Psychology
Vol.07 No.14(2016), Article ID:72508,15 pages
10.4236/psych.2016.714169
Identification of Students at Risk for Attention Deficit Disorder with Hyperactivity Using the Response to Intervention Model (RTI)
Giseli Donadon Germano, Simone Aparecida Capellini
Investigation Learning Disabilities Laboratory (LIDA), Speech and Hearing Sciences Department, São Paulo State University “Júlio de Mesquita Filho” UNESP, Marília, Brazil

Copyright © 2016 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: October 28, 2016; Accepted: December 2, 2016; Published: December 5, 2016
ABSTRACT
The use of Response to Intervention Model (RTI) has been described in the literature as an important tool for early identification of students at risk of learning problems. However, such studies are rare in the Brazilian population. This study aimed to use the response to intervention model (RTI) as an early identification procedure for Attention Deficit Disorder (ADD) students from 1st grade level of elementary school in Brazilian population. A total of 118 students participated of this study, aged between 6:0 and 6:11 (years:months), from 1st grade level, of both genders. The study was divided into three phases. In the first phase, all students were tested individually with Visual Attention Test software (TAVIS) composed of three tasks: selective attention, alternating attention and sustained attention. Because it was an initial study, all students were submitted to the Remediation Program with Attention and Working Memory (RAWM) in phase 2. The program consists of attention skills and phonological working memory skills (7 individual sessions, 40 minutes each). In phase 3, the students were submitted to the TAVIS. As results, from 118 students, 106 students concluded all 3 phases, which 34 students (32%) met the risk criteria for ADD after being submitted to the program. Of these, 34 students, 15 students (46.7%) responded to the intervention, while 19 students (59.3%) not responded. These students who not responded to the intervention program were sent to multidisciplinary care for monitoring and subsequent confirmation of the diagnosis of ADD. The findings of this study able us to conclude that RTI model can be used as an early identification tool for student at risk of attention in the early years literacy deficit.
Keywords:
Attention Deficit Disorder/Hyperactivity, Response to Intervention Model (RTI), Early Identification, Assessment, Education

1. Introduction
Response to Intervention model (RTI) is defined by the National Research Center on Learning Disabilities (NRCLD) as an assessment and intervention process for systematic monitoring student progress and making decisions about the need for education changes or increasing intensification services using progress monitoring information ( Johnson, Mellard, Fuchs, & McKnight, 2006 ).
The main purpose of RTI is to prevent academic and behavioral problems and help identifying students with specific learning difficulties ( Reutebuch, 2008 ). Roth, Dougherty, Paul and Adamczyk (2010) described RTI as a model of intervention that is possible the early identification of students with language disorders, learning and reading problems and thus, a model that provides a cognitive-linguistic instruction that supports these students to overcome their difficulties during the literacy period. RTI has been described in the literature with the following levels: 1) multiple levels, 2) evaluation system, 3) protocol and 4) educational interventions based on evidence. There is not necessarily an even relationship between one level and another; also, the levels may overlap depending on the need for intervention ( Barnes & Harlacher, 2008 ).
The principle of multiple levels is one of the most described in the international literature (Hale, 2008; Johnson et al., 2006 ) and is often developed on three levels. According with the authors, level 1 has the aim to identify risk for behavioral and learning problems using procedures based on the academic curriculum of these students, so it would be able to verify if these students reached the expected results for its own group-class. At level 2, the aim is to determine the type of intervention that will be used to assist the student to overcome their difficulties (specific intervention). In addition, in this level, the student must receive a specific intervention, where the teacher in the classroom can count on with help of speech therapists, psychologists, occupational therapists or specialized teachers to determine the best intervention model addressed to the teacher or directed to student individually or in-group. At this level 2, it’s important to verify if the student presented or not presented response to intervention. If is the case that the student did not responded, this will imply that he hasn’t overcome his learning or behavioral difficulties, so he must be send to an interdisciplinary assessment, which will occur at level 3. In the latter level, the aim will be to perform an interdisciplinary diagnosis and to check for indication for a specialized service or for special education.
Thus, the use of the RTI model allows classifying the student at his appropriate levels, but also monitoring his progress in relation to the teaching-learning process ( Coyne & Harn, 2006 ; National Association of State Directors of Special Education, NASDSE, 2006 ). This means that the data collected in the evaluation should facilitate and direct the development of intervention procedures to ensure the effectiveness of its application. Because it is an evidence-based intervention procedure, the RTI has been used by educators, practitioners and researchers as an alternative that can provide data for early identification in a fast and effective way, as well as ensuring a support directed through the intervention in the educational context ( Gresham, 2002 ; Learning Disabilities Roundtable, 2005 ).
