Open Journal of Gastroenterology
Vol. 2 No. 3 (2012) , Article ID: 22039 , 4 pages DOI:10.4236/ojgas.2012.23025
Parenteral erythromycin for potential use to empty retained gastric contents encountered during upper gastrointestinal endoscopic procedures*
![]()
1Department of Anesthesia, Saint Louis University School of Medicine, St. Louis, USA
2Division of Gastroenterology and Hepatology, Saint Louis University School of Medicine, St. Louis, USA
Email: #agarwalb@slu.edu
Received 14 June 2012; revised 18 July 2012; accepted 29 July 2012
Keywords: Erythromycin; Endoscopy; Gastric Contents
ABSTRACT
Background: Erythromycin, a prokinetic agent facilitates gastric emptying. We report our experience with the use of IV erythromycin for emptying retained gastric contents encountered during elective upper gastrointestinal endoscopy (UGIE) procedures in an effort to complete of the procedure on the same day. Patients and methods: This retrospective case series includes 15 patients who were found to have a signifycant amount of retained gastric contents while undergoing an UGIE procedure. After aborting the procedure, a repeat endoscopic examination was performed 30 - 120 minutes following administration of 250 - 500 mg erythromycin intravenously. Results: During repeat endoscopy, ten patients had complete emptying of the gastric contents, three patients had partial emptying and in two patients the amount of residual contents was largely unchanged. Both these patients were later found to have high grade mechanical gastric outlet obstruction. No anesthesia or procedure related complications were noted. Conclusion: Parenteral erythromycin can rapidly empty retained gastric contents encountered during UGIE procedures in a significant proportion of patients. Erythromycin can potentially be tried for safe completion of procedure on the same day.
1. INTRODUCTION
Peri-operative pulmonary aspiration (PPA) is a dreaded complication in patients who undergo anesthesia, especially so in patients requiring emergent surgery or those with delayed gastric emptying [1,2]. Despite adequate preprocedure fasting, retained food in stomach is not inferquently encountered during endoscopy and usually leads to aborting the procedure. Procedure cancellation and postponement can sometimes lead to inordinate treatment delay or inconvenience to the patients and their families. The ability to rapidly empty gastric contents in these patients could potentially allow the performance of the procedure later on the same day and minimize the problems due to cancellation and rescheduling.
Gastric pro-kinetic agents including erythromycin are often used prior to sedation to facilitate gastric emptying in certain high risk patients [3]. However, the supporting data for this use is indirect and largely based on patients with an average risk for PPA [4,5]. In this case series, we report our experience with intravenous erythromycin for emptying gastric content retained despite overnight fasting, in patients who were scheduled to undergoing an elective upper gastrointestinal endoscopic procedure.
2. PATIENTS AND METHODS
This is a retrospective study involving patients who underwent upper gastrointestinal endoscopic (UGIE) procedures in our endoscopy unit after January 2004. After obtaining approval from the institutional review board of the Saint Louis University School of Medicine, the medical records of patients who had received intravenous erythromycin in an effort to empty retained gastric contents during UGIE procedure were reviewed. Careful attention was paid to the medical conditions and the medications that are known to be associated with delayed gastric emptying. In addition, endoscopic findings before and after the administration of intravenous erythromycin, time to repeat endoscopic examination, and dose of erythromycin used were recorded.
All patients scheduled for UGIE in our unit are advised to fast overnight (minimum of 6 hours). The fasting interval was confirmed by an endoscopy nurse and an anesthesiologist independently at the time of registration and again during pre-procedure evaluation. A detailed medical history including a list of medications was taken by a physician’s assistant or a nurse practitioner at the time of scheduling the procedure and again by the anesthesiologists during pre-anesthesia evaluation.
