O. BABUCCU ET AL.
Copyright © 2011 SciRes. SS
208
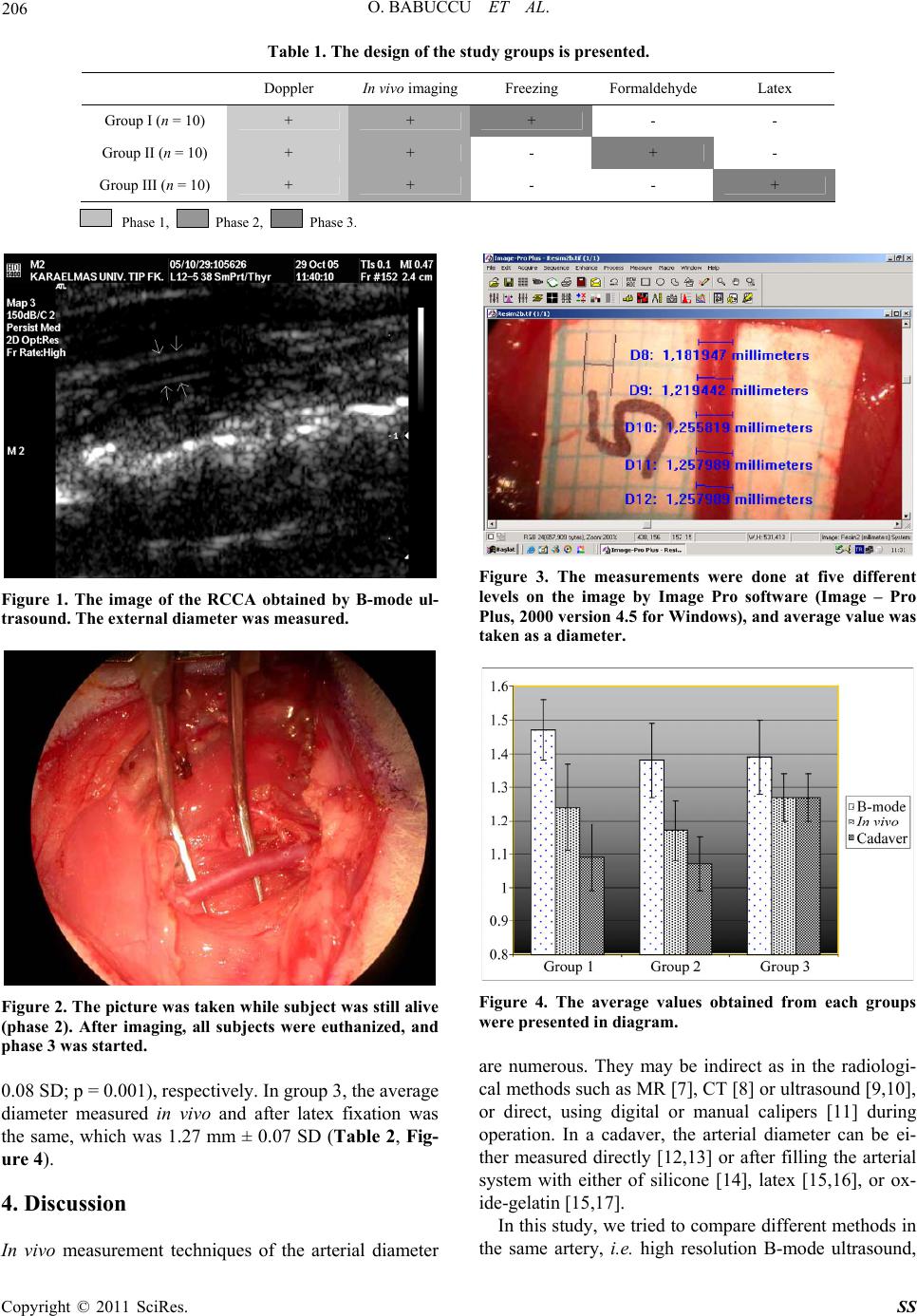
direct in vivo measurement, and cadaver study of the
right common carotid artery of the same rat. Among
three different methods applied to the same artery, the
widest diameter was found in high resolution B-mode
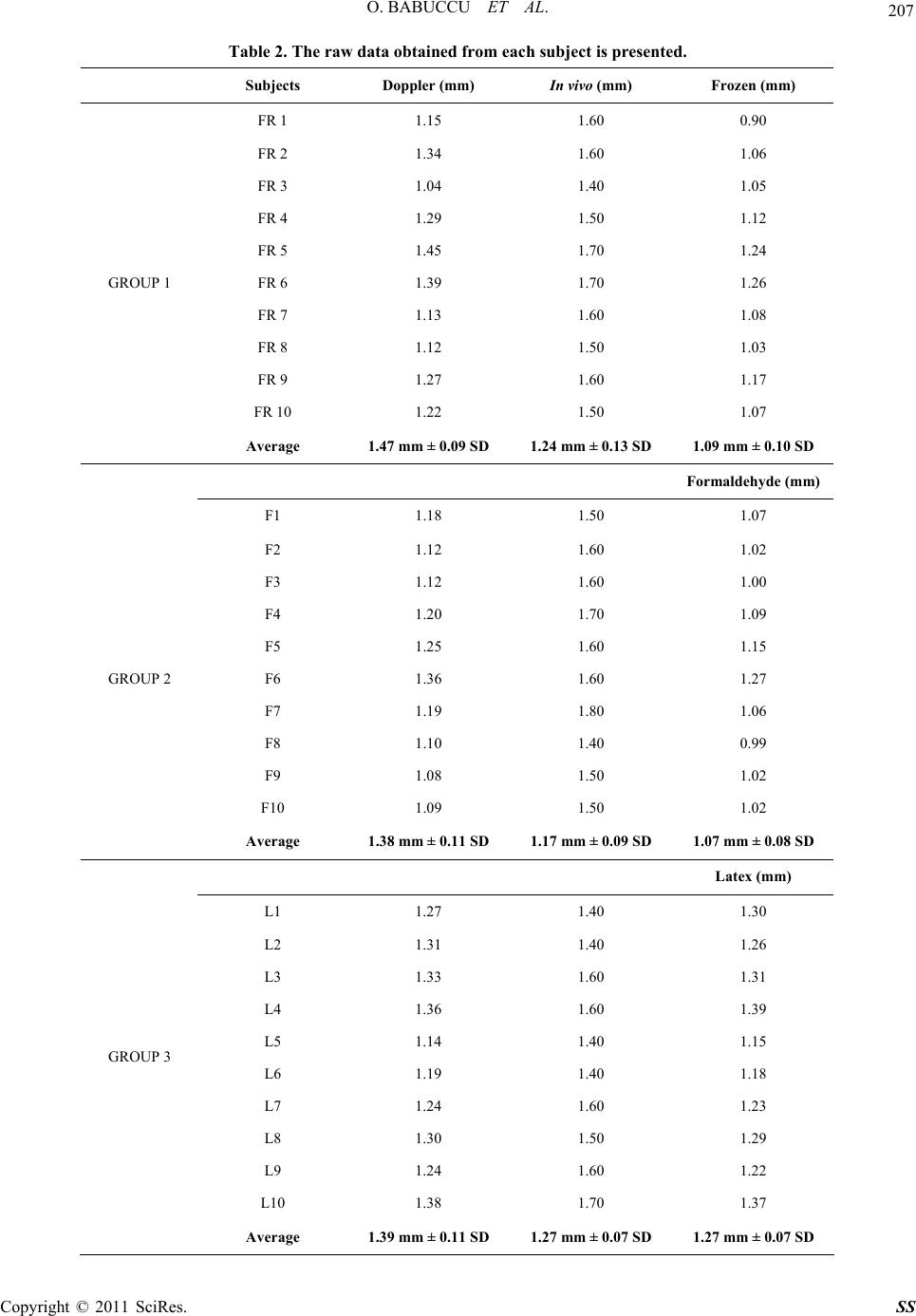
ultrasound examination in all groups (Table 2, Figure 4).
It was probably actual diameter of the given artery in
living subject. In group 1 and 2, the values obtained dur-
ing phase 2 (in vivo measurement) were significantly
grater than those obtained from frozen and formalin
fixed cadavers. In contrast, the average diameter directly
measured on living subject and that measured on latex
filled artery within the same subject were equal. In fact,
this is not unexpected, since latex can sup port vessel wall
as blood pressure does.
5. Conclusions
1) Unless filled immediately with latex or silicon, vascu-
lar diameter values measured in cadaver will be lesser
than in vivo values.
