Open Journal of Anesthesiology
Vol.2 No.3(2012), Article ID:20569,5 pages DOI:10.4236/ojanes.2012.23019
Introduction of a New Concept of Pain Management during Labor and a Novel Technique for Pain Free Labor
![]()
Wyckoff Heights Medical Center, New York, USA.
Email: ilyako2000@yahoo.com
Received April 3rd, 2012; revised May 8th, 2012; accepted June 1st, 2012
Keywords: Pain Free Labor; Blockade of 2nd Stage of Labor; Combined Spinal Epidural (CSE); Hyperbaric Tetracaine; Saddle Block
ABSTRACT
Traditional labor epidural techniques have not been proven to be sufficient to cover the second stage of labor. We have developed a new concept of pain management during labor and a new technique that provides sufficient analgesia for second stage of labor. Combined Spinal Epidural with long lasting saddle block (with hyperbaric tetracaine) was used. Potentially pain free labor could be achieved by using this method. Utilizing hyperbaric Tetracaine intrathecally may provide a long lasting sensory sacral blockade. Primary outcome measure was absence of pain during pushing (2nd stage of labor). Patients received additional comfort during 1st stage of labor. Sample size included all patients that requested labor epidurals since 12/22/11 when this new technique was introduced.
1. Introduction
1.1. Background
We designed this observational study to examine whether a new technique, Combined Spinal Epidural (CSE) with long lasting saddle block, will improve labor analgesia for second stage of labor when compared to a traditional epidural technique without saddle block. It’s based on our new concept of labor pain management.
1.2. Methods
Ninety eight parturients were randomly assigned to receive a standardized epidural technique or CSE with long lasting saddle block. After placement of 17 g Touhy needle 19 g epidural catheter was introduced and epidural infusion of Bupivacaine 0.0625% and Fentanyl 2 mcg/ml started. In CSE after placement of 17 g Touhy needle 27 g Whitacre needle was placed, 0.6 ml of 0.66% Tetracaine in 8% Dextrose was injected intrathecaly. The same epidural infusion was started. Patients were left in sitting position for 15 - 20 min for saddle block to settle. The presence of sacral analgesia and pain scores were compared between group using prepared questionnaire.
1.3. Results
In demographically similar groups, parturients with CSE and long lasting saddle block did not feel discomfort on Foley catheter insertion, no discomfort on during vaginal exams, no pain during pushing at second stage, no pain on lacerations or episotomies, no local anesthetics were needed for repaires.
1.4. Conclusions
Combined Spinal Epidural (CSE) with long lasting saddle block provides additional comfort during first stage of labor and reliable analgesia for second stage of labor. It allows practicaly pain free labor. This technique proves our new concept of labor pain management.
2. Main Text
Traditional labor epidural techniques have not been proven to be sufficient to cover the second stage of labor [1-3]. According to different sources sacralization using traditional epidural occurs from 2% to 68% of cases [1-5]. Rate of sacralization that occurs is not reliable, it takes significant time, it rarely provides enough analgesia for second stage of labor. Methods of defining sufficient “sacralization” varies from pin prick tests [3] to verbal questioning about “pain at delivery” [1]. For example statement like this: “Sacral sparing was defined as pain perceived by the patient at delivery despite adequate topup dose administration, or pain necessitating perineal local anesthetic administration for delivery. Top-up doses for second-stage delivery consisted of 5-ml increments of 0.25% bupivacaine up to 10 ml, then 5-ml increments of 2% lidocaine or 2-chloroprocaine if needed up to 10 ml” [1]—does not take in consideration that 2% lidocaine will create motor block that will prevent patient to push and will increase length of second stage of labor (addressed on p. 334 in [6]). In many institutions, including our epidural infusion is often shut off by obstetricians to minimize motor block and facilitate pushing. Local anesthetic are required for episotomies or laceration repair. Traditional epidural will not provide sufficient analgesia when cervical dilatation 8 cm or more. Anesthesiologist often finds himself in awkward situation during second stage of labor—administration of stronger concentration of local anesthetic (2% lidocaine) will provide sacralization, but will create significant motor block when patient can not push. What is the crux of the problem?
