Open Journal of Medical Imaging
Vol.3 No.3(2013), Article ID:37139,3 pages DOI:10.4236/ojmi.2013.33016
Gigantic Nasal Fibroma: CT and MR Imaging Findings with Histopathological Correlation
Department of Radiology, Showa University Northern Yokohama Hospital, Yokohama, Japan
Email: rad.ukisu@gmail.com
Copyright © 2013 Ryutarou Ukisu et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received August 14, 2013; revised August 28, 2013; accepted September 4, 2013
Keywords: Fibroma; Nasal Cavity; CT; MRI
ABSTRACT
A 79-year-old woman with gradually worsening left nasal obstruction, purulent rhinorrhea and severe headaches for 6 months admitted to the hospital. A gray-white and huge mass occupying the left nasal cavity was found in physical examination. CT revealed a soft-tissue-density mass in the left nasal cavity with erosion of adjacent bone structures. On T2-weighted MR images, the lesion showed homogenous extreme low signal intensity. The patient underwent successful surgical removal of huge sinonasal soft tissue mass measuring 50 × 45 × 40 mm. The final diagnosis of fibroma was made histologically. MR imaging studies showed characteristic signal intensities corresponding to histopathological components. To the best of our knowledge, this is the first report regarding the MR imaging findings of huge nasal fibroma in the English literature.
1. Introduction
Fibromas of the upper respiratory tract have been described as polypoid benign lesions, and are classified as fibrous polyps. Fibromas of the upper respiratory tract may originate from previous inflammatory reactions or fibroblast proliferations, which may result in tumors composed of collagen fiber and mature spindle cells. In head and neck region, they occur mostly in the pharynx and larynx, but rarely in the nasal cavity [1,2]. CT of nasal and paranasal sinus reveals the relationship between the tumor and surrounding bony structures. MR imaging provides information on the margin of the tumor more clearly than CT. In addition, T2-weighted MR image revealed characteristic homogenous low signal intensity due to the fibrous component of the tumor.
2. Case Report
A 79-year-old woman had suffered from left nasal obstruction, purulent rhinorrhea and severe headaches for 6 months. The patient did not have any history of sinonasal disease and other associated signs and symptoms such as epistaxis. Physical examination and endoscopy revealed a gray-white, smooth-surfaced, huge firm mass completely obstructing the left nasal cavity and distorting the nasal septum toward the right side. Paranasal sinus CT with bone window showed 51 × 44 × 40 mm soft-tissuedensity mass in the left nasal cavity with erosion of nasal septum and adjacent bones (Figure 1). The mass showed slightly inhomogenous intensity similar to muscle on T1-weighted MR image (Figure 2), and homogenous low signal intensity on T2-weighted MR image (Figure 3). The mass showed inhomogeneous enhancement predominantly peripheral component on gadolinium enhanced T1-weighted MR image. MR imaging also suggested that the tumor arised in the lateral wall of the left maxillary sinus (Figure 4).
The patient underwent surgical removal of the tumor. During the surgery the tumor was found to originate from the lateral wall of the left nasal cavity with a wide-based stalk attachment. Bleeding was mild during the operation and stopped on anterior nasal packing. Complete tumor resection was performed without any complications.