During endoscopy, if we encountered significant amount of residual gastric contents (solid food) that could potentially interfere with adequate examination and increase the risk of aspiration, we immediately withdrew the endoscope and terminated the procedure. Patients then received Erythromycin (250 or 500 mg) intravenously in the patients’ holding area and were brought back to the procedure room 30 - 120 minutes after the infusion was completed depending upon the availability of the procedure room. Under conscious sedation, the stomach was then re-examined with a forward viewing endoscope for residual gastric contents prior to proceeding with the remaining part of the procedure. Inpatients who failed to empty the gastric contents after IV erythromycin, the procedure was aborted and the patients were brought back for endoscopy after 48 hours of clear liquid diet followed by12 hour fasting. This approach of using IV erythromycin instead of canceling the procedure was deemed necessary because of the relative urgency of the procedure.
3. RESULTS
Table 1 summarizes the characteristics, including list of co-morbid conditions and medications, of 15 patients included in this study. The mean age of 15 patients (7 female) was 59.3 ± 16.2 years. The dose of intravenous erythromycin used was 250 - 500 mg. The mean time from the end of erythromycin infusion and repeat endoscopy was 58.7 ± 22.1 minutes (range 30 - 120 minutes). During repeat endoscopy, complete emptying of the gastric contents was noted in 10 patients (Figure 1), three patients had partial emptying (less than 30% of gastric contents remaining) and in two patients, the amount of residual contents was largely unchanged from prior examination. No anesthesia or procedure related complication occurred in these patients.
The co-morbid medical conditions or medications that are known to significantly delay gastric emptying, which were found in our study patients are marked in italics in Table 1. All but one patient in our study who had retained food in the stomach at the time of endoscopy had one or more of these predisposing factors. The most common predisposing medical conditions were diabetes mellitus (n = 7), hypothyroidism (n = 3) and parkinsonism (n = 1). The medications with significant effects on gastric emptying included narcotic analgesics (propoxyphene, oxycodone, hydrocodone), antidepressants (amytriptyline, fluoxetine, duloxetine, gabapentin, vanlafaxine) and calcium channel blockers (diltiazem). Three patients with partial emptying after IV erythromycin had multiple medications and medical conditions associated with delayed gastric emptying. The two patients in whom erythromycin completely failed to empty the stomach contents were subsequently found to have a high-grade gastric outlet obstruction; one patient had duodenal compression by pancreatic cancer and the other patient had a large pancreatic pseudocyst pressing and deforming the gastric antrum and pylorus. The presence of high grade mechanical obstruction in these patients was found only at the time of repeat endoscopy performed later.
4. DISCUSSION
Erythromycin is a motilin-receptor agonist,with strong gastric prokinetic properties and is used in patients with gastroparesis to relieve symptoms [6], to facilitate early nutritional intake in critically injured trauma victims [7] and improves endoscopic visualization in patients with acute upper gastrointestinal bleeding [8,9]. Erythromycin is also recommended to empty the stomach prior to anesthesia in certain high risk patients, though there is limited supporting data. When administered three hours prior to anesthesia in unselected patients without an increased risk for PPA, erythromycin decreased the volume of gastric contents and their acidity [10]. In one pediatric patient, parenteral erythromycin was used successfully to facilitate gastric emptying prior to emergency anesthesia [11].
Using radionucleide scintigraphy, intravenous erythromycin was found to dramatically accelerate emptying of both solids and liquids with 50% and 100% gastric emptying observed at 10 minutes and 60 minutes in healthy volunteers and at 20 minutes and 150 minutes in diabetics with gastroparesis [6]. In our cohort of patients with retained food despite adequate pre-operative fasting, we observed complete gastric emptying within 30 - 120 minutes after erythromycin infusion in ten patients. In three patients, the gastric emptying was partial (about 70%) at repeat endoscopy. It is possible that these three patients would have emptied the remaining food had we waited longer before the repeat endoscopy. Unfortunately, that cannot be determined from our data. The patients with partial emptying had multiple medical conditions or medications which slow gastric emptying potentially making these patients much more resistant to erythromycin.
Erythromycin is well tolerated, with minimal risk of allergic reactions and does not have significant interacttions with most anesthetic agents. It did not cause any problems in the two patients with high grade mechanical obstruction with large amount of retained food. We encountered no complications related to erythromycin, anesthesia, or aspiration pneumonia in our cohort. Therefore, a trial of IV erythromycin with a cautiously performed endoscopy under light sedation may be reasonable in patients who are found to have retained food in the stomach during urgent or emergent UGIE procedures.