In order to find solution we looked into the problem. Labor has 2 stages (we include delivery of placenta into 2nd stage). First stage is contraction of uterus till cervix is open, second is passing of fetuts through vagina. Two stages are different in character of pain, morphology of nerve fibers that transmit pain, pathways thru which pain stimuli reach to the spinal cord, and level in the spinal cord where dorsal nerve root enter into CNS. Pain during first stage of labor is perceived as bad cramps, its visceral, poorly localized pain. It is transmitted by C-fibers, unmielinated, these fibers that are relatively easy to block. They enter spinal cord at level of T10-L1. Pain during second stage, “pushing”, is completely different. Passing of fetus through vagina creates franc damage to tissues— its somatic pain, localized, transmitted by A-delta fibers (through pudendal nerves), that are relatively difficult to block, they enter spinal cord on level S2-S4. In order to provide sufficient analgesia we need 2 different blocks for 2 different stages.
As we mentioned before traditional epidural provides sufficient analgesia for 1st stage of labor, but there is no clarity in realizing that it is conceptually wrong for management of 2nd stage of labor. Epidural is placed on the level L4L5 where motor neurons are and adding high concentration local anesthetic (like this for example: Sacral sparing was defined as pain perceived by the patient at delivery despite adequate top-up dose administration, or pain necessitating perineal local anesthetic administration for delivery. Top-up doses for second-stage delivery consisted of 5-ml increments of 0.25% bupivacaine up to 10 ml, then 5-ml increments of 2% lidocaine or 2-chloroprocain [1]—will inevitably create motor block that will paralyze the patient, will increase length of second stage and will frustrate obstetrician. Ideally it’s not only comfort of the patient, its absence of motor block and ability to push. Lower concentrations (0.125% bupivacaine [3] that do not provide motor block are not enough to provide analgesia for 2nd stage. Epidural opiods by themselves are not enough to provide sufficient analgesia even for 1st stage. Only sacral or saddle block (S2S4) can provide sufficient analgesia for second stage without any motor block. It was offered and proposed in literature (p 336 in [6]), but practical application was not found. (application of spinal hyperbaric bupivacaine or lidocaine for saddle block for vaginal delivery requires removal of existing epiural and not done in practice). Double-catheter technique (p 336 in [6]), lumber and caudal, is cumbersome and is not used in practice. One of the reasons that easy practical solution was not found and looked for—lack of realization by anesthesiaologists that it is conceptually wrong to expect sufficient coverage of 2nd stage of labor from traditional epidural technique without motor block, and lack of awareness that long lasting anesthetic (used for saddle block) like tetracaine or etidocaine will last till second stage. Another blind spot that we found in common practice is lack of awareness by anesthesiologists that patient can benefit from saddle block even in 1st stage of labor, since epidural is placed. Why? Most unpleasant parts of labor are vaginal examinations, Foley placement, intrauterine monitors placement. Traditional epidural does not relieve discomfort from these procedures. Our technique does.
New Concept of Pain Management during Labor
We would like to present our concept of pain management during labor. Considering differences in 2 stages of labor (mentioned before) we realized that there should be 2 different blocks that require 2 different noncommunicating anatomical spaces to prevent motor block (communication on level L4L5 will create motor block) and give ability to use 2 different medications in different concentrations. One would be epidural T10L1 block with diluted local anesthetic (0.0625% - 0.125% bupivacaine). It does not create motor block. Second block should be be saddle block, performed thru spinal needle using hyperbaric Tetracaine (or other very long acting local anesthetic). It’s long lasting (see this article), it is purely sensor block (S2S4). 27 g Spinal needle that we used during CSE is not creating opening big enough for 2 spaces to communicate [1]. Dural puncture technique [3] that was offered before conceptually wrong, because its goal to create communication between spinal and epidural space, and because it’s on the level L4L5 motor block is unavoidable.
Another part of new concept its a realization of need of saddle block during 1st stage of labor, in time of epidural placement and on going, only in this way sever discomfort of vaginal examinations, Foley insertion, intrauterine placement could be relieved. This need was ignored by all other methods that we found in literature.
We understand that length of Tetracaine action that described in literature is around 5 hours. In our experience with this new technique we found it can last up to 12 hours. We can suggest for explanation that sacralisation that develops through epidural infusion somehow prolongs length of tetracaine saddle block. More studies are needed to explain this phenomenon.
Other long acting local anesthetics could be concidered, like Etidocaine or new long acting neurotoxins.
