Surgical Science
Vol.5 No.2(2014), Article ID:42962,3 pages DOI:10.4236/ss.2014.52013
Early Diagnosis and Treatment of Traumatic Diaphragmatic Injuries
1Department of General Surgery, Adıyaman University Training and Research Hospital, Adıyaman, Turkey
2Department of Pediatric Surgery, Faculty of Medicine, Adıyaman University, Adıyaman, Turkey
3Department of Thoracic Surgery, Faculty of Medicine, Adıyaman University, Adıyaman, Turkey
4Department of Radiology, Faculty of Medicine, Adıyaman University, Adıyaman, Turkey
Email: *musaabes@hotmail.com
Copyright © 2014 Feyzi Kurt et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accordance of the Creative Commons Attribution License all Copyrights © 2014 are reserved for SCIRP and the owner of the intellectual property Feyzi Kurt et al. All Copyright © 2014 are guarded by law and by SCIRP as a guardian.
Received January 13, 2014; revised February 5, 2014; accepted February 12, 2014
ABSTRACT
Introduction: Early diagnosis and treatment of injuries of the diaphragm are important both because of high incidence of concomitant injuries and since they may lead to life-threatening intestinal and gastric strangulation in the late term. Herein, cases with diaphragmatic injury that have been diagnosed and operated in the early period after injury or during surgery were presented. Methods: Data of 14 cases, which have been diagnosed with diaphragmatic injury after trauma or during surgical procedure that was performed because of concomitant abdominal or intra-thoracic injury between January 2008 and April 2013, were retrospectively reviewed. Results: Of the traumatic diaphragmatic injuries, 10 (71.4%) have occurred due to penetrating trauma, whereas 4 (28.5%) have occurred due to blunt trauma. Diagnosis was made using I.V. contrast-enhanced whole abdominal and thoracic tomography in all 3 pediatric cases (21.4%) and during surgery in the others (78.5%). Conclusion: All of the diaphragmatic injuries have been accompanied by intra-abdominal or intra-thoracic organ injury that requires surgery. In these cases, the diagnosis was made on suspicion of diaphragmatic injury in the course of surgical procedure performed for concomitant organ injury. Computed tomography was diagnostic for diaphragmatic injuries in the pediatric cases.
KEYWORDS
Trauma; Diaphragmatic Injury; Early Diagnosis
1. Introduction
Although traumatic diaphragmatic injuries (TDI) are rare conditions, early diagnosis and treatment is important. Because TDIs are associated with high incidence of concomitant injuries and lead to life threatening intestinal and gastric strangulation in the late term [1-4]. They are difficult to be diagnosed due to anatomical structure and localization of the diaphragm. The prevalence of preoperative diagnosis is low [5,6]. The subject generally undergoes surgical procedure because of concomitant organ injury and the diagnosis is made during exploration performed on suspicion of diaphragmatic injury in the course of surgical intervention [7]; or the subjects present with diaphragm hernia in the late term [8]. Herein, cases with diaphragmatic injury, which have undergone surgical procedure in early posttraumatic period because of concomitant organ injury and diagnosed during exploration, were presented.
2. Method & Materials
In this study, data of 14 cases, which have been diagnosed with diaphragmatic injury after trauma or during surgical procedure that was performed because of concomitant abdominal or intra-thoracic injury between January 2008 and April 2013, were retrospectively reviewed. The cases underwent diagnostic chest x-ray, abdominal US, or intravenous contrast-enhanced thoracic or abdominal tomography. The cases were evaluated in terms of etiology, age, gender, diagnosis, side of injury, concomitant organ injury, treatment, and early and late complications.