Histopathologically, the tumor was composed of spindle-shaped cells with long nuclei; some areas showed interstitial dense collagen deposits while some others showed abundant hyalinization (Figure 5). There was no evidence of atypical cellularity, necrosis, hemorrhage, or an increase in the number of mitosis. Immunohistochemical staining was negative for CD34, CD99 and
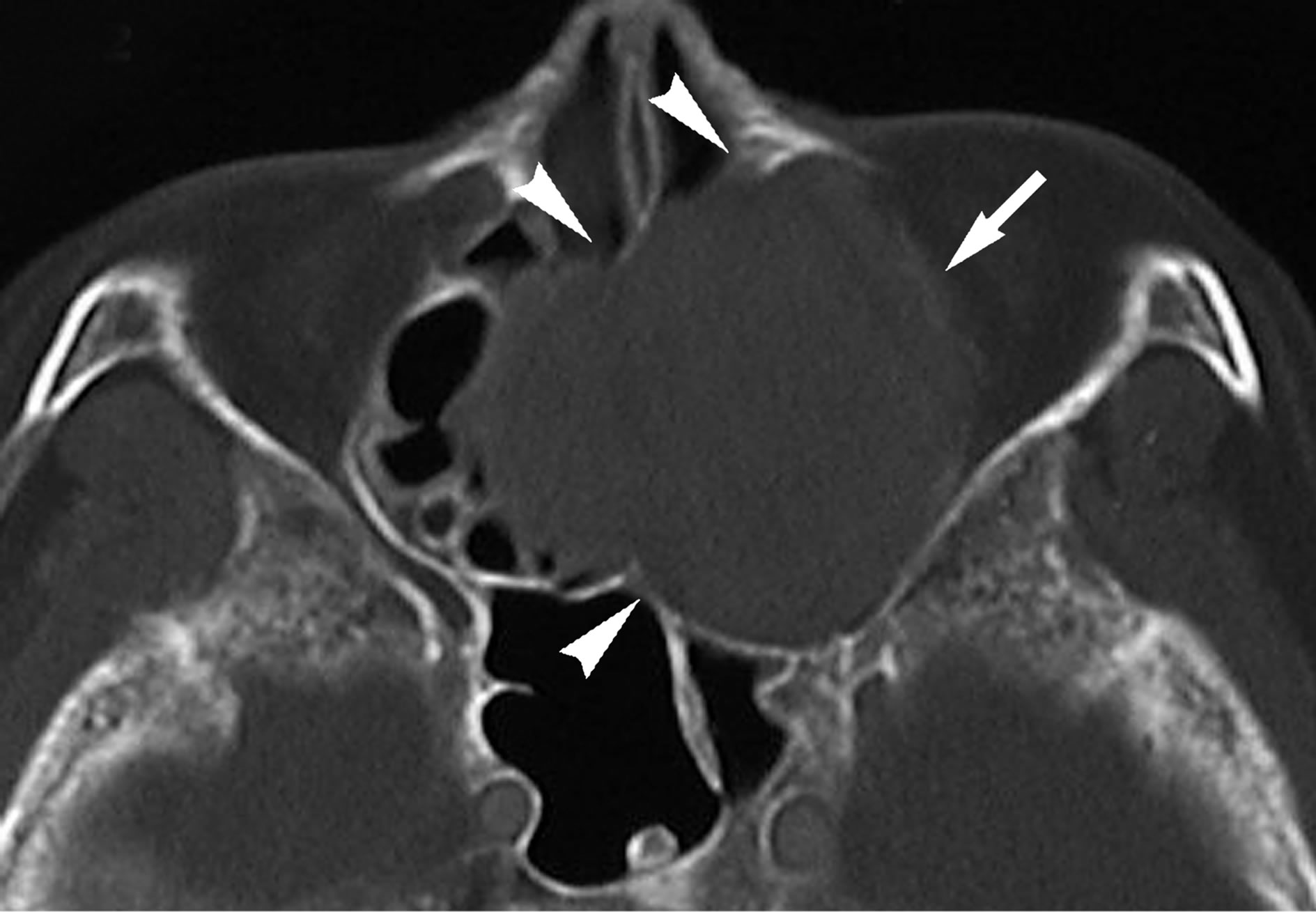
Figure 1. Non-contrast CT at the level of maxillary sinus demonstrates round soft-tissue density mass in the left nasal cavity (arrow). Several degree of bony erosion around the lesion is also observed (arrowheads).