Another part of new concept is use of CSE. Exellent detailed descriptions of this technique could be found in these works [1,3]. Purpose for what its used and advantages (in mentioned articles) that CSE gives are earlier onset of analgesia (if intrathecal lypophilic opioids used like Fentanyl or Sufentanyl), more precise epidural needle placement, and better sacralization if spinal needle 25 G or bigger was used. We look at CSE from completely different angle. For us its method to provide long lasting saddle block through spinal needle and use 2 different noncommunicating anatomical spaces (needle 27 g or smaller should be used).
We hope that more reasonable look at pain management of labor, using this new concept and implementation of this new technique will allow introduction of pain free labor in common practice .
We have developed a technique that provides sufficient analgesia for second stage of labor and avoids unnecessary motor block. Potentially pain free labor could be achieved by using this method. Utilizing hyperbaric Tetracaine intrathecally may provide a long lasting sensory sacral blockade. Primary outcome measure was absence of pain during pushing (2nd stage of labor). Sample size included all patients that requested labor epidurals since 12/22/11 when this new technique was introduced.
3. Methods
After IRB approval and informed consent, 98 parturients with singleton, vertex presentation fetuses at 38 - 42 weeks gestation in active labor received CSE. 98 parturients received a Combined Spinal Epidural (CSE) technique in the sitting position with a 17 gauge Touhy needle, 27 gauge Whitacre spinal needle and Tetracaine 4 mg in 8% dextrose (0.6 ml of 0.66% solution). We were unable to find premixed hyperbaric Tetracaine. We prepared hyperbaric Tetracaine by mixing 2 ml of 1% of preservative free Tetracaine (Akorn Inc.) with 1 ml of 25% sterile Dextrose (from 10 ml premixed syringes by Hospira). It will result in 0.66% Tetracaine in 8% dextrose. After successful placement of needles and epidural catheter, 10 ml of 0.0625% Bupivicaine and Fentanyl 2 mcg/ml was given and a patient controlled epidural analgesia (PCEA) was initiated. Patients were left in a sitting position for 20 minutes in order for saddle block to settle, no discomfort was reported by patients during this period. The effects of sacral block were evaluated by of absence of pain on Foley insertion, absence of discomfort on vaginal examination and need for local anesthetic for episiotomy or laceration repairs. Potential motor block was assessed by asking parturients to move their legs 30 min after CSE placement. Control group consistent of 52 parturients where in sitting position a 17 gauge Touhy needle was placed, epidural catheter inserted, and PCEA with 0.0625% Bupivacaine and Fentanyl 2 mcg/ml was initiated, 10 ml/h, the demand dose was 10 ml q 30 min, it’s a standard technique used in our institution.
The Following Questions Were Asked
Ø Did the patient feel any pain or discomfort during Foley insertion?
Ø Was there a difference between vaginal exams before and after sacral block?
Ø Was there any pain during pushing?
Ø Was there any pain for episiotomy or laceration repair?
Ø OBs and midwives were asked if local anesthetics were needed for episiotomy or laceration repair?
4. Results
22 patients whose labor ended in a C section were excluded from the study. We found that of the remaining 76 patients there was 0/76 patients complaining of pain on Foley insertion, 0/76 patients complained of discomfort during vaginal exam, 0/76 patients complained of pain during second stage of labor. No local anesthesia had to be administered for episiotomy or repairs. The duration of sacral block ranged from 2 h to 12 h. No motor block developed 30 min after CSE placement. No other side effects were noted.
In control group none of the patients had relief of pain during Foley insertion, none of them had relief of discomfort during vaginal examination, all of them had pain during pushing, all of episiotomies or lacerations needed local anesthetic for repair, all of control group had pain if episiotomies or lacerations occurred.
