S. N. Nallapati et al.
Although the E/e’ ratio is a robust marker in the predictio n of left ventricular filling pressure, it is imperfect
and sho uld be interpr eted wit h conside ration o f many si tuatio ns such a s severe mitral annular calcification, sig-
nificant mitral stenosis, moderate-to-severe mitral regurgitation, severe left ventricular dysfunction, and hyper-
trophic cardiomyopathy. These conditions can be a source of misleading information in the setting of acute
myocardial infarction [3].
Study Limitations
Our study has certain limitations: 1) the sample size is inadequate to draw conclusions in whole population; 2)
echocardiographer was not blinded in this study, which might impact selection bias; 3) certain compounding
factors like PCI/CABG and compliance of drug intake were not considered in the analysis, which might influ-
ence t he study fi ndings; 4) Since E/e’ ratio reflects an instantaneous measure of left ventricular filling p ressure,
a single measurement may not convey maximal prognostic information as the left ventricular filling pressure
may change over the course of the peri-infarct period; and 5) the follow-up period was only 6 months, which is
not enough to draw significant co ncl us io ns of sur v iva l. We s ug ges t tha t st ud ie s i nvo l vi ng l ar ge r sample -size and
long-term follow-up would offer necessary insights regarding the prognostic value of E/e’ ratio. We are of opi-
nion that echocardiographic estimation of E/e’ can be used as a valuable bed-size tool in the risk-strati ficatio n of
the patients with acute myocardial infarction.
5. Conclusion
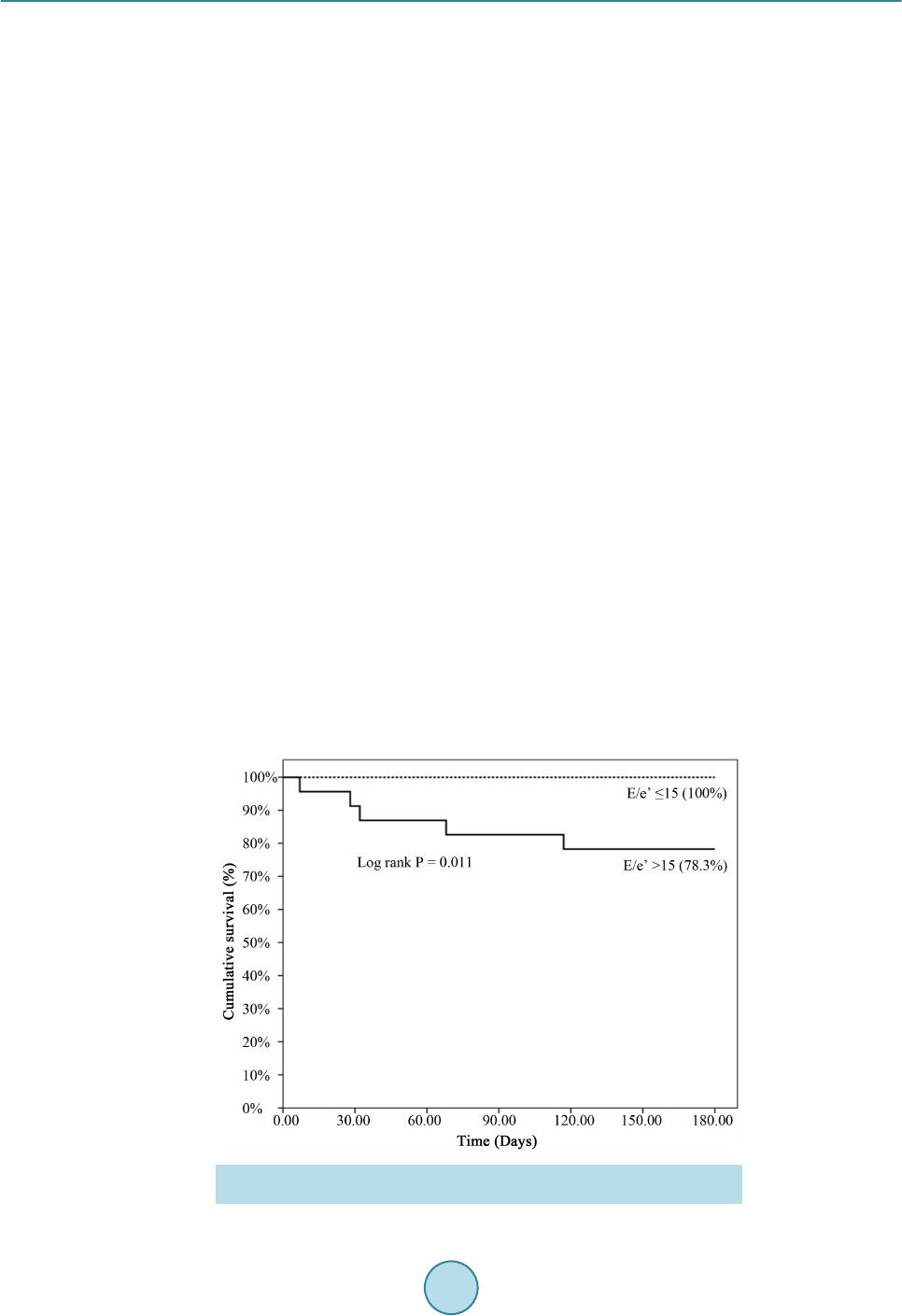
Findings of the present study suggest that an E/e’ ratio >15 is a powerful predictor of decreased survival after
acute STEMI. Further studies are warranted to substantiate the findings. However, we opine that measurement
of E/e’ may assist ris k-stratification of patie nts in this settin g.