3. Results
The median age of the cases was 37.5 (ranged between 8 and 58 years) years. All patients, except one, were male. Of the TDIs, 10 (71.4%) have occurred due to penetrating trauma, whereas 4 (28.5%) have occurred due to blunt trauma. Blunt traumas have resulted from traffic accidents. Penetrating traumas have occurred due to firearm in one of the adult cases and due to penetrating objects in the other adults, whereas due to penetrating objects in one pediatric case and due to a sharp object that fell accidentally from high in two pediatric cases. Injury was on the left side in 8 (57.1%) and on the right side in 6 (42.8%) cases. It was on the right side in all 3 pediatric cases. Diagnosis was made before surgery in all 3 pediatric cases (21.4%) and during surgery in the others (78.5%). In the pediatric cases, the diagnosis was made using I.V. contrast-enhanced whole abdominal and thoracic tomography. These pediatric cases penetrating injury had hemothorax, pneumothorax and intra-abdominal organ injuries together with a single insertion site (Figures 1 and 2). Other cases underwent surgery due to concomitant life-threatening organ injury and the diagnosis was made during exploration, which was performed on suspicion of diaphragmatic injury in the course of surgical procedure. In these cases, organ injuries were diagnosed via I.V. contrast-enhanced tomography or US. CT was performed in 9 cases and US was performed in one case. Failure in providing hemodynamic stability was the most important indication for surgical intervention. Concomitant organ injury was present in all cases. Seven cases had hepatic injury, 4 cases had splenic injury, one case had gall bladder injury, one case had renal injury, 5 cases had lung injury, 1 case had cardiac injury, 2 cases had head trauma, and one case had femur fracture. Diaphragm injury was repaired depending on the localization of concomitant organ injury. Diaphragm was repaired by thoracotomy in 4 (28.5%) cases with lung injury, cardiac injury and pneumothorax, whereas it was repaired by laparotomy in 10 (71.4%) cases with intra-abdominal organ injury. Diaphragmatic injuries underwent primary repair with either absorbable or non-absorbable suture material. A case with cardiac and lung injuries together with diaphragmatic injury died. No early and late complication was observed in the other cases.
4. Discussion
Diaphragmatic injuries may be mortal due to high inci-

Figure 1. Axial CT section demonstrating pneumothorax and hemothorax in a case with penetrating injury of the diaphragm.
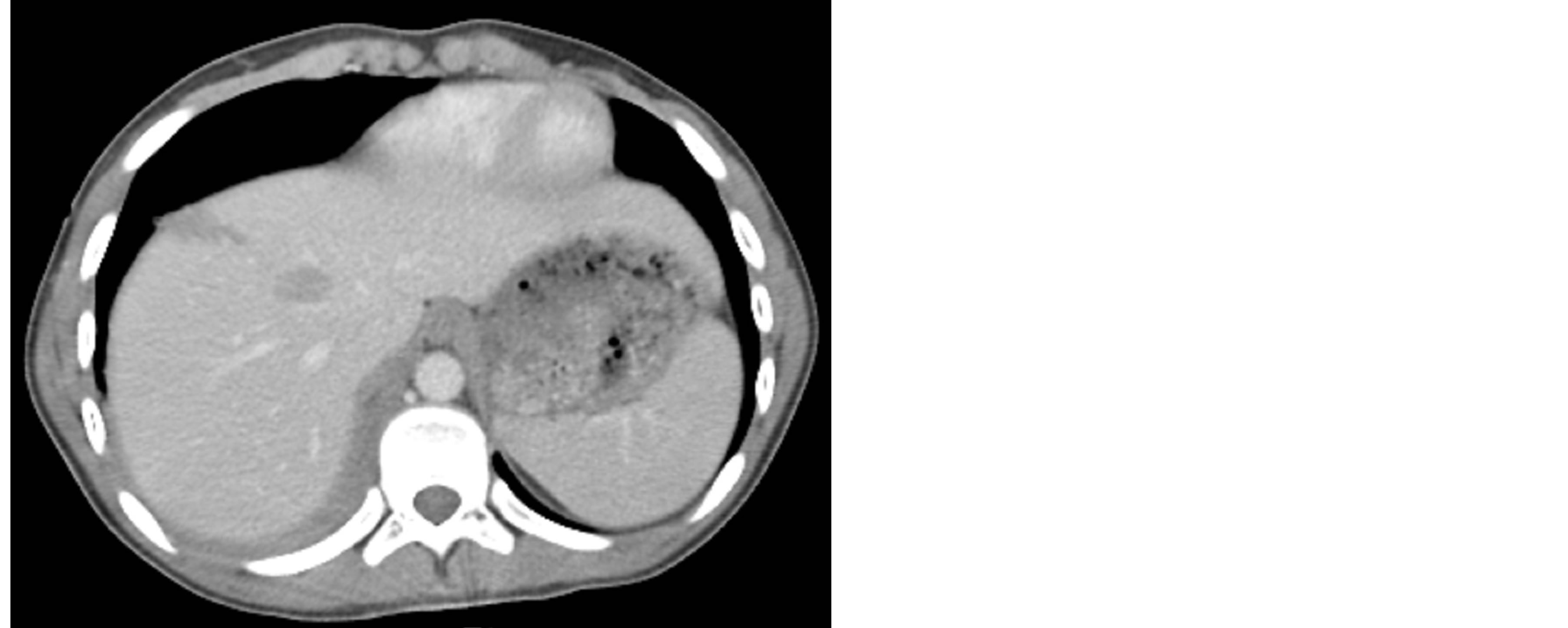
Figure 2. Axial CT section demonstrating hepatic injury in the same case.