However, despite international developments with the use of RTI in school population has been occurred in the last decades ( Gresham, 2002 ; Coyne & Harn, 2006 ; Johnson et al., 2006 ; NASDSE, 2006 ; Barnes & Harlacher, 2008 ; Roth et al., 2010 ; Hale, 2012 ). However, in Brazil there are few researches using the response to intervention model, that has been published, such as the use of RTI model for early identification of student at risk of dyslexia ( Refundini, Martins, & Capellini, 2010 ; Fadini & Capellini, 2011 ; Fukuda & Capellini, 2011 ; Martins & Capellini, 2011 ; Andrade, Andrade, & Capellini, 2014 ; Capellini, Cesar, & Germano, 2015 ) and only recently for ADHD ( Capellini, Silva, & Germano, 2015 ; Germano & Okuda, 2015 ; Germano, Silva, & Capellini, 2015 ).
The Diagnostic and Statistical Manual of Mental Disorders ( American Psychiatric Association, APA, 2013 ) Attention Deficit Hyperactivity Disorder (ADHD) by the persistent presence of inattention signs and/or hyperactivity-impulsivity that end up interfering with the language development, motor, social and academics impairments.
Among the damages described in the literature, students with ADHD have academic difficulties, such as poor performance in reading and writing activities, logical-mathe- matical reasoning, reading comprehension, motor skills resulting from neuropsychological changes ( DuPaul, Weyandt, & Janusis 2011 ; Dyck & Piek, 2014 ). Although there is a vast literature about low academic performance and how this affects the student progress throughout academic life, there is only a few studies about the early identification and intervention with students at risk for ADHD. This reinforces the idea that it is imperative and necessary the improvements of studies about early identification and interventions in school context, particularly during the early years of literacy.
Among the options of intervention in the classroom, Sayal, Hornsey, Warren, MacDiarmid and Taylor (2006) described a training program with teachers, which the aim was to teach them to identify students at risk for ADHD by themselves, in order to facilitate recommendations to specialized services for further diagnoses. This study involved only teachers and was divided into four phases. Phase 1 consisted of a training of recognition, which teachers should indicate which student would fill signs of inattention and/or hyperactivity, using the criteria described in the Diagnostic and statistical manual of mental disorders―DSM-IV ( APA, 1994 ).
In the 2nd phase, teachers should fill out a questionnaire about student’s difficulties (Strengths and Difficulties Questionnaire―SDQ, Goodman, 1997 ). In the 3rd phase, the researchers made an intervention with teachers, with a duration of 45-minute, providing information about the symptoms, diagnosis criteria, and possible diagnostic co-occurrences. In the last phase, phase 4, the teachers repeat the proceeds of phase 1. In this phase, it was verified that after the intervention there was an increase of the proportion of students considered at risk for ADHD by teachers. Therefore, it was possible to verify that teachers began to better identify students at risk for ADHD, as well as they learnt to recognize some of the predictors signs. In conclusion, this study indicated that a brief educational intervention with teachers could help identify students at risk for ADHD.
The survey was repeated after six years. Sayal, Merrell, Tymms and Kasim (2015) conducted a follow-up survey to investigate the impact of the interventions described above, with the application of tests to re-evaluate the performance of students who were identified as risk for ADHD. According to the results, the authors reported that there was a relationship between the symptoms of inattention and poor academic performance. The same relationship was not observed when compared to impulsivity symptoms. The authors concluded that behavioral and educational interventions could maximize the potential of interventions.
Haraway (2012) conducted a survey in order to provide an overview of possible evaluation methods, taking in account the needs of students with ADHD, using the model of RTI (combination of layers) and also using an intervention models for positive behavior. The author described that normally, RTI model includes three layers. In the first layer, all the students were submitted to assessments and interventions with academic and behavioral strategies. In the behavioral field, such strategies include training students for appropriate behaviors (i.e. knowledge of classroom routines), and supported by a system of recognition/reinforcing positive behavior. The results of the evaluations were analyzed, providing the basis for the preparation of layer 2, which was designed to complement layer 1, but including intervention in small groups and monitoring of students’ progress. Layer 3 was designed for a direct intervention with small number of students who have not made progress. The author referred that it was possible to use RTI model (layers 1 and 2), but also, this study showed the possibility of carrying out assessments or surveys based on curriculum content, involving math skills, reading and spelling skills, and then use this content to select or program the assessments subtests. After this selection, the author indicated that the academic process could be graphically represented, favoring communication with parents and other professionals in the teaching-learning process.
Also, in the same study, another example given by the author was regarding the combination of layers 2 and 3 of RTI model. It was possible monitoring students’ pro- gress, referring to a direct observation of behavior that was carried out in the classroom, that is, to compute and to record the occurrence of a behavior (i.e. the number of times the student talked without permission or the number of minutes the student kept sit). Initially, one researcher or teacher should select a target behavior and then perform the collection within a specified period. For convenience, the viewer can convert behaviors to percentage to allow quick comparison. This information will help educators and consultants to determine if the target behavior is specific to the student or indicates that the problem may be due the classroom management.