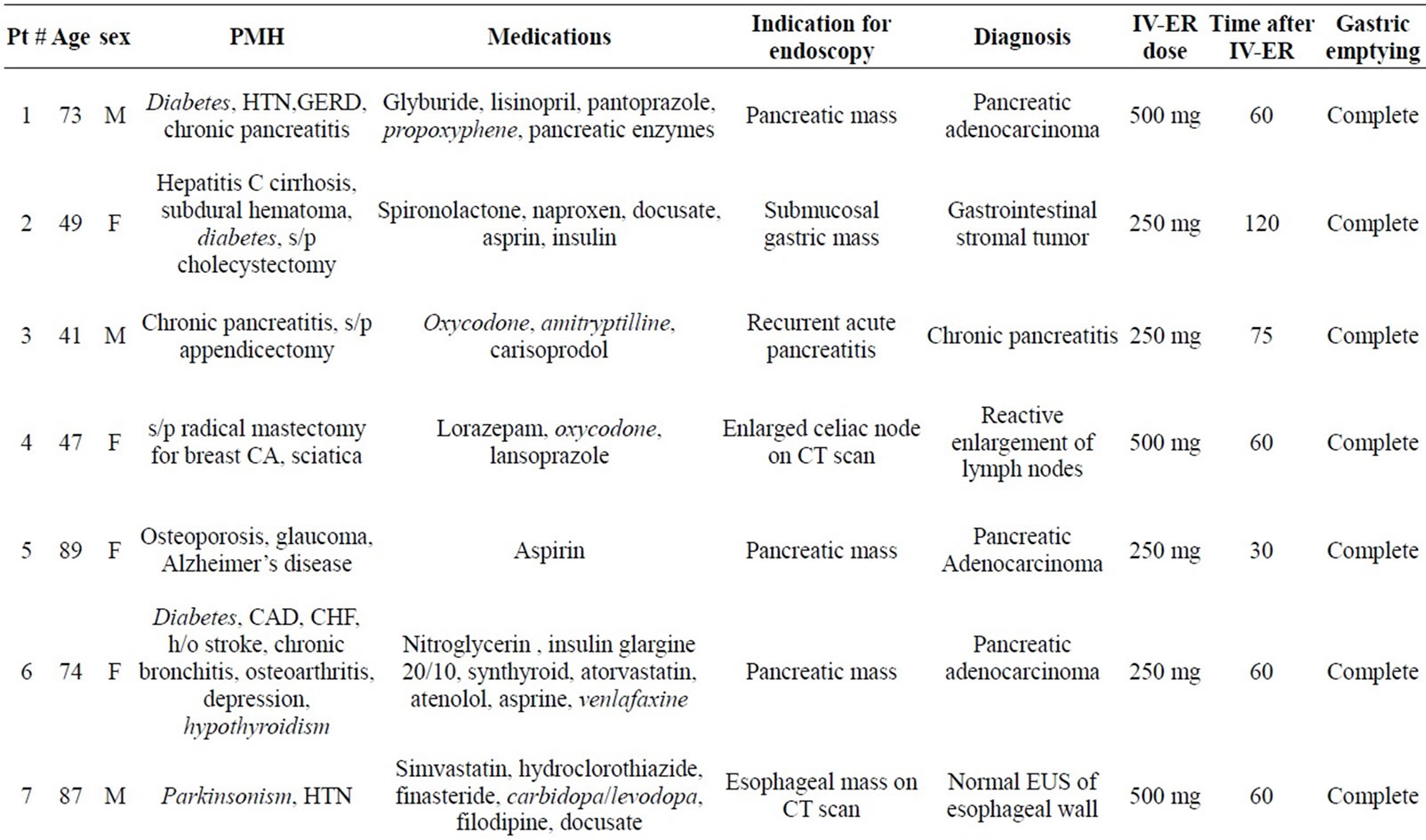
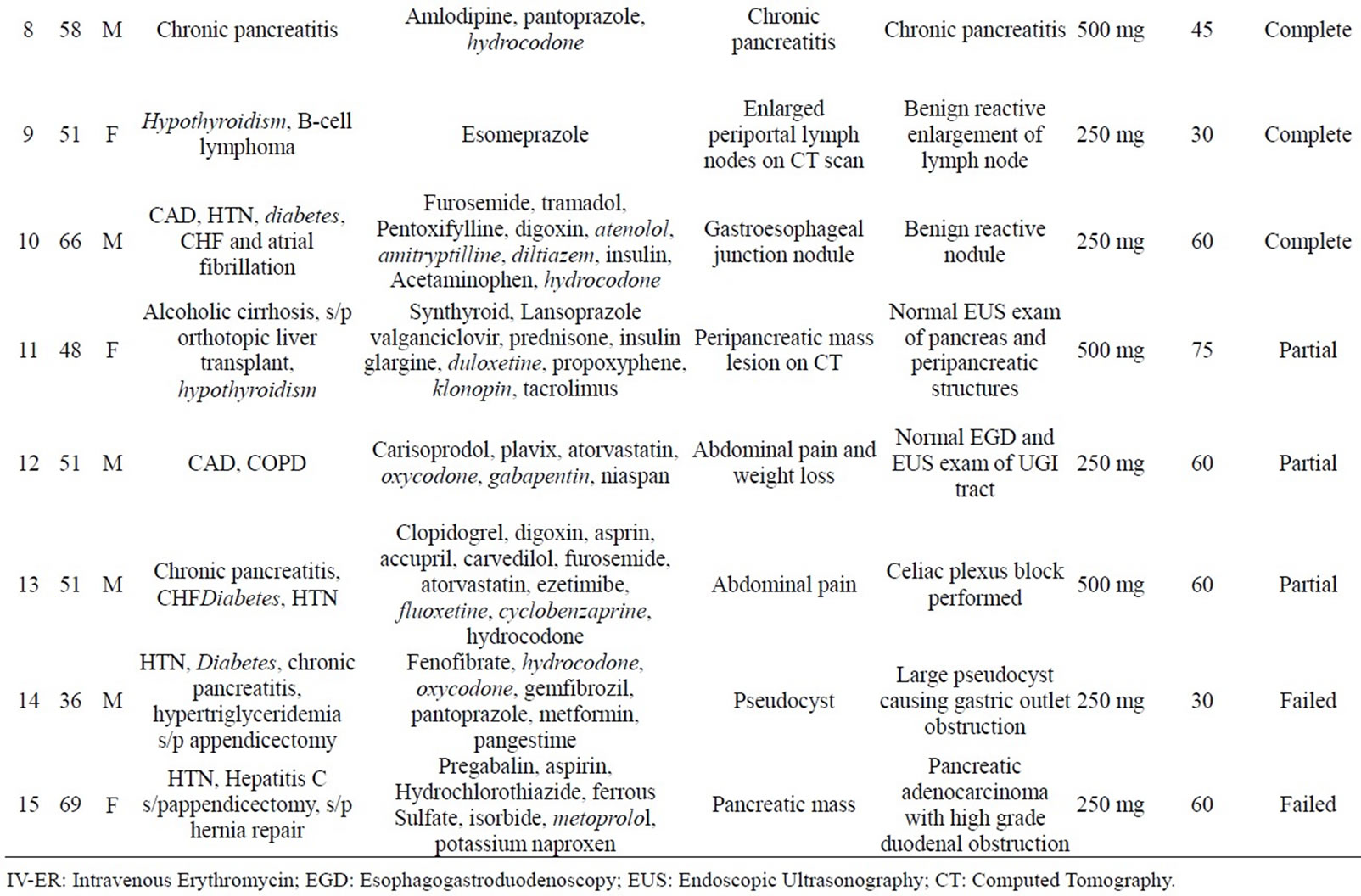
Table 1. The demographics, list of co-morbid conditions, medications, diagnosis, IV erythromycin dose and outcome of the 15 patients included in this case series. Co-morbid conditions and medications known to be associated with delayed gastric emptying are marked in italics.