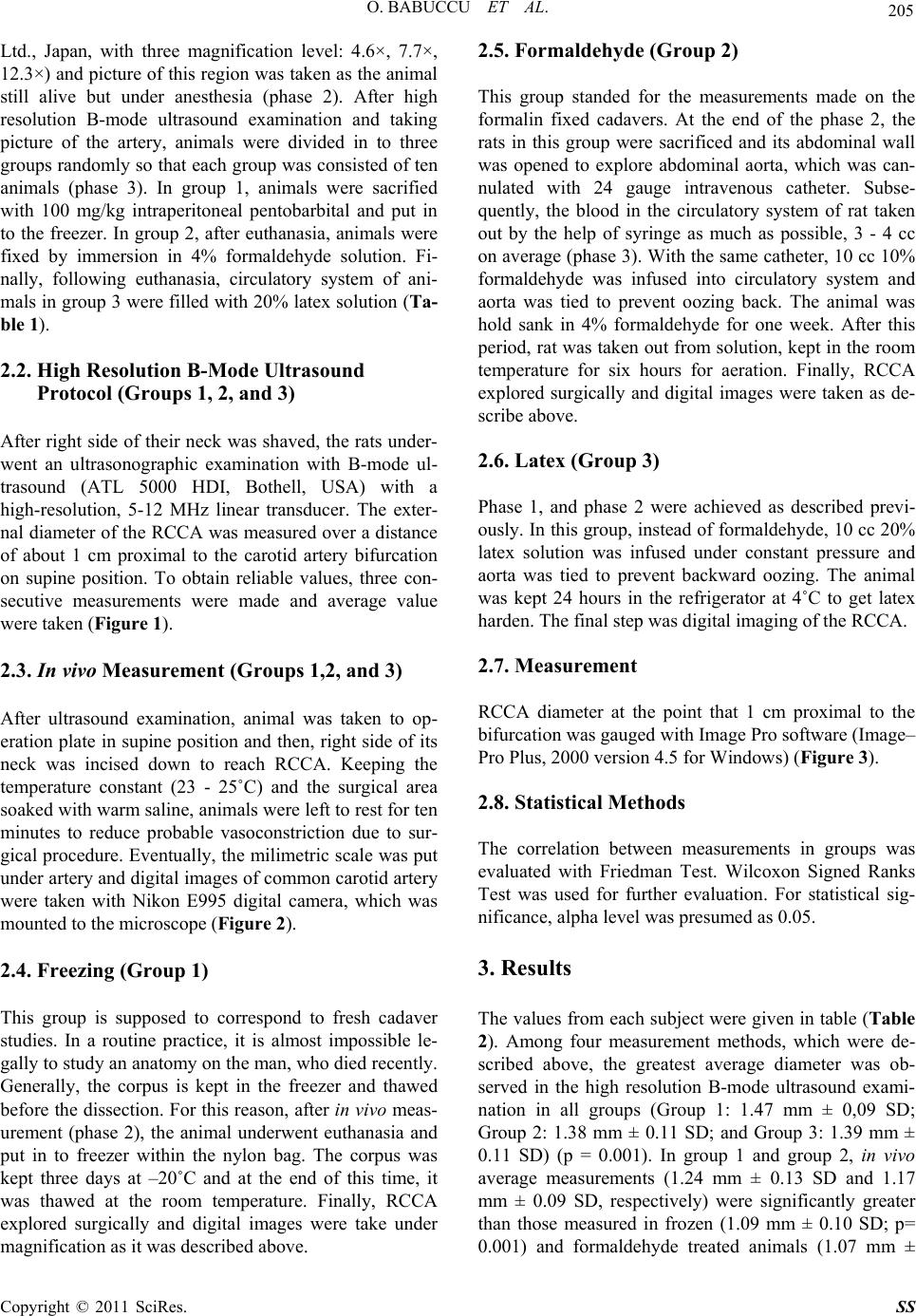
2) In living person, high resolution B-mode ultrasound
is practical way to measure arterial diameter. On the
other hand, the results probably will always be greater
than those written classical textbooks.
6. References
[1] B. Strauch and H. L. Yu, “Atlas of Microvascular Sur-
gery: Anatomy and Operative Approaches,” Thieme
Medical publishers, Inc., New York, 1993.
[2] S. J. Mathes and F. Nahai, “Reconstructive Surgery : Prin-
ciples, Anatomy and Technique,” Churchill Livingstone,
Edinburgh, 1997.
[3] D. Serafin, “Atlas of Microsurgical Composite Tissue
Transplantation,” Saunders Company, Philadelphia, 1996.
[4] O. Babuccu, H. Ozdemir, M. Hosnuter, E. Kargi, A.