Andrade, Andrade and Capellini (2014) reported that the most common model and most accepted is the three-tier model. The layer 1 is characterized by universal screening of students at risk for learning disabilities and/or attentional deficits, but also by an universal or primary preventive intervention, in which all students receive regular instruction of excellence (in classroom). Both effective instruction and universal screening for students at risk in Tier 1 are processes that require well-trained professionals. At layer 2, the students identified as “at risk” (i.e. those who do not responded adequately to the intervention of layer 1 or universal screening) receive a secondary intervention (also called intervention Layer 2), characterized by instruction directed at small groups of 3 to 4 students with weekly or fortnightly monitoring of their progress. At layer 3, those who still didn’t responded to an intervention are redirected to a diagnosis pro- cesses.
Fuchs and Fuchs (2006) highlighted three aspects considered as essential to the implementation of these models: 1) systematization of identification processes, intervention and evaluation of responsiveness, 2) involvement of highly trained professionals through continuous training, and 3) reasoning on scientific evidence regarding both monitoring, content strategies and interventions, as well as the monitoring of student progress.
Thus, according to described above, the hypothesis of this study is that students at risk for Attention Deficit Disorder (ADD) could be identified by using layer 1 of the RTI model, i.e. assessment and intervention using visual attention skills and phonological working memory skills.
Thus, this study aimed to use the first layer of Response to Intervention model (RTI) as an early identification and intervention procedure for identification of students at risk for Disorder Attention Deficit Disorder (ADD) of 1st grade level of elementary school.
2. Method
This study was approved by the Ethics under the Protocol 0663/2013 the Faculty of Philosophy and Sciences, São Paulo State University Committee “Júlio de Mesquita Filho” (FFC/UNESP).
Participated of this study 118 students aged from 6:0 years-old to 6:11 years-old, of both sex, from 1st grade level of elementary school. As exclusion criteria for this research, it was considered: students with sensory, motor or cognitive impairment and students who did not present signature of the Consent and Informed Term. Inclusion criteria: students who present signature of the Consent and Informed Term, students without presence of sensory, motor or cognitive impairment constant in school records. This study was focused the first layer of the RTI model, and was composed of three phases, being performed in a period of 6 months.
As procedure, this study was divided into three phases, such as pre-testing, intervention and post-testing procedures. In the first phase, all students were tested individually using Visual Attention Test Software (TAVIS-4, Duchesne & Mattos, 1997 ). This test was applied in a single session (duration of 20 to 30 minutes). The student was assessed in a separate and silent room of the school. The student was placed in front of a computer, and received a joystick. The instruction consisted that the student must press the button of the joystick after Examiner orientation regarding the task. Visual Attention Test Software (TAVIS-4, Duchesne & Mattos, 1997 ; Coutinho, Mattos, Araújo, & Duchesne, 2007 ) consists of three tasks: Visual Selection Attention, Visual Alternate Attention and Visual Sustained Attention as described below:
- Task 1: Visual Selection Attention Task. It consists in making the student to respond selectively to a target stimulus, ignoring the presence of other stimuli (distractors). This task is the presentation of sequential stimuli (colored animals, i.e. yellow and green hippopotamus, blue and red squirrel, green lion) and it was required that the student to identify a target (specific colored animal, i.e. yellow hippopotamus with black spot on body) among several other distractors stimuli, responding exclusively to it. The stimulus was presented one by one at computer screen. Thus, Coutinho et al. (2007) reported that in addition to the attention capacity, the task requires visual scanning (ability to follow with their eyes a set of information in line) and it’s an important ability to visual selectivity. The result of this task may be indicative of problems with attention or selectivity skills.
- Task 2: Visual Alternate Attention Task. In this task, the student should pay attention and respond alternately to two different parameters equal/different. At the computer screen, geometric shapes were presented. When the forms were shown in green, the student should press the button if the forms were identical (e.g. Circle with circle). When the forms were presented in red, the student should press the button if the forms were different (e.g. Circle with square). This alternation task requires the ability to change the focus of attention among different parameters of the same concept ( Coutinho et al., 2007 ).
- Task 3: Visual Sustained Attention Task. This task requires the student to sustain attention to the computer screen for a long period, in order to respond quickly to the emergence of a stimulus. On the computer screen, the stimulus presented was a clock that appeared in different positions on the screen. The stimulus appeared and then disappeared. The student should pay attention to the screen because the stimulus appeared again after a randomized time interval in another position on the screen. This task primarily demand sustained attention, being a long-term task (lasts six minutes for students with 7 minutes).
The software itself performs the score. There are three types of punctuation. First punctuation is obtained by the number of correct answers (NCA). Second punctuation is the number of errors per omission (NEO), which consists of not detecting the occurrence of a target stimulus, failing to respond to this or responding very slowly (not pressing the button of joystick). The third punctuation is the number of errors per action (NEA), which consists of responding in the absence of the stimulus target, or pressing the joystick button when there is no stimulus on the screen (task 3) or against the appearance of a non-target stimulus (tasks 1 and 2). The report errors per action can help us to assess the tendency to impulsiveness of the student. This parameter is particularly important in the diagnosis of Attention Deficit Disorder (ADD) in each of the three tasks ( Duchesne & Mattos, 1997 ).