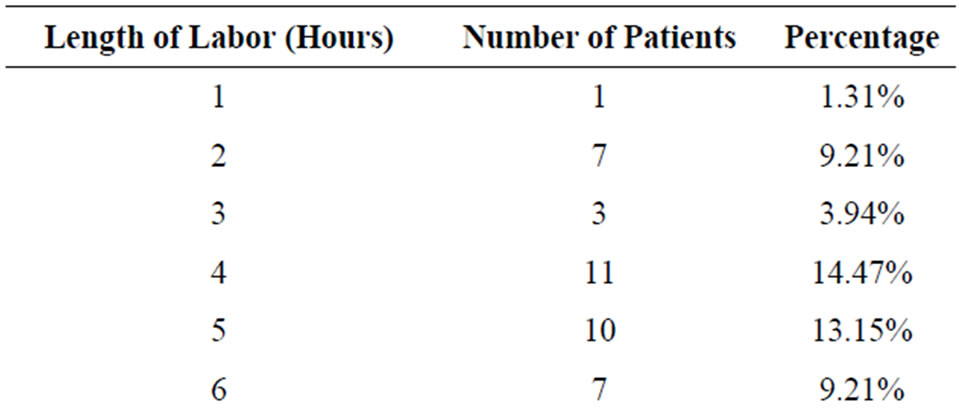
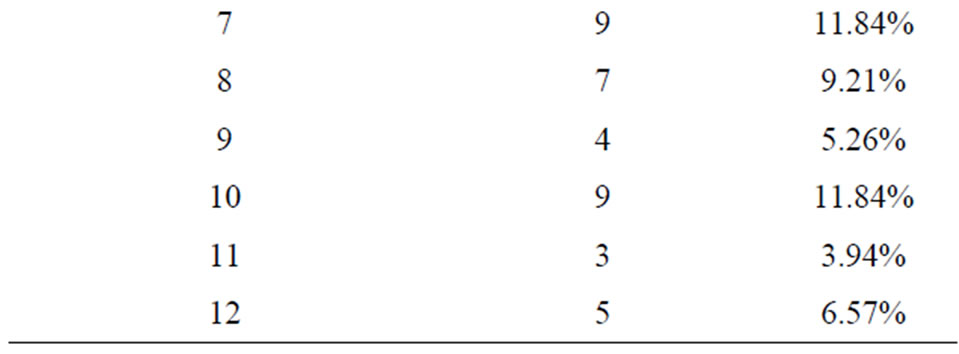
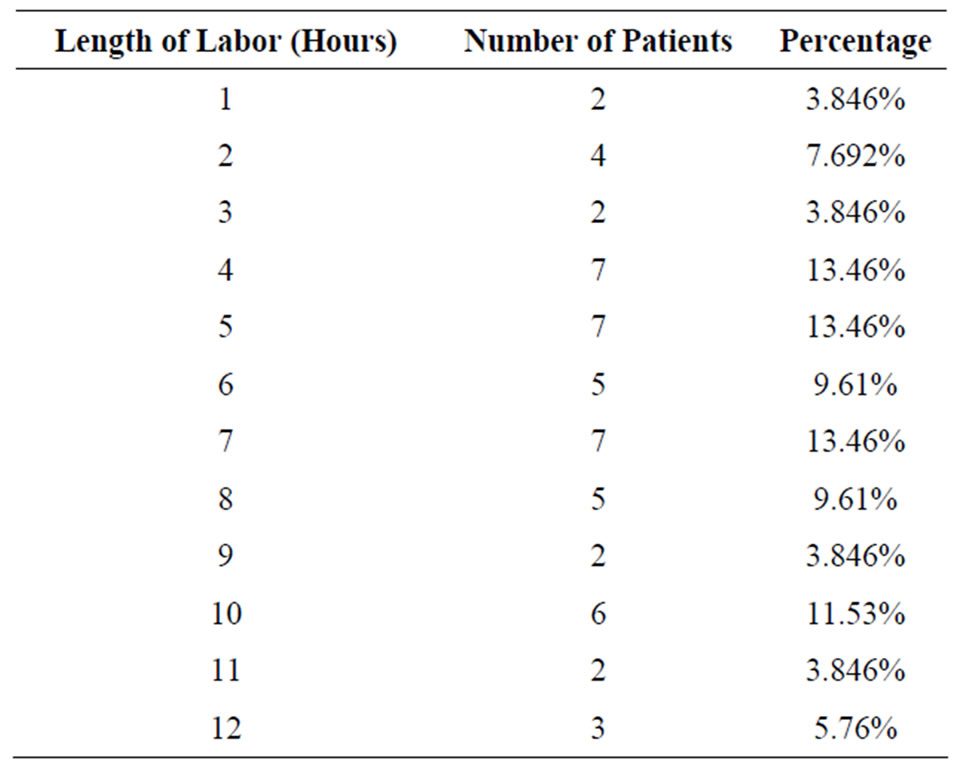
No significant difference in the length of labor was found in both groups.