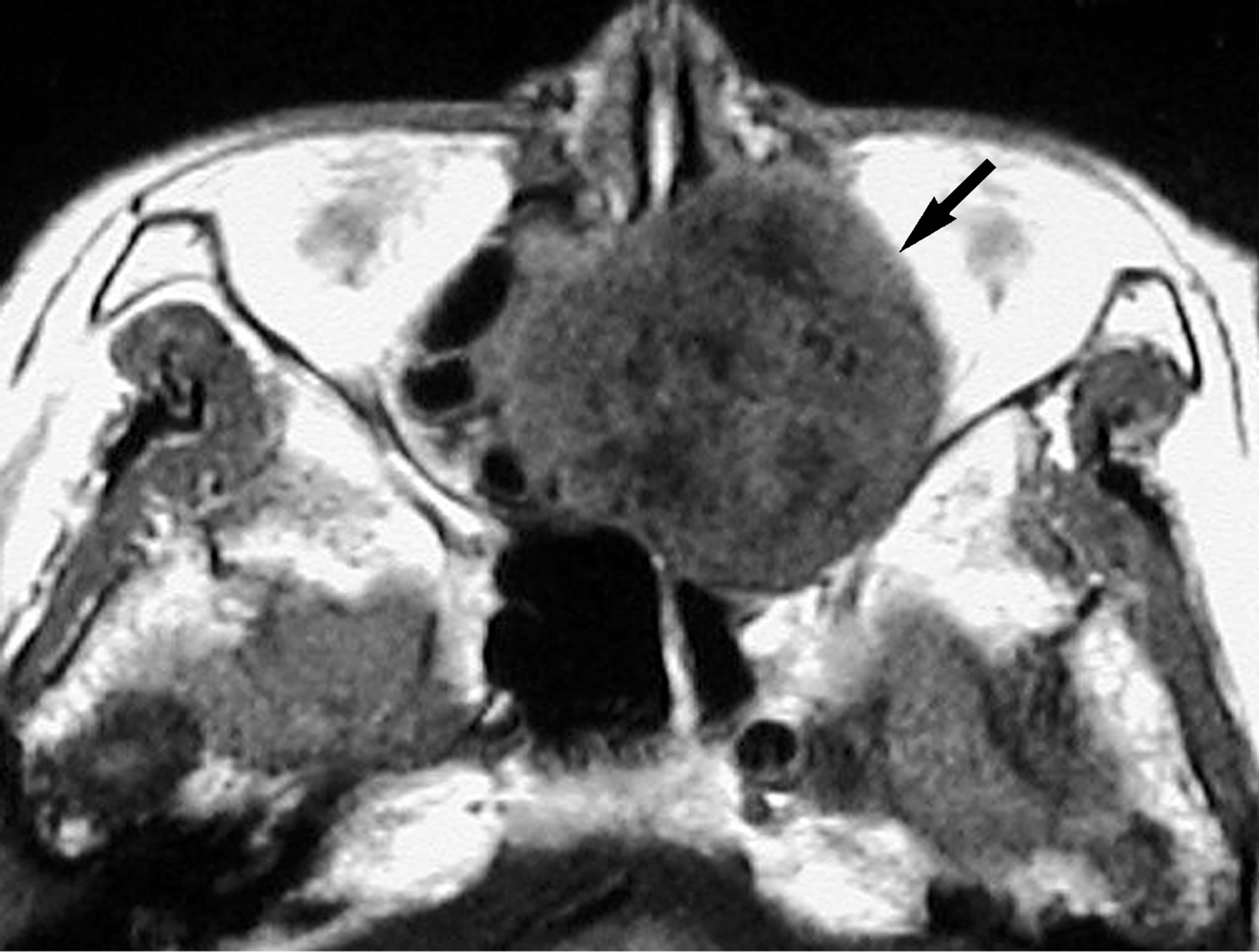
Figure 2. T1-weighted MR image (TR/TE = 460 ms/14 ms) at the same level shows round mass (arrow) in the left nasal cavity. The signal intensity is intermediate and slightly inhomogeneous that is similar to muscle.