For the realization of the sample cohort peak it was used, as a criterion, the descriptive statistical analysis of the population of this study. Therefore, it was used as cutoff point percentile 25 (mean values below percentile 25 for number of correct answers; mean values above percentile 25 for number of errors per omission and for number of errors per action). This percentile was chosen in an attentive to select a great number of student at risk, considering a preventive aspect. If a student met this criteria, he or she was considerate as “at risk” for ADD and was addressed to phase 2.
In phase 2, the students “at risk” were submitted to the Remediation Program with Attention and Working Memory (RAWM; Capellini, Silva, & Germano, 2015 ; Germano, Silva, & Capellini, 2015 ) in phase 2 of this study. The program consisted of 8 sessions, applied individually, twice a week, with sessions lasting 30 to 40 minutes in the school class period in a separate room. The program was composed by figures of substantives, previously selected by linguistic criterions ( Germano & Capellini, 2015 ).
In this program, activities were designed to work the working memory skills and attention, based in Baddeley (1986) Model. For working memory skills were developed activities such as grouping of figures by semantic category (animals and fruits); Figures grouping (animals and fruits) according with the initial letter (alphabet target); organization of stories in sequence with figures; sequential memory with figures and letters; create mental images (relate sentence with figures; relate numbers with geometric shapes and form sequences of numbers). For attention skills, it was prepared activities such as finding differences between the two pictures; figures finding and words findings; visuospatial relationship with figures, geometric shapes and letters; memory game with figures and letters; creating mental images (create phrases and numbers using figures and geometric shapes).
In the third phase, all students were re-tested individually using Visual Attention Test Software (TAVIS-4, Duchesne & Mattos, 1997 ).
3. Results
Initially, 118 students were selected from the first grade level of elementary school. However, 12 students were excluded for not performing all intervention sessions provided in this study due to excessive absences. Thus, 106 students participated in all phases. The classification of the socioeconomic level was performed based on the statistical study of the Socioeconomic Development Index ( Foundation of Economy and Statistics, 2003 ), thus guaranteeing the homogeneity of the sample from an average socioeconomic point of view.
Table 1 shows the distribution of mean, standard deviation, minimum and maximum values, values of percentiles 25 and 75. Therefore, it was used as cutoff point percentile 25, such as mean values below percentile 25 for number of correct answers (NCA) and mean values above percentile 25 for number of errors per omission (NEO) and for number of errors per action (NEA). This criterion was used both in the pre-testing analysis as in post-testing. In addition, the students selected to be submitted to the remediation program should fulfil those criterion in at least five of the nine variables that composed the elaborate remediation procedure.
From the 106 students, 34 students (32%) met the criteria “at risk” for ADHD after being submitted to the program. Because it was an initial study, all students were submitted to Remediation Program with Attention and Working Memory (RAWM; Capellini, Silva, & Germano, 2015 ; Germano, Silva, & Capellini, 2015 ) in phase 2. Table 2 shows the distribution the results of the comparison of pre and post-testing of Visual Attention Test Software (TAVIS-4, Duchesne & Mattos, 1997 ), using Wilcoxon Signed Ranks Test.
In Table 2, there was a statistical difference in task 1 (selectivity) for number of errors per action (NEA). There was diminish of mean when comparing pre and post- testing. This finding suggest that students improved their attention in selecting a stimuli target and a reducing in impulsivity behavior. There was a statistical difference in task 2 (alternation attention) for all variables number of correct answers (NCA), number of errors by omission (NEO) and number of errors per action (NEA), showing a reducing of numbers of errors in post-testing and an increasing in the number of correct answers, suggesting a positive interference of the remediation program.
In addition, there was a statistical difference in task 3 (task of sustained attention) of number of errors by omission (NEO) and number of errors per action (NEA). However, there was an increase of the number of errors by omission and errors by action. This

Table 1. Distribution of mean (M), standard deviation (SD), minimum (min) and maximum values (max), percentiles values 25 (25%) and 75 (75%) of the students in TAVIS-4 tasks.
Legend: NCA: number of correct answers; NEO: number of errors by omission; NEA: number of errors per action.
Table 2. Distribution of mean, standard deviation (SD) and p value between pre and post-testing TAVIS-4.
Legend: NCA: number of correct answers; NEO: number of errors by omission; NEA: number of errors per action. Wilcoxon Signed Ranks Test (*p < 0.05).
result suggest that there was a maintenance of an attention deficit or an impulsivity by the students for task 3 (Sustained attention Task), which indicates a possible maintenance of sustained attention deficit for a greater time interval, demonstrating a lack of response of students and so, confirming the presence of students “at risk” for ADHD.
As results, from 118 students, 106 students concluded all 3 phases, which 34 students (32.07%) met the risk criteria for ADHD after being submitted to the program. Of these 34 students, we found that 15 students (44.12%) responded to the intervention, while 19 students (55.88%) not responded.