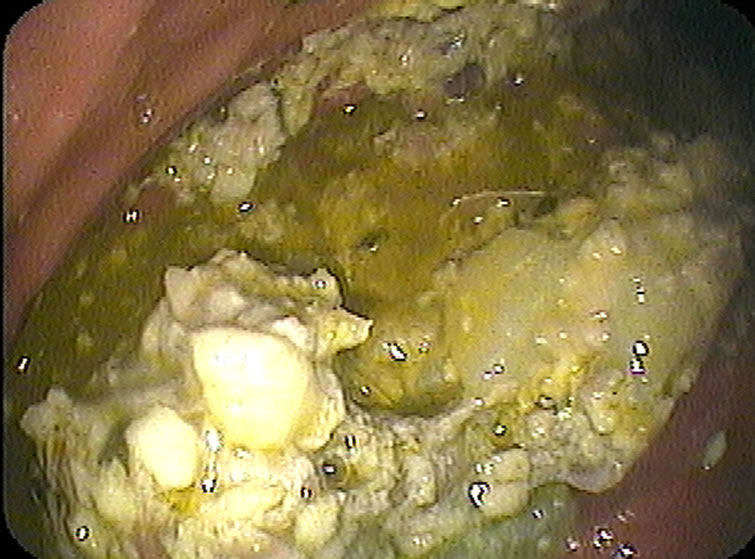
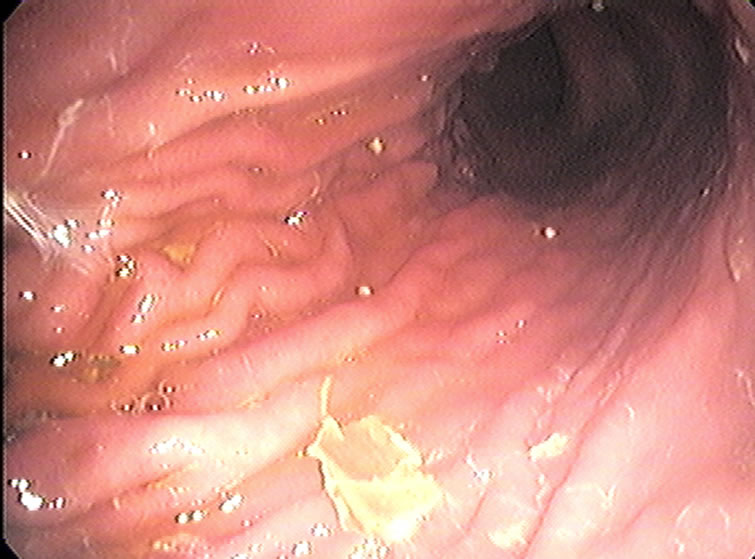
(a) Pre Erythromycin (b) Post Erythromycin
Figure 1. Endoscopic appearance of the stomach in a patient with retained food before (a) and after (b) IV erythromycin was administered.
This study is limited by its retrospective design and lack of a control arm. However, a prospective study or a study with a control arm, are not practical in this clinical scenario. Another potential criticism is that the emptying of the gastric contents could just be a function of time and was not related to erythromycin. Due to lack of a control arm it is impossible to definitively exclude that possibility in our patients. However, most of the study patients had fasted more than 12 hours prior to procedure (even though 6 hours was recommended) and had multiple factors that are known to delay gastric emptying. It is possible but rather unlikely that they would empty their gastric contents spontaneously without the prokinetic effects of erythromycin in another 30 - 120 minutes after having failed to do so in >12 hours of pre-procedure fasting. The study has several strengths, the most important being the evaluation of the amount of retained gastric contents directly by endoscopy. Secondly, it provides direct evidence of efficacy and the rapidity of gastric emptying in this subset of patient in whom gastric emptying is so impaired that they are unable to empty their stomach despite adequate pre-procedure fasting. Lastly, it provides preliminary evidence showing that with use of erythromycin, retained gastric contents noted during UGIE procedures can be emptied within a reasonable time in a significant number of patients to allow for a repeat attempt at completion of the procedure on the same day.