References
[1] Gaziano, T.A., Bitton, A., Anand, S., Abrahams-Gessel, S. and Murphy, A. (2010) Growing Epidemic of Coronary
Heart Disease in Low- and Midd le-Income Countries. Current Problems in Cardiology, 35, 72-115.
http://dx.doi.org/10.1016/j.cpcardiol.2009.10.002
[2] Hillis, G.S., Moller, J.E., Pellikka, P.A., Gersh, B.J., Wright, R.S., Ommen, S.R., Reeder, G.S. and Oh, J.K. (2004)
Noninvasive Estimation of Left Ventricular Filling Pressure by E/e' Is a Powerful Predictor of Survival after Acute
Myocardial Infarction. Journal of the American College of Cardiology, 43, 360-367.
http://dx.doi.org/10.1016/j.jacc.2003.07.044
[3] Park, J.H. and Marwick, T.H. (2011) Use and Limitations of E/e' to Assess Left Ventri cular Fillin g Pressure b y Echo-
cardiography. Journal of Cardiovascular Ultrasound, 19, 169-173. http://dx.doi.org/10.4250/jcu.2011.19.4.169
[4] Liang, H.Y., Cauduro, S.A., Pellikka, P.A., Bailey, K.R., Grossardt, B.R., Yang, E.H., Rihal, C., Seward, J.B., Miller,
F.A. and Abraham, T.P. (2006) Comparison of Usefulness of Echocardiographic Doppler Variables to Left Ventricular
End-Diastolic Pressure in Predicting Futu r e H eart Failure Events. American Journal of Cardiology, 97, 866-871.
http://dx.doi.org/10.1016/j.amjcard.2005.09.136
[5] Ommen, S.R., Nishimura, R.A., Appleton, C.P., Miller, F.A., Oh, J.K., Redfield, M.M. and Tajik, A.J. (2000) Clinical
Utility of Doppler Echocardiography and Tissue Doppler Imaging in the Estimation of Left Ventricular Filling Pres-
sures: A Comparative Simul taneous Doppler-Catheterization Study. Circulation, 102, 1788-1794.
http://dx.doi.org/10.1161/01.CIR.102.15.1788
[6] Poulsen, S.H. (2001) Clinical Aspects of Left Ventricular Diastolic Function Assessed by Doppler Echocardiography
Following Acute Myocardial Infarction. Danish Medical Bulletin, 48, 199-210.
[7] Nagueh, S.F., Appleton, C.P., Gillebert, T.C., Marino, P.N., Oh, J.K., Smiseth, O.A., Waggoner, A.D., Flachskampf,
F.A., Pellikka, P.A. and Evangelisa, A. (2009) Recommendations for the Evaluation of Left Ventricular Diastolic
Function by Echocardiography. European Journal of Echocardiography, 10, 165-193.
http://dx.doi.org/10.1093/ejechocard/jep007
[8] Cerisano, G. and Bolognese, L. (2001) Echo-Doppler Evaluation of Left Ventricular Diastolic Dysfunction during
Acute Myocardial Infarct ion: Methodological, Clinical and Prognostic Implications. Italian Heart Journal, 2, 13-20.
[9] Shanks, M., Ng, A.C., van de Veire, N.R., Antoni, M.L., Bertini, M., Delgado, V., Nucifora, G., Holman, E.R., Choy,
J.B., Leung, D.Y., Schalij, M.J. and Bax, J.J. (2010) Incremental Prognostic Value of Novel Left Ventricular Diastolic
Indexes for P rediction of Clinical Outco me in Patients with ST-Elevation M yocardial Infarction . American Journal of