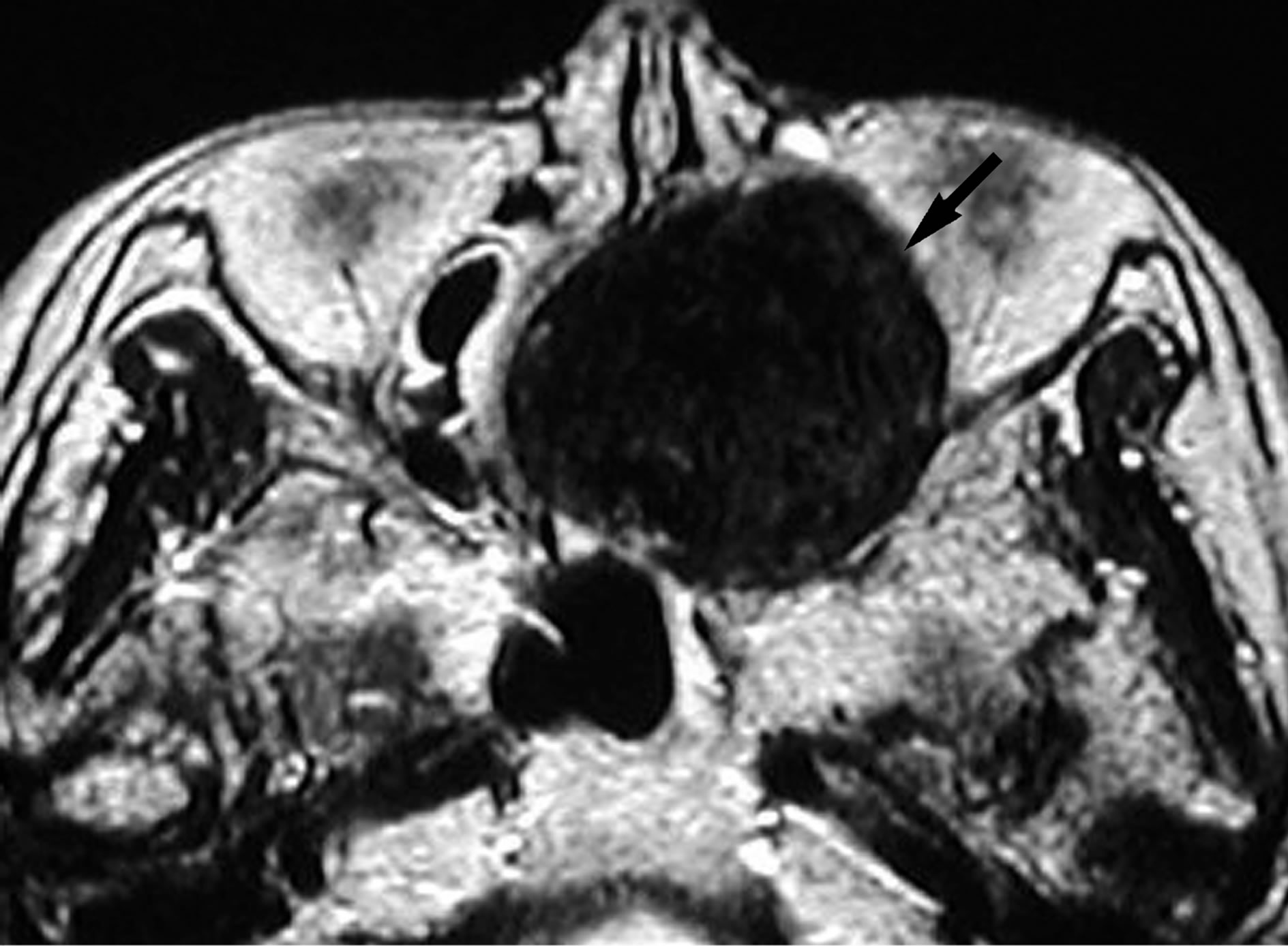
Figure 3. On T2-weighted MR image (TR/TE = 3000 ms/96 ms), the signal intensity of the lesion is uniformly low (arrow).