dence of concomitant intra-abdominal and intrathoracic injuries in the early period as well as intestinal and gastric strangulation in the late period [4,9,10]. The injury may occur after either a penetrating or blunt trauma. In the literature, the incidence of injuries due to blunt trauma is higher; in the present study, however, the incidence of injuries due to penetrating trauma was higher (63.63%) [8]. It is 3 times more prevalent on the left side versus the right side [3]. Likewise, it was more prevalent on the left side in our cases (72.72%).
It is difficult to demonstrate diaphragmatic injury unless it is accompanied by acute diaphragmatic hernia [2]. Today, whilst the diagnosis is made more commonly by CT, it is made on suspicion of diaphragmatic injury particularly in the cases with thoraco-abdominal injury [1,6]. Diaphragmatic injury is present in 8% of all cases that underwent surgical exploration due to trauma [10]. Since the diaphragm is located between abdomen and thorax, isolated injury of the diaphragm is rare and is usually accompanied by additional organ injury [11]. Diaphragmatic injury should certainly be considered when a lifethreatening organ injury is detected in the cases with thoraco-abdominal trauma [7,8]. All of the present cases were diagnosed in the early period. The diagnosis was usually made during exploration performed routinely on suspicion of diaphragmatic injury in the course of surgical procedure, which was performed due to concomitant injuries such as hepatic, splenic, lung, and cardiac injury (78.57%). In the other 3 (21.42%) cases, the diagnosis was made prior to the surgery detecting organ injury on CT both under and over the diaphragm together with a single insertion site [5]. In these cases, all of which were the pediatric cases, there were both lung, liver, kidney and gall bladder injuries together with a single penetrating insertion site in the thorax or abdomen. The fact that this finding was present only in the pediatric cases might be associated with the size and anatomic structure of children. A penetrating trauma in children can easily reach to the diaphragm and beyond because of weak thoracic and abdominal wall in children. In adults, such an injury requires both much higher energy and much longer penetrating object. Pelvis and long bone fracture is seen by 60% and brain injury is seen by 50% when blunt trauma-induced diaphragmatic injury occurs with high energy [3]. One of our cases with blunt trauma had femur fracture and two cases had brain injury. Early diagnosis is unlikely in isolated injuries of the diaphragm and diagnosis could be made in the late term when strangulation is developed [2]. No isolated diaphragmatic injury was detected in this present series.
Although experimental studies have demonstrated that a part of diaphragmatic injuries is closed spontaneously, it is generally thought that a small diaphragmatic injury is not closed, gradually becomes larger due to the difference between the pressures of thoracic and abdominal spaces, and may lead to intestinal and gastric strangulation [9]. Therefore, diaphragmatic injuries should be repaired as soon as detected [8]. Repair of concomitant life-threatening organ injury is done via thoracotomy or laparotomy depending on the localization of injury [3]. The prevalence of concomitant organ injury reported in the literature changes between 52% and 100% [2,7,10]. All of the present cases had concomitant organ injury. The injury was repaired via thoracotomy in 4 (28.5%) cases with lung injury, heart injury and pneumothorax, whereas it was repaired via laparotomy in 10 (71.4%) cases with intra-abdominal organ injury.