In conclusion, in our retrospective case series of patients undergoing elective UGIE procedures, who were found to have a significant amount of residual food in the stomach during endoscopy, single dose of 250 - 500 mg IV erythromycin promoted emptying of the retained gastric contents rapidly except in patients with high grade mechanical obstruction. Trial of IV erythromycin may be worth a consideration for emptying retained gastric contents in patients undergoing UGIE procedures in an effort to avoid cancellation and be able to safely complete the procedure on the same day in selected patients.
REFERENCES
- Warner, M.A., Warner, M.E. and Weber, J.G. (1993) Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology, 78, 56-62. doi:10.1097/00000542-199301000-00010
- American Society of Anesthesiologists Task Force on Preoperative Fasting (1999) Practice guidelines for preoperative fasting and the use of pharmacologic agentsto reduce the risk of pulmonary aspiration: Application of healthy patients undergoing elective procedures. Anesthesiology, 90, 896-905. doi:10.1097/00000542-199903000-00034
- Hawkyard, C.V. and Koerner, R.J. (2007) The use of erythromycin as a gastrointestinal prokinetic agent in adult critical care: Benefits versus risks. Journal of Antimicrobial Chemotherapy, 59, 347-358. doi:10.1093/jac/dkl537
- Petring, O.U. and Blake, D.W. (1993) Gastric emptying in adults: An over-view related to anesthesia. Anaesthesia and Intensive Care, 21, 774-781.
- Soreide, E., Eriksson, L.I., Hirlekar, G., et al., Task Force on Scandinavian Pre-Operative Fasting Guidelines, Clinical Practice Committee Scandinavian Society of Anaesthesiology and Intensive Care Medicine (2005) Preoperative fasting guidelines: An update. Acta Anaesthesiologica Scandinavica, 49, 1041-1047. doi:10.1111/j.1399-6576.2005.00781.x
- Urbain, J.L., Vantrappen, G., Janssens, J., et al. (1990) Intravenous erythromycin dramatically accelerates gastric emptying in gastroparesis diabeticum and normals and abolishes the emptying discrimination between solids and liquids. Journal of Nuclear Medicine, 31, 1490-1493.
- Berne, J.D., Norwood, S.H., McAuley, C.E., et al. (2002) Erythromycin reduces delayed gastric emptying in critically ill trauma patients: A randomized, controlled trial. Archives of Surgery, 37, 696-701.
- Frossard, J.L., Spahr, L., Queneau, P.E., Giostra, E., Burckhardt, B., Ory, G., De Saussure, P., Armenian, B., De Peyer, R. and Hadengue, A. (2002) Erythromycin intravenous bolus infusion in acute upper gastrointestinal bleeding: A randomized, controlled, double-blind trial. Gastroenterology, 123, 17-23. doi:10.1053/gast.2002.34230
- Carbonell, N., Pauwels, A., Serfaty, L., Boelle, P.Y., Becquemont, L. and Poupon, R. (2006) Erythromycin infusion prior to endoscopy for acute upper gastrointestinal bleeding: A randomized, controlled, double-blind trial. The American Journal of Gastroenterology, 101, 1211-1215. doi:10.1111/j.1572-0241.2006.00582.x
- Asai, T., Murao, K. and Shingu, K. (2000) Pre-operative oral erythromycin reduces residual gastric volume and acidity. British Journal of Anaesthesia, 85, 861-864. doi:10.1093/bja/85.6.861
- Kopp, V.J., Mayer, D.C. and Shaheen, N.J. (1997) Intravenous erythromycin promotes gastric emptying prior to emergency anesthesia. Anesthesiology, 87, 703-705.
NOTES
*There was no funding support for this manuscript. None of the authors have any potential conflict of interest relevant to this manuscript.
#Corresponding author.