Of the total of 106 school participants, 34 students (32.07%) met the criteria described above. After being subjected to elaborate remediation program (RAMT), the students were again submitted to TAVIS and was reapplied the same cutoff criteria in order to see which school not respond to the intervention, that is, who did not have performance improvement post-testing situation. From these 34 students (Figure 1). These students who not responded to remediation program developed in this study were referred to specialized care for monitoring and subsequent confirmation of the diagnosis of ADHD. Figure 1 resume the findings of this study.
4. Discussion
One of the most important findings of this study is the occurrence of lack of response
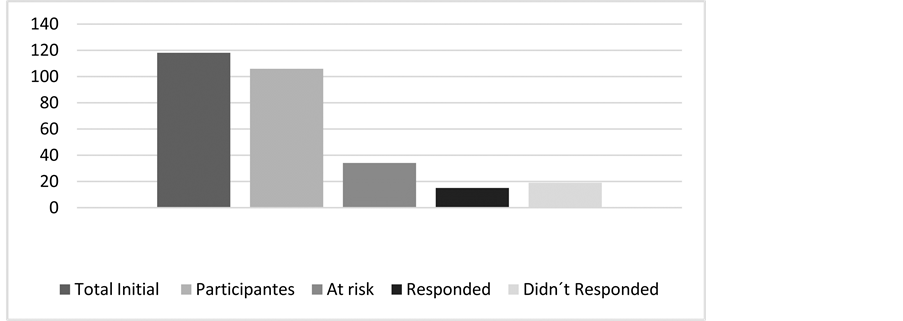
Figure 1. Distribution of students according to the Model Response to Intervention (RTI).
to intervention that occurred in 55.88% (19 students) of the sample. This represents a great advance in terms of diagnostic and innovation in educational policy in Brazil, since as a common procedure is to direct students to a health care center in later ages.
The purpose of early identification is to determine which children have developmental problems that may be obstacles to learning or that place children at risk. Development in infants, toddlers, and preschoolers is characterized by broad variability in rates and patterns of maturation. For some children, differences and delays in abilities are temporary and are resolved during the normal course of development. For other children, delays may persist in different domains of functioning, necessitating the child’s referral for targeted screening and/or comprehensive evaluation ( National Joint Committee on Learning Disabilities, NJCLD, 2005 ).
There is a consensus in the literature that the identification and early prevention of risk students for learning disabilities and attention is a fundamental and important pre-diagnostic procedure in the educational context, since it allows us to influence a high plasticity phase of neurocognitive systems involved in the acquisition of written language at the same time can prevent the development of a school gap too much which causes the low academic performance ( Catts, Fey, Zhang, & Tomblin, 2001 ; Germano & Okuda, 2015 ; Reynolds & Shaywitz, 2009 ; Capellini, Cesar, & Germano, 2015 ; Fletcher & Vaughn, 2009 ).
The students from this study showed an improvement from in task 1 and task 2 from Visual Attention Test Software (TAVIS-4, Duchesne & Mattos, 1997 ; Coutinho, Mattos, Araújo, & Duchesne, 2007 ). In task 1 (Visual Selection Attention Task) the students improved their performance, that consists in making the student to respond selectively to a target stimulus, ignoring the presence of other stimuli (distractors). In task 2 (Visual Alternate Attention Task), the students improved their ability to change the focus of attention among different parameters of the same concept.
However, it was possible to observe that students from this study had difficulties especially in task 3 (Visual Sustained Attention Task) regarding the number of errors by omission and number of errors per action. This task requires the school to remain continuously attentive to the computer screen for a long period of time, aiming to quickly respond to the appearance of a stimulus for all the tasks already mentioned ( Coutinho et al., 2007 ).
The first type of errors (number of errors by omission) was described by Coutinho et al. (2007) has an indicative of attention or selectivity. The second type of errors number of errors per action may be related to impulsivity problem ( Coutinho et al., 2007 ). Slobodin, Cassuto and Berger (2015) described that sustained attention, characterized as the ability to concentrate on a specific stimulus over a period of time, develops slower. Meanwhile, other functions, such as inhibitory control, an important component of executive function that allows for the suppression of actions and resistance to interference from irrelevant stimuli, do not show a clear developmental trajectory.
Studies investigating sustained attention in students with ADHD have rather consistently shown that these students have frequent lapses of attention during continuous performance tasks. In contrast, studies investigating selective attention have shown children with ADHD to have intact selective attention on a variety of tasks, including visual search, visuospatial orienting, perceptual load, and perceptual discrimination-distractibility tasks ( McAvinue et al., 2015 ).
An inability to sustain attention is one of the hallmark symptoms of ADHD. The results of this study were also supported by McAvinue et al. (2015) , who tested 25 students using the Sustained Attention to Response Task (SART). The results showed evidence that students with ADHD showed an impaired ability to sustain attention during the SART, as evidenced by a significantly higher number of errors.