5. Conclusion
The diagnosis of diaphragmatic injury was made before surgery in none of the cases except for pediatric cases. All of the diaphragmatic injuries have been accompanied by intra-abdominal or intra-thoracic organ injury that requires surgery. In these cases, the diagnosis was made on suspicion of diaphragmatic injury in the course of surgical procedure performed for concomitant organ injury.
REFERENCES
- I. Karnak, M. E. Senocak, F. C. Tanyel and N. Büyükpamukçu, “Diaphragmatic Injuries in Childhood,” Surgery Today, Vol. 31, No. 1, 2001, pp. 5-11. http://dx.doi.org/10.1007/s005950170212
- B. S. Powell, L. J. Magnotti, T. J. Schroeppel and C. W. Finnell, “Diagnostic Laparoscopy for the Evaluation of Occult Diaphragmatic Injury Following Penetrating Thoracoabdominal Trauma Injury,” Injury—International Journal of Care of Injured, Vol. 39, No. 5, 2008, pp. 530-534.
- W. C. Hanna and L. E. Ferri, “Acute Traumatic Diaphragmatic Injury,” Thoracic Surgery Clinics, Vol. 19, No. 4, 2009, pp. 485-489. http://dx.doi.org/10.1016/j.thorsurg.2009.07.008
- S. Sözübir, B. Tander, F. Bernay, E. Aritürk, R. Rizalar and N. Gürses, “Traumatic Diaphragmatic Ruptures in Children,” Ulusal Travma Dergisi, Vol. 11, No. 1, 2005, pp. 64-68.
- U. K. Bodanapally, K. Shanmuganathan, S. E. Mirvis, C. W. Sliker, T. R. Fleiter, K. Sarada, L. A. Miller, D. M. Stein and M. Alexander, “MDCT Diagnosis of Penetrating Diaphragm Injury,” European Radiology, Vol. 19, No. 8, 2009, pp. 1875-1881. http://dx.doi.org/10.1007/s00330-009-1367-9
- D. M. Stein, G. B. York, S. Boswell, K. Shanmuganathan, J. M. Haan and T. M. Scalea, “Accuracy of Computed Tomography (CT) Scan in the Detection of Penetrating Diaphragm Injury,” Journal of Trauma, Vol. 63, No. 3, 2007, pp. 538-543. http://dx.doi.org/10.1097/TA.0b013e318068b53c
- C. T. Ramos, B. Z. Koplewitz, P. S. Babyn, P. S. Manson and S. H. Ein, “What Have We Learned about Traumatic Diaphragmatic Hernias in Children?” Journal of Pediatric Surgery, Vol. 35, No. 4, 2000, pp. 601-604. http://dx.doi.org/10.1053/jpsu.2000.0350601
- K. Turhan, O. Makay, A. Cakan, O. Samancilar, O. Firat, G. Icoz and U. Cagirici, “Traumatic Diaphragmatic Rupture: Look to See,” European Journal of Cardio-Thoracic Surgery, Vol. 33, No. 6, 2008, pp. 1082-1085. http://dx.doi.org/10.1016/j.ejcts.2008.01.029
- J. A. Perlingeiro, R. Saad Jr., C. L. Lancelotti, S. Rasslam, P. C. Candelária and S. C. Soldá, “Natural Course of Penetrating Diaphragmatic Injury: An Experimental Study in Rats,” International Surgery, Vol. 92, No. 1, 2007, pp. 1-9.
- W. C. Hanna, L. E. Ferri, P. Fata, T. Razek and D. S. Mulder, “The Current Status of Traumatic Diaphragmatic Injury: Lessons Learned from 105 Patients over 13 Years,” The Annals of Thoracic Surgery, Vol. 85, No. 3, 2008, pp.1044-1048. http://dx.doi.org/10.1016/j.athoracsur.2007.10.084
NOTES
*Corresponding author.