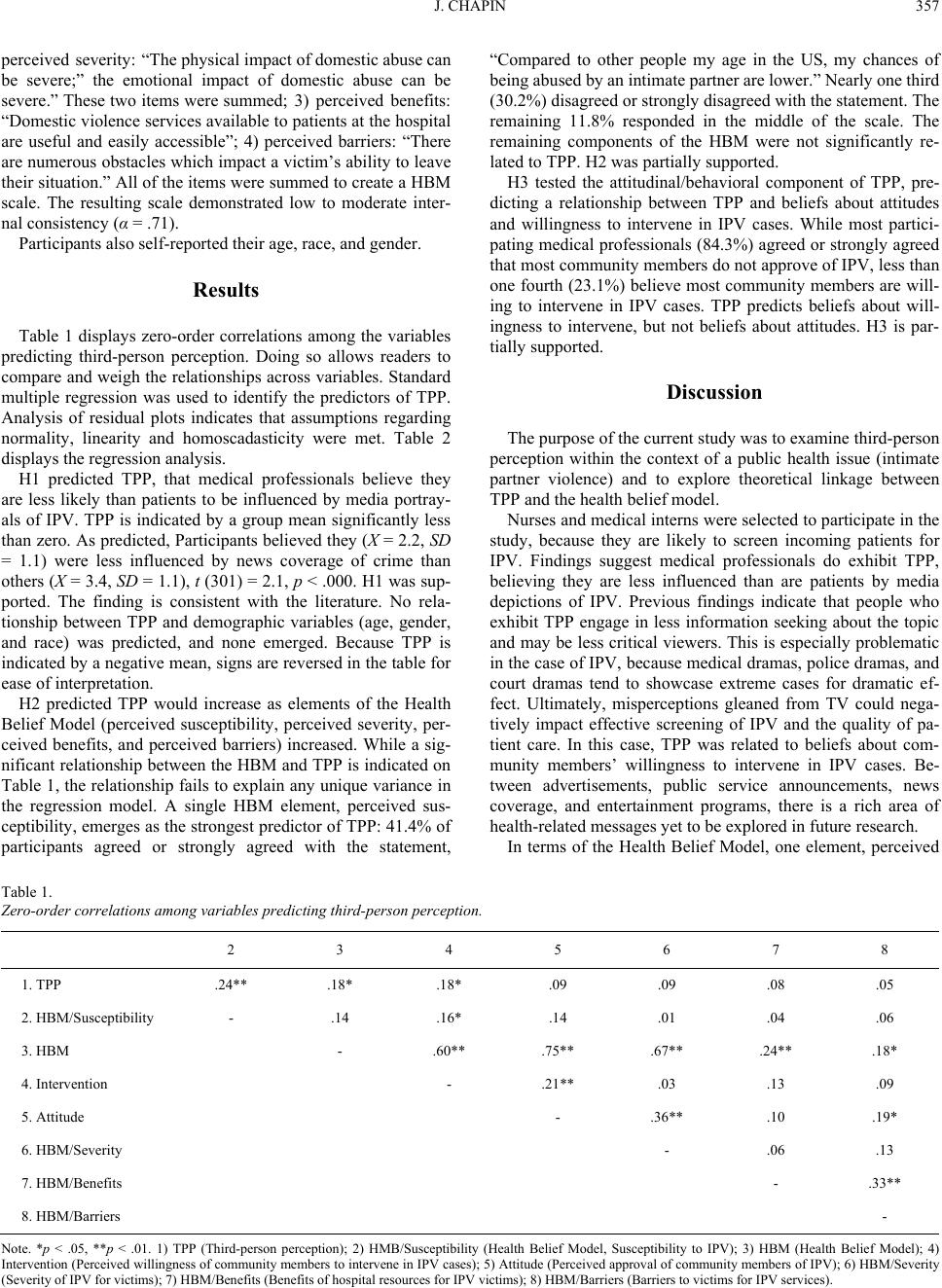
Table 2.
Summary of linear regression analysis for variables predicting third-
person perception.
Adj. r2 = .10
N = 306
Predictor B SE B β
HBM/Susceptibility .11 .06 .16*
HMB .04 .10 .08
*p < .05
susceptibility, emerged as a predictor of TPP. A similar con-
struct, optimistic bias, has been linked with TPP in the past
(Chapin, 2000; Salwen & Dupagne, 2003). Perceived suscepti-
bility and perceived severity tend to be the strongest predictors
of attitudes and behaviors in the HBM literature. In this case,
98.7% agreed or strongly agreed that the emotional impact of
IPV is severe and 98.1 agreed or strongly agreed that the physi-
cal impact of IPV is severe. The lack of variance may explain
the insignificant finding. While it was not the focus of this paper,
it’s interesting to note that both community attitudes about IPV
and willingness to intervene were more strongly related to the
HBM than to TPP. The finding solidifies the value of the model
for IPV scholars and advocates. It also provides the groundwork
for future linkages between the HBM and TPP literatures.
A number of limitations should be considered before inter-
preting the results of this study. The study is based on a con-
venience sample of medical personnel gathered for training on
intimate partner violence. Test measures were collected prior to
the training to limit skewed responses, but participants were
aware of the topic and some priming may have occurred.
Conflict of Interest Statement
None to report.