These results were also founded in Tsal, Shalev and Mevorach (2005) . The authors assessed participants with attention-deficit/hyperactivity disorder (ADHD) using four tasks uniquely assessing the functions of selective attention, executive attention, sustained attention, and orienting of attention. The results showed that deficits in sustained attention were the most pronounced, characterizing most participants with ADHD and deficits in each of the other three functions characterized more than half of these participants. Different participants with ADHD revealed different clusters of attentional deficits. These results call for a revision of leading theories of ADHD that identify the core of the pathology as a sole deficit in executive functions
Thus, Stern and Shalev (2013) investigated the relation and impact of sustained attention and the number of correct answers reading performance. The researchers revealed that participants with good sustained attention answered significantly more questions correctly and read the text faster compared to participants with medium sustained attention and compared to participants with poor sustained attention. The authors highlighted that good sustained attention is related to successful reading comprehension not only when comparing good and poor participants in sustained attention but more so when comparing good and average participants in sustained attention.
Studies also have reported the positive effect in attention training over the years. Tamm et al. (2013) referred that researchers have turned to investigate attention training as an intervention for Attention-Deficit/Hyperactivity Disorder (ADHD) since ADHD involves impairment in attention and related executive functions. Furthermore, studies of attention training in ADHD also provide initial support for improvements on untrained measures of attention and academic efficiency.
Likewise, regarding with intervention programs for students with ADHD, Rapport et al. (2013) referred that, of the executive functions and related attentional processes reviewed, only working memory (WM) central executive processes and vigilance/sustained attention abilities were associated with large magnitude deficits and related to core symptoms and/or functional outcomes in children with ADHD.
5. Conclusion
The results of this research point to the need to (re)think the importance of knowledge and identification of the individual profile of abilities and difficulties for each grade level, especially in early years, which literacy plays a great roll. Furthermore, the early identification of students at risk for ADHD in the classroom context favors to contemplate individual needs with early intervention, thereby minimizing the impact of attention and phonological working memory difficulties in reading and writing learning.
The findings of this study showed that the use of the RTI model could be used as an early identification tool for students at risk of attention deficit in the early years of literacy, as the population of this study.
Despite the fact of being a recent study using RTI model in Brazilian population, it is important to highlight that from 106 students, 19 students (59.3%) not responded to intervention. These findings bring an important contribution for public educational policy regarding the need of more studies using RTI model in early grade level. In addition, this highlight the necessity of orientation of teachers and clinicians to ensure the observation of manifestation in school context, the necessity of the application of systematic screenings for early identification and monitoring students progression, and finally, to observe the need of adaptation strategies and implementation of curricular adaptations to encourage these students in academic activities in the classroom.
Acknowledgements
To Brazilian National Council for Scientific and Technological Development (CNPq) for supporting this research (Universal Notice MCT/CNPq number 14/2012).
Cite this paper
Germano, G. D., & Capellini, S. A. (2016). Identification of Stu- dents at Risk for Attention Deficit Disorder with Hyperactivity Using the Response to Intervention Model (RTI). Psychology, 7, 1824-1838. http://dx.doi.org/10.4236/psych.2016.714169
References
- 1. American Psychiatric Association (APA). (1994). Diagnostic and Statistical Manual of Mental Disorders—DSM-IV (4th ed). Washington DC: APA. [Paper reference 1]
- 2. American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5). American Psychiatric Pub. [Paper reference 1]
- 3. Andrade, O. V. C. A., Andrade P. E., & Capellini, S. A. (2014). Response to Intervention Model: RTI: How to Identify and Intervene with Children at Risk for Learning Disorders. São José dos Campos: Pulse Editorial. [Paper reference 2]
- 4. Baddeley, A. D. (1986). Working Memory. Oxford: Oxford University Press. [Paper reference 1]
- 5. Barnes, A. C., & Harlacher, J. A. (2008). Clearing the Confusion: Response-To Intervention as a Set of Principles. Education and Treatment of Children, 31, 417-431.
https:/doi.org/10.1353/etc.0.0000 [Paper reference 2] - 6. Capellini, S. A., César, A. B. P. C., & Germano, G. D. (2015) Early Identification of Reading Problems: Preliminary Study with Students of 1st Grade. Procedia-Social and Behavioral Sciences, 174, 1351-1355.
https:/doi.org/10.1016/j.sbspro.2015.01.758 [Paper reference 2] - 7. Capellini, S. A., Silva, E. C., & Germano, G. D. (2015). The Use of the Response to Intervention Model (RTI) for the Identification of Attention Deficit Hyperactivity Disorder. In: A. C. Machado, K. K. Borges, & S. F. Bello (Eds.), Attention Deficit/Hyperactivity Disorder (ADHD): Clinical and Educational Practice (pp. 119-132). Marília, SP: FUNDEPE Editora, FUNDEPE Publishing. [Paper reference 3]
- 8. Catts, H. W., Fey, M. E., Zhang, X., & Tomblin, J. B. (2001). Estimating the Risk of Future Reading Difficulties in Kindergarten Children: A Research-Based Model and Its Clinical Implementation. Language, Speech, and Hearing Services in Schools, 32, 38-50. [Paper reference 1]
- 9. Coutinho, G., Mattos, P., Araujo, C., & Duchesne, M. (2007). Attention-Deficit/Hyperactivity Disorder: Diagnostic Contribution of a Computerized Assessment of Visual Attention. Archives of Clinical Psychiatry, 34, 215-222.