Length of labor, patients with saddle block:
Length of labor patients with traditional epidural:
5. Conclusions
Utilizing 4 mg of hyperbaric Tetracaine in a CSE technique provided excellent analgesia of sacral region for both first and second stage of labor. A second benefit which was noted was the absence of pain during subsequent episiotomy repair.
Combined Spinal Epidural Anesthesia (CSEA) has become the preferred technique for providing analgesia to laboring parturients. There are various techniques involved with CSEA but the goals are rapid onset of analgesia, minimal motor blockade and high patient satisfaction. Utilizing a spinal needle in this technique has been shown to reduce epidural failure.
Traditional method of CSEA analgesia has been to administer a small amount of narcotic intrathecally. This results in good analgesia for the patient without motor blockade. Disadvantages of this technique include pruritis, fetal bradycardia, no effect on second stage of labor, and short duration of action. A novel method for the intrathecal component is to administer a small amount of hyperbaric Tetracaine to create a sensory sacral block. The main advantages of this technique include fast onset of action and the ability to block the pain of second stage of labor with a long duration of action. Avoiding narcotics precludes the typical pruritis associated with the CSE.
Anesthesiologists traditionally have been able to provide effective relief during the first stage of labor but no practical method utilized can decrease pain during the second stage of labor (Methods that were offered—dural puncture technique, repeated doses of top-off with 0.25% bupivacaine, or others are not reliable, take several hours to start working, ineffective in short labor). Anesthesiologists may have a blind spot concerning pain relief during the second stage of labor. This method addresses this blind spot. Education of anesthesiologist in this area, coming to terms that existing traditional epidural is not efficient in covering second stage of labor, more reasonable approach to management will be needed to spread use of this technique and improve its operating frequency.
Any parturient that is suitable for traditional epidural should be suitable for CSE with long lasting sacral block.
6. Discussion
Traditional labor epidural techniques are not sufficient to cover the 2nd stage of labor. Giving more local anesthetic thru the epidural catheter to create analgesia for 2nd stage of labor will inevitably cause motor blockade and the patient will not be able to push. This prompted us to develop a technique that provides adequate sensory sacral blockade without a motor block. This could be easily accomplished by administering 4 mg hyperbaric Tetracaine for the spinal component of the CSE. In these 76 patients there was absence of pain on Foley insertion, vaginal examinations, and during the complete 2nd stage of labor. Further, no local anesthesia had to be administered for any episiotomy or laceration repairs. We believe this technique warrants further evaluation.
Extended length of Tetracaine saddle block (6 - 12 hours) found in our case can be explained combined use of PCEA with top-offs [1,4]. More studies are needed to explain this phenomenon.
We hope that more reasonable look at pain management of labor, using this new concept and implementation of this new technique will allow introduction of pain free labor in common practice .
REFERENCES
- J. A. Thomas, P. H. Pan, L. C. Harris, M. D. Owen and R. D’Angelo, “Dural puncture with a 27-gauge Whitacre needle as part of a combined Spinal-Epidural Technique Does Not Improve Labor Epidural Catheter Function,” Anesthesiology, Vol. 103, No. 5, 2005, pp. 1046-1051.
- S. W. Simmons, A. M. Cyna, A. T. Dennis and D. Hughes, “Combined Spinal-Epidural versus Epidural Analgesia in labour,” Cochrane database of systematic reviews, Vol. 3, 2007, Article ID: CD003401.
- E. Cappiello, N. O’Rourke, S. Segal and L. C. Tsen, “A Randomized Trial of Dural Puncture Epidural Technique Compared with the Standard Epidural Technique for Labor Analgesia,” Anesthesia & Analgesia, Vol. 107, No. 5, 2008, pp. 1646-1651.
- R. W. Yarnell, D. A. Ewing, E. Tierney and M. H. Smith, “Sacralization of Epidural Block with Repeated Doses of 0.25% bupivacaine during labor,” Regional Anesthesia & Pain Medicine, Vol. 15, No. 6, 1990, pp. 275-279.
- S. Torvaldsen, C. L. Roberts, J. C. Bell and C. H. RaynesGreenow, “Discontinuation of Epidural Analgesia Late in labour for reducing the Adverse Delivery Outcomes Associated with Epidural Analgesia,” Cochrane database of systematic reviews, Vol. 18, No. 4, 2004, Article ID: CD004457. doi:10.1002/14651858.CD004457.pub2
- D. Chestnut, “Obstetrical anesthesia,” 3rd edition, Mosby, Maryland Heights, 2004.