References
Boyle, M., McLeod, D., & Rojas, H. (2008). The role of ego enhance-
ment and perceived message exposure in third-person perception
judgments concerning violent video games. American Behavioral
Scientist, 52, 165-185. doi:10.1177/0002764208321349
Campo, S., Poulos, G. & Sipple, J. (2005). Prevalence and profiling:
Hazing among college students and points of intervention. American
Journal of Health Behavior, 29, 137-149.
Carlson, A., Campbell, J., Garza, M., Campo, P., Dienemann, J., Kub,
J., Jones, A., & Lloyd, D. (2006). Domestic violence in the military:
Women’s policy preferences and beliefs concerning routine screen-
ing and mandatory repor ting. Military Medicine, 171, 729-735.
Chapin, J. (2000). Third-person perception and optimistic bias among
urban minority at-risk youth. Communication Research, 27, 51-81.
doi:10.1177/009365000027001003
Chia, S. (2009). When the east meets the west: An examination of
third-person perceptions about idealized body image in Singapore.
Mass Communication and Society, 12, 423-445.
doi:10.1080/15205430802567123
Chia, S., & Wen, N. (2009). College men’s third-person perceptions
about idealized body image and consequent behavior. Paper pre-
sented at the annual meeting of the International Communication
Association.
Cho, H., & Boster, F. (2008). First and third person perceptions on
anti-drug ads among adolescents. Communication Research, 35,
169-189. doi:10.1177/0093650207313158
Chock, T., Fox, J., Angelini, J., Lee, S., & Lang, A. (2007). Telling me
quickly: How arousing fast-paced PSAs decrease self-other distinc-
tions. Communication Research, 34, 618-63 6.
doi:10.1177/0093650207307900
Coe, K. Tewksbury, D., Bond, B., Drogos, K., Porter, R., Yahn, A., &
Zhang, Y. (2008). Hostile news: Partisan use and perceptions of ca-
ble news programming. Journal of Communication, 58, 201-219.
doi:10.1111/j.1460-2466.2008.00381.x
Cohen, J., & Weimann, G. (2008). Who’s afraid of reality shows? Ex-
ploring the effects of reality shows and the concern over their social
effects on willingness to censor. Communication Research, 35,
382-397. doi:10.1177/0093650208315964
Conners, J. (2005). Understanding third-person effect. Communication
Research Trends, 24, 3- 22.
Davison, W. (1983). The third-person effect in communication. Public
Opinion Quarterly, 47, 1-15. doi:10.1086/268763
Day, A. (2008). Out of the living room and into the voting booth: An
analysis of corporate public affairs advertising under the third-person
effect. American Behavioral Scientist, 52, 243-260.
doi:10.1177/0002764208321354
Frederick, E., & Neuwirth, K. (2008). The second-person effect and its
role in formation of active issues publics. Mass Communication and
Society, 11, 514-538. doi:10.1080/15205430802368613
Golan, G., Banning, S., & Lundy, L. (2008). Likelihood to vote, candi-
date choice, and the third-person effect. American Behavioral Scien-
tist, 52, 278-290. doi:10.1177/0002764208321356
Golan, G., & Day, A. (2008). The first-person effect and its behavioral
consequences: A new trend in the twenty-five year history of
third-person effect research. Mass Communication and Society, 11,
539-556. doi:10.1080/15205430802368621
Jeffres, L., Neundorf, K., Bracken, C., & Atkin, D. (2008). Integrating
theoretical traditions in media effects: Using third-person effects to
link agenda-setting and cultivation. Mass Communication and Soci-
ety, 11, 470-491. doi:10.1080/15205430802375303
Lewis, I., Watson, B., & Tay, R. (2007). Examining the effectiveness of
physical threats in road safet y advertising: The role of the third-person
effect, gender and age. Transportation Research, 10, 48-60.
Lin, P., Simoni, J. & Zemon, V. (2005). The health belief model, sexual
behaviors, and HIV risk among Taiwanese immigrants. AIDS Educa-
tion and prevention, 17, 469- 483. doi:10.1521/aeap.2005.17.5.469
Rubin, B., Rubin, A., Graham, E., Perse, E., & Seibold, D. (2009).
Communication research measures II: A sourcebook. New York:
Routledge.
Salwen, M., & Dupagne, M. (2003). News of Y2K and experiencing
Y2K: Exploring the relationship between the third-person effect and
optimistic bias. Media Psychology, 5, 57-82.
doi:10.1207/S1532785XMEP0501_3
Sigal, B. (2009). The third-person effect in Israeli women’s attitude to
TV commercials and their images. Paper presented at the annual
meeting of the International Communication Association.
Wei, R., Lo, V., & Lu, H. (2008). Third-person effects of health news:
Exploring the relationships among media exposure, presumed media
influence, and behavioral intentions. American Behavioral Scientist,
52, 261-277.
Zhao, X., & Cai, X. (2008). From self-enhancement to supporting cen-
sorship: The third-person effect process in the case of Internet por-
nography, Mass Communication and Society, 11, 437-462.
doi:10.1080/15205430802071258
Zhong, Z. (2009). Third-person perceptions and online games: A com-
parison of perceived antisocial and prosocial game effects. Journal of
Computer-Mediated Communication, 14, 286-306.
doi:10.1111/j.1083-6101.2009.01441.x