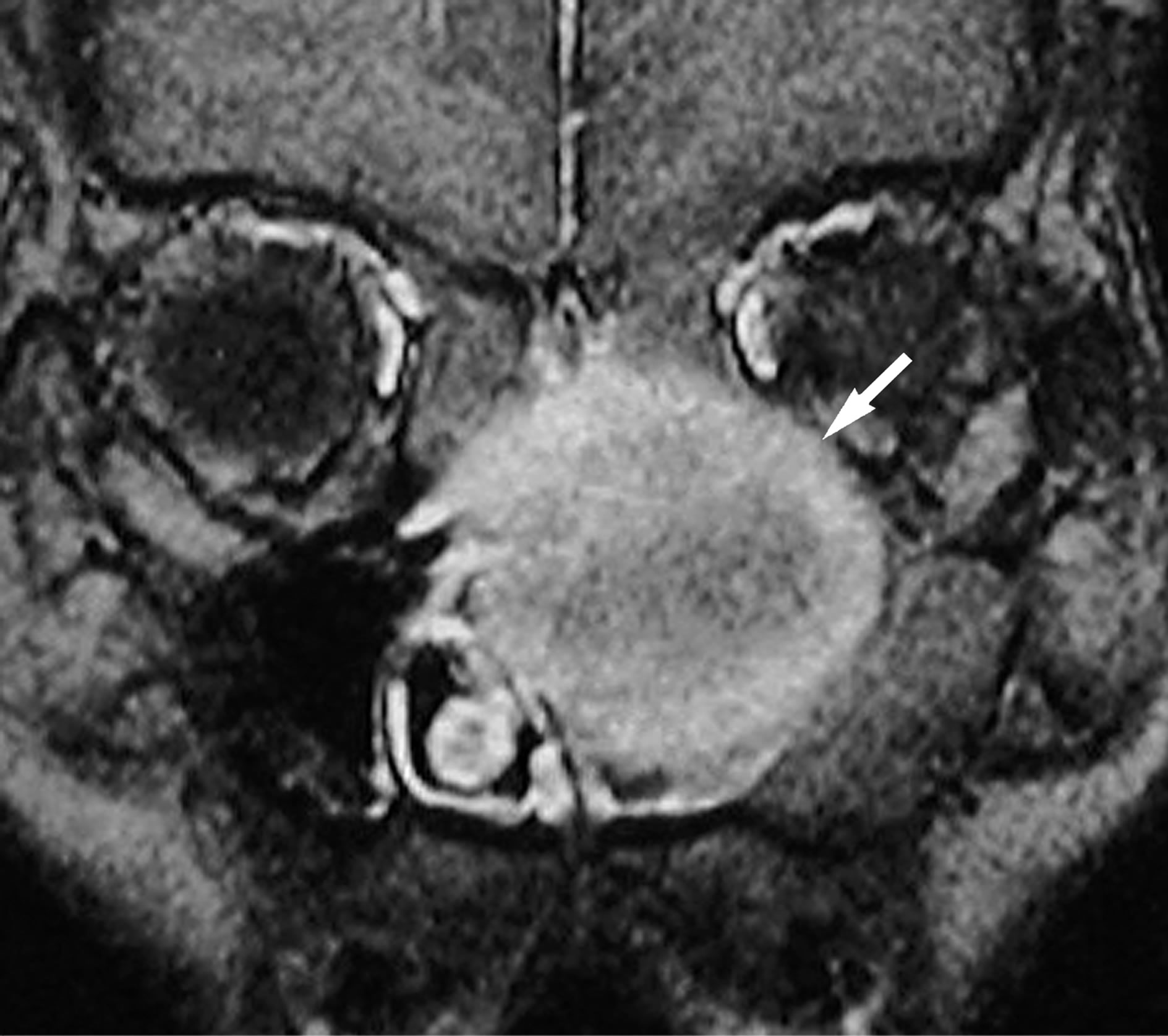
Figure 4. Coronal gadolinium-enhanced fat-saturated T1- weighted MR image (TR/TE = 460 ms/14 ms) shows moderate enhancement predominantly in the peripheral component of the lesion (arrow).