https:/doi.org/10.1590/S0101-60832007000500003 [Paper reference 7] - 10. Coyne, M. D., & Harn, B. A. (2006). Promoting Beginning Reading Success through Meaningful Assessment of Early Literacy Skills. Psychology in the Schools, 43, 33-43.
https:/doi.org/10.1002/pits.20127 [Paper reference 2] - 11. Duchesne, M., & Mattos, P. (1997). Normatization of a Computerized Visual Attention Test (TAVIS). Archives of Neuropsychiatry, 55, 62-69. [Paper reference 6]
- 12. DuPaul, G. J., Weyandt, L. L., & Janusis, G. M. (2011). ADHD in the Classroom: Effective Intervention Strategies. Theory into Practice, 50, 35-42.
https:/doi.org/10.1080/00405841.2011.534935 [Paper reference 1] - 13. Dyck, M. J., & Piek, J. P. (2014). Developmental Delays in Children with ADHD. Journal of Attention Disorders, 18, 466-478.
https:/doi.org/10.1177/1087054712441832 [Paper reference 1] - 14. Fadini, C. C., & Capellini, S. A. (2011). Efficacy of Phonological Skills Training Program in Children under Risk of Dyslexia. Revista CEFAC, 13, 856-865.
https:/doi.org/10.1590/S1516-18462011005000025 [Paper reference 1] - 15. Fletcher, J., & Vaughn, S. (2009). Response to Intervention: Preventing and Remediating Academic Difficulties. Child Development Perspectives, 3, 30-37.
https:/doi.org/10.1111/j.1750-8606.2008.00072.x [Paper reference 1] - 16. Foundation of Economy and Statistics (2003). índice de Desenvolvimento Socioeconômico (Idese). Porto Alegre: FEE.
http://www.fee.tche.br/sitefee/pt/content/estatisticas/pg_idese.php [Paper reference 1] - 17. Fuchs, D., & Fuchs, L. S. (2006). Introduction to Response to Intervention: What, Why, and How Valid Is It? Reading Research Quarterly, 41, 93-99.
https:/doi.org/10.1598/RRQ.41.1.4 [Paper reference 1] - 18. Fukuda, M. T. M., & Capellini, S. A. (2011). Phonological Skills and Grapheme-Phoneme Training Correspondence in Children under Dyslexia Risk. Revista CEFAC, 13, 227-235.
https:/doi.org/10.1590/S1516-18462010005000074 [Paper reference 1] - 19. Germano, G. D., & Capellini, S. A. (2015). Metalinguistic Skills Evaluation (PROHFON): Characterization and Comparison of Students’ Performance. Psychology: Research and Review, 28, 378-387 [Paper reference 1]
- 20. Germano, G. D., & Okuda, P. M. M. (2015). The Use of the Response to Intervention Model (RTI) for Early Identification of Attention Deficit Hyperactivity Disorder (ADHD) and Developmental Coordination Disorder (DCD). In O. V. C. A. Andrade, P. M. M. Okuda, & S. A. Capellini (Org.), Topics in Learning Disorders—Part IV (pp. 211-222). Marília-SP/Brazil: FUNDEPE: Academic Culture. [Paper reference 2]
- 21. Germano, G. D., Silva, E. C., & Capellini, S. A. (May). The Use of the Response to Intervention Model (RTI) for Identification of Children with Attention Deficit Hyperactivity Disorder (ADHD). II Meeting on Child Development—II IBNequinho. Salvador. [Paper reference 3]
- 22. Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A Research Note. Journal of Child Psychology and Psychiatry, 38, 581-586.
https:/doi.org/10.1111/j.1469-7610.1997.tb01545.x [Paper reference 1] - 23. Gresham, F. M. (2002). Responsiveness to Intervention: An Alternative Approach to the Identification of Learning Disabilities. In: R. Bradley, L. Danielson, & D. P. Hallahan (Eds.), Identification of Learning Disabilities: Research to Practice (pp. 467-519). Mahwah, NJ: Erlbaum. [Paper reference 2]
- 24. Hale, J. B. (2012). Response to Intervention: Guidelines for Parents and Practitioners. USA.
http://www.wrightslaw.com [Paper reference 1] - 25. Haraway, D. L. (2012). Monitoring Students with ADHD within the RTI Framework. The Behavior Analyst Today, 13, 17-21.