Sogut and F. N. Ayoglu, “Cross-Sectional Internal Di-
ameters of Radial, Thoracodorsal, and Dorsalis Pedis Ar-
teries in Children: Relationship to Subject Sex, Age, and
Body Size,” Journal of Reconstructive Microsurgery, Vol.
22, No. 1, 2006, pp. 49-52. doi:10.1055/s-2006-931907
[5] I. H. Peterson, R. E. Jensen, J. Parnell, “Mechanical Prop-
erties of Arteries In vivo,” Circulation Research, Vol. 8,
1960, pp. 622-639.
[6] A. Munk, K. Darge, M. Wiesel, J. Troeger, “Diameter of
the infrarenal aorta and the iliac arteries in children: ul-
trasound measurements,” Transplantation, Vol. 73, No. 4,
2002, pp. 631-635.
doi:10.1097/00007890-200202270-00028
[7] H. C. Assen, A. de Roos, J. Vanderschoot and J. H.
Reiber, “Vessel Diameter Measurements in Gadolinium
Contrast-Enhanced Three-Dimensional Mra of Peripheral
Arteries,” Magnetic Resonance Imaging, Vol. 18, No. 1,
2000, pp. 13-22. doi:10.1016/S0730-725X(99)00099-5
[8] S. Suzuki, S. Furui, T. Kaminaga and T. Yamauchi,
“Measurement of Vascular Diameter In vitro by Auto-
mated Software for Ct Angiography: Effects of Inner
Diameter, Density of Contrast Medium, and Convolution
Kernel,” American Journal of Roentgenol, Vol. 182, No.
5, 2004, pp.1313-1317.
[9] R. W. Stadler, W. C. Karl and R. S. Lees, “New Methods
for Arterial Diameter Measurement from B-Mode Im-
ages,” Ultrasound in Medicine and Biology, Vol.22, No.1,
1996, pp. 25-34. doi:10.1016/0301-5629(95)02017-9
[10] V. R. Newey, D. K. Nassiri, “Online Artery Diameter
Measurement in Ultrasound Images using Artificial Neu-
ral Networks,” Ultrasound in Medicine and Biology, Vol.
28, No. 2, 2002, pp. 209-216.
doi:10.1016/S0301-5629(01)00505-1
[11] A. Uehata, T. Matsuguchi, J. A. Bittl, et al, “Accuracy of
Electronic Digital Calipers Compared with Quantitative
Angiography in Measuring Coronary Arterial Diameter,”
Circulation, Vol. 88, No.4 Pt 1, 1993, pp.1724-1729.
[12] G. D. Rosson, L. H. Holton, R. P. Silverman, N. K. Singh,
M. Y. Nahabedian, “Internal Mammary Perforators: A
Cadaver Study,” Journal of Reconstructive Microsurgery,
Vol. 21, No. 4, 2005, pp. 239-242.
doi:10.1055/s-2005-871750
[13] I. K. Lukic, V. Gluncic, A. Marusic, “Extracranial
Braches of the Middle Meningeal Artery,” Clinical
anatomy, Vol. 14, No. 4, 2001, pp. 292-294.
doi:10.1002/ca.1051
[14] O. Magden, M. Edizer, A. Atabey, V. Tayfur, I. Ergur,
“Cadaveric Study of the Arterial Anatomy of the Upper
Lip,” Plastic and Reconstructive Surgery, Vol. 114, No. 7,
2004, pp. 355-359.
doi:10.1097/01.PRS.0000131876.45116.77
[15] K. Hwang, W. J. Lee, C. Y. Jung, I. H. Chung, “Cutane-
ous Perforators of the Upper Arm and Clinical Applica-
tions,” Journal of Reconstructive Microsurgery, Vol. 21,
No. 7, 2005, pp.463-469. doi:10.1055/s-2005-918901
[16] K. Z. Tao, E. Y. Chen, R. M. Ji and R. S. Dang, “Ana-
tomical Study on Arteries of Fasciae in the Forearm Fas-
ciocutaneous Flap,” Clinical Anatomy, Vol. 13, No. 1,
2000, pp.1-5.
doi:10.1002/(SICI)1098-2353(2000)13:1<1::AID-CA1>3
.0.CO;2-6
[17] B. P. Thomas, C. R. Geddes, M. Tang, J. Williams and S.
F. Morris, “The Vascular Basis of the Thoracodorsal Ar-
tery Perforator Flap,” Plastic and Reconstructive Surgery,
Vol. 116, No. 3, 2000, pp. 818-822.
doi:10.1097/01.prs.0000176253.42394.7c