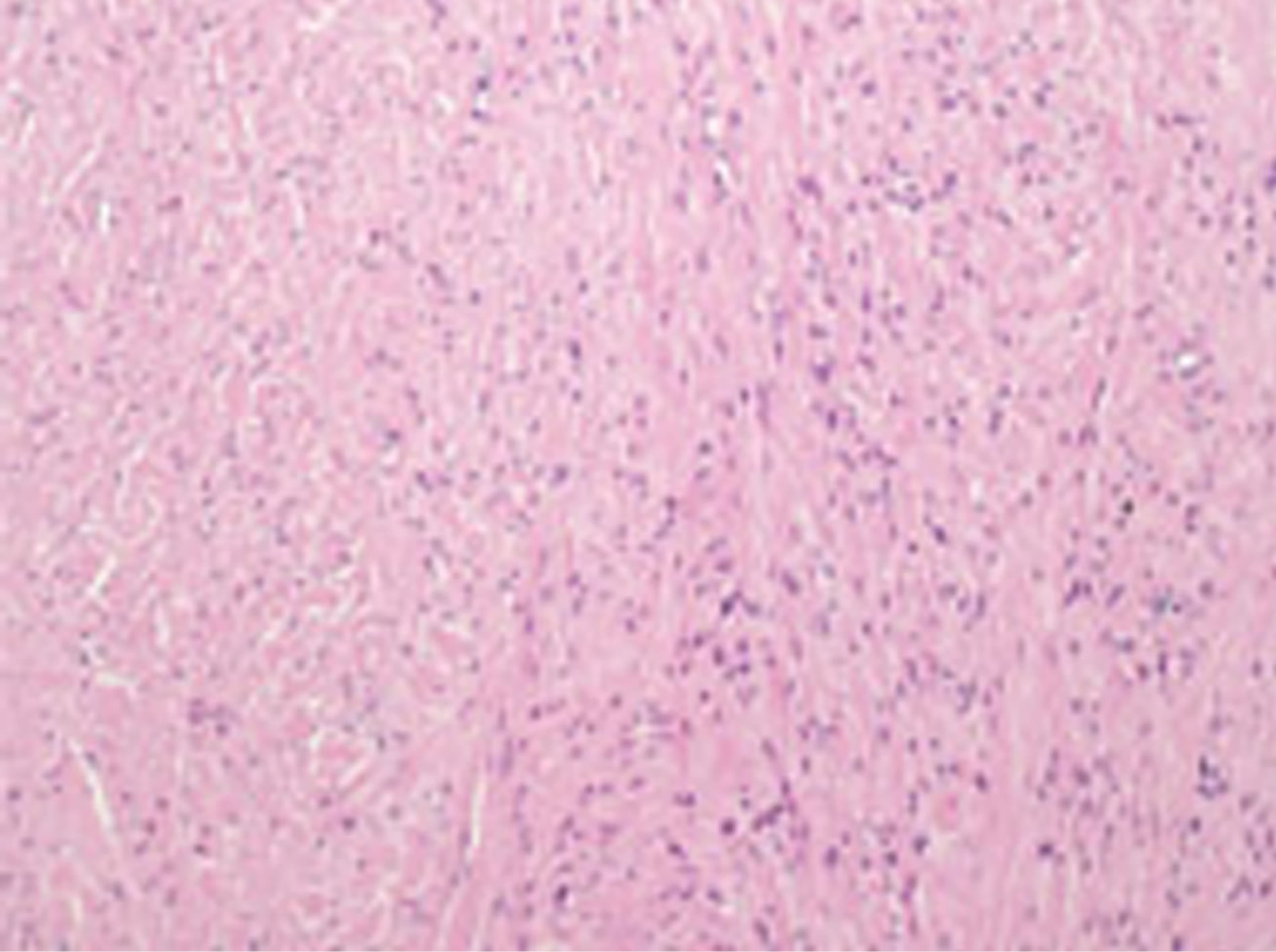
Figure 5. Histological examination shows that the lesion is composed of interlacing bundles of spindle cells with collagen fibers. The specimen reveals neither nuclear pleomorphic, nor mitotic activity, nor necrosis (Haematoxylin and Eosin stain, ×100).
S-100 protein. According to light microscopy and immunohistochemical stain examinations, a diagnosis of huge fibroma of the left nasal cavity was established.
3. Discussion
Fibromas are thought to be a result from progressive inflammation or fibroblastic proliferation of the nasal mucosa. In the nasal cavity, it might also originate from previous polypoid changes or tumors, such as inflammatory polyp [1,2]. They affect all age groups with no predilection to either sex. In 1976, Fu and Perzin reported 256 non-epithelial tumors of the nasal cavity, paranasal sinus and nasopharynx. Only four of the 256 cases were classified as nasal fibroma, and their sizes were smaller than 1 cm in diameter [2]. The tumor is usually remains small and causes no symptom. However, occasionally, they could form a large mass filling in the nasal cavity causing nasal obstruction, rhinorrhea, epistaxis headache, and exophthalmos. Review of the available literature has shown a similar case report of fibroma arising from bony nasal septum. A few cases of fibroma of the nasal cavity arising from the cartilaginous part of the nasal septum have been reported [3-6].