https:/doi.org/10.1037/h0100720 [Paper reference 1] - 26. Johnson, E., Mellard, D. F., Fuchs, D., & Mcknight, M. A. (2006). Responsiveness to Intervention (RTI): How to Do It. Lawrence, KS: National Research Center on Learning Disabilities. [Paper reference 3]
- 27. Learning Disabilities Roundtable (2005). Comments and Recommendations on Regulatory Issues under the Individuals with Disabilities Education Improvement Act of 2004, Public Law 108-446. USA.
http://www.copyright.gov/legislation/pl108-446.pdf [Paper reference 1] - 28. Martins, M. A., & Capellini, S. A. (2011). Early Intervention in Students at Risk for Dyslexia: Literature Review. Revista CEFAC, 13, 749-755.
https:/doi.org/10.1590/S1516-18462011005000028 [Paper reference 1] - 29. McAvinue, L. P., Vangkilde, S., Johnson, K. A., Habekost, T., Kyllingsbæk, S., Bundesen, C., & Robertson, I. H. (2015). A Componential Analysis of Visual Attention in Children with ADHD. Journal of Attention Disorders, 19, 882-894.
https:/doi.org/10.1177/1087054712461935 [Paper reference 2] - 30. National Association of State Directors of Special Education (2006). Response to Intervention: Policy Considerations and Implementation. Alexandria, VA: NASDSE Inc. [Paper reference 2]
- 31. National Joint Committee on Learning Disabilities (2005). Responsiveness to Intervention and Learning Disabilities. USA.
http://www.ldonline.org/njcld [Paper reference 1] - 32. Rapport, M. D., Orban, S. A., Kofler, M. J., & Friedman, L. M. (2013). Do Programs Designed to Train Working Memory, other Executive Functions, and Attention Benefit Children with ADHD? A Meta-Analytic Review of Cognitive, Academic, and Behavioral Outcomes. Clinical Psychology Review, 33, 1237-1252.
https:/doi.org/10.1016/j.cpr.2013.08.005 [Paper reference 1] - 33. Refundini, D. C., Martins M. A., & Capellini S. A. (2010). Grapheme-Phoneme Correspondence Training in Students at Risk for Dyslexia. Revista Psicopedagogia, 27, 191-201.
http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S0103-84862010000200005&lng=en&tlng [Paper reference 3] - 34. Reutebuch, C. K. (2008). Succeed with a Response-to-Intervention Model. Intervention in School and Clinic, 44, 126-128.
https:/doi.org/10.1177/1053451208321598 [Paper reference 1] - 35. Reynolds, C. R., & Shaywitz, S. E. (2009). Response to Intervention: Ready or Not? Or, from Wait-to-Fail to Watch-Them-Fail. School Pschology Quaterly, 24, 130-145.
https:/doi.org/10.1037/a0016158 [Paper reference 1] - 36. Roth, F. P., Dougherty, D. P., Paul, D. R., & Adamczyk, D. (2010). RTI in Action: Oral Language Activities for K-2 Classrooms. Rockville, MD: American Speech-Language-Hearing Association. [Paper reference null]
- 37. Sayal, K., Hornsey, H., Warren, S., MacDiarmid, F., & Taylor, E. (2006). Identification of Children at Risk of Attention Deficit/Hyperactivity Disorder. A School-Based Intervention. Social Psychiatry and Psychiatric Epidemiology, 41, 806-813.
https:/doi.org/10.1007/s00127-006-0100-0 [Paper reference 1] - 38. Sayal, K., Merrell, C., Tymms, P., & Kasim, P. (2015). Academic Outcomes Following a School-Based RCT for ADHD: 6-Year Follow-Up. Journal of Attention Disorders, Epub.
https:/doi.org/10.1177/1087054714562588 [Paper reference 1] - 39. Slobodin, O., Cassuto, H., & Berger, I. (2015). Age-Related Changes in Distractibility Developmental Trajectory of Sustained Attention in ADHD. Journal of Attention Disorders, Epub.
https:/doi.org/10.1177/1087054715575066 [Paper reference 1] - 40. Stern, P., & Shalev, L. (2013). The Role of Sustained Attention and Display Medium in Reading Comprehension among Adolescents with ADHD and without It. Research in Developmental Disabilities, 34, 431-439.
https:/doi.org/10.1016/j.ridd.2012.08.021 [Paper reference 1] - 41. Tamm, L., Epstein, J. N., Peugh, J. L., Nakonezny, P. A., & Hughes, C. W. (2013). Preliminary Data Suggesting the Efficacy of Attention Training for School-Aged Children with ADHD. Developmental Cognitive Neuroscience, 4, 16-28.
https:/doi.org/10.1016/j.dcn.2012.11.004 [Paper reference 1] - 42. Tsal, Y., Shalev, L., & Mevorach, C. (2005). The Diversity of Attention Deficits in ADHD the Prevalence of four Cognitive Factors in ADHD versus Controls. Journal of Learning Disabilities, 2, 142-157.
https:/doi.org/10.1177/00222194050380020401 [Paper reference 1]