Histologically, these lesions were composed of elongated spindle cells, collagen and hyalinized fibrous tissue [2]. To accurately distinguish between fibroma and the other nasal non-epithelial tumors, immunohistochemical staining such as CD34 staining and CD99 staining is indispensable. No recurrences have been reported following simple local excision.
In our case, the lesion reveals homogeneous soft tissue density on CT. Bone erosion surrounding the lesion is observed, and no calcified area is seen. These findings are non-specific, and the differential diagnosis are numerous and include many causes such as nasal polyp, solitary fibrous tumor, inverted papilloma, neurofibroma and hemangioma as well as other malignant tumors [4]. On the other hand, MR imaging which provides better contrast than CT, showed low signal intensity on T2- weighted images and intermediate signal intensity on T1- weighted images which representing spindle cells, collagen and hyalinized tissue within the tumor. These MR imaging findings are well known for ovarian fibromas [7]. Also, heterogeneous enhancement is common with large ovarian fibromas [8].
The main reason attributed for low signal intensity on T2-weighted MR images are calcification, fibrous tissue, bleeding, effusion from chronic inflammation, fungi, hyper-acute phase hematoma, melanocyte and metal foreign body. Lesions of the nasal cavity showing low signal intensity with irregular border, and irregularity in the low signal intensity on T2-weighted MR images suggest malignant lesions such as synovial sarcoma, malignant fibrous histiocytoma (which has more recently being classified as pleomorphic undifferentied sarcoma) and fibrosarcoma. One exception is malignant melanoma, where the signal intensity homogenous and the margin is clear in some cases. High signal on T1-weighted images, and absence of calcium on CT images in this setting suggest melanoma [9]. Otherwise, fibroma should be suspected.
REFERENCES
- J. E. Ash, M. R. Beck and J. D. Wilkes, “Tumors of the Upper Respiratory Tract and Ear,” In: Atlas of Tumor Pathology, Armed Forces Institute of Pathology, Washington DC, 1964, pp. 273-278.
- Y. S. Fu and K. H. Perzin. “Non-Epithelial Tumors of the Nasal Cavity, Paranasal Sinuses and Nasopharynx. A Clinicopathologic Study VI. Fibrous Tissue Tumors (Fibroma, Fibromatosis, Fibrosarcoma),” Cancer, Vol. 37, No. 6, 1976, pp. 2912-2928.
- R. N. Prasad and R Pandey, “Fibroma of the Bony Part of the Nasal Septum,” Indian Journal of Otolaryngology, Vol. 33, No. 4, 1981, p. 154.
- H. L. Lin, C. C. Huang and T. J. Lee. “Endoscopic Sinus Surgery Treatment for a Huge Sinonasal Fibroma,” Chang Gung Medical Journal, Vol. 27, No. 3, 2004, pp. 233- 237.
- B. K. Roychaudhuri, “Fibroma-Bony Nasal Septum,” Indian Journal of Otolaryngology, Vol. 25, No. 3, 1973, pp. 165-167.
- K. R. Gupta and P. K. Kakar. “Fibroma Nose,” Indian Journal of Otolaryngology, Vol. 21, No. 3, 1969, pp. 135- 137.
- R. N. Troiano K. M. Lazzarini, L. M. Scoutt, R. C. Lange, S. D. Flynn and S. McCarthy, “Fibroma and Fibrothecoma of the Ovary: MR Imaging Findings,” Radiology, Vol. 204, No. 9, 1997, pp. 795-798.
- A. B. Shinagare, L. J. Meylaerts, A. R. Laury and K. J. Mortele, “MRI Features of Ovarian Fibroma and Fibrothecoma with Histopathologic Correlation,” American Journal of, Vol. 198, No. 3, 2012, pp. 296-303. doi:10.2214/AJR.11.7221
- K. Oba, R. Ukisu, K. Kojima, T. Fukushita, N. Usui, M. Baba, M. Suzuki, H. Fujisawa, H. Takenaka and T. Kushihashi. “Abnormal Low Intensity on T2-Weighted MR Images in Head and Neck Tumors and Tumorlike Conditions,” The 25th International Congress of Radiology, Marrakesh, 5-8 June 2008, p. 171.