N. Miyatake et al. / Health 3 (2011) 394-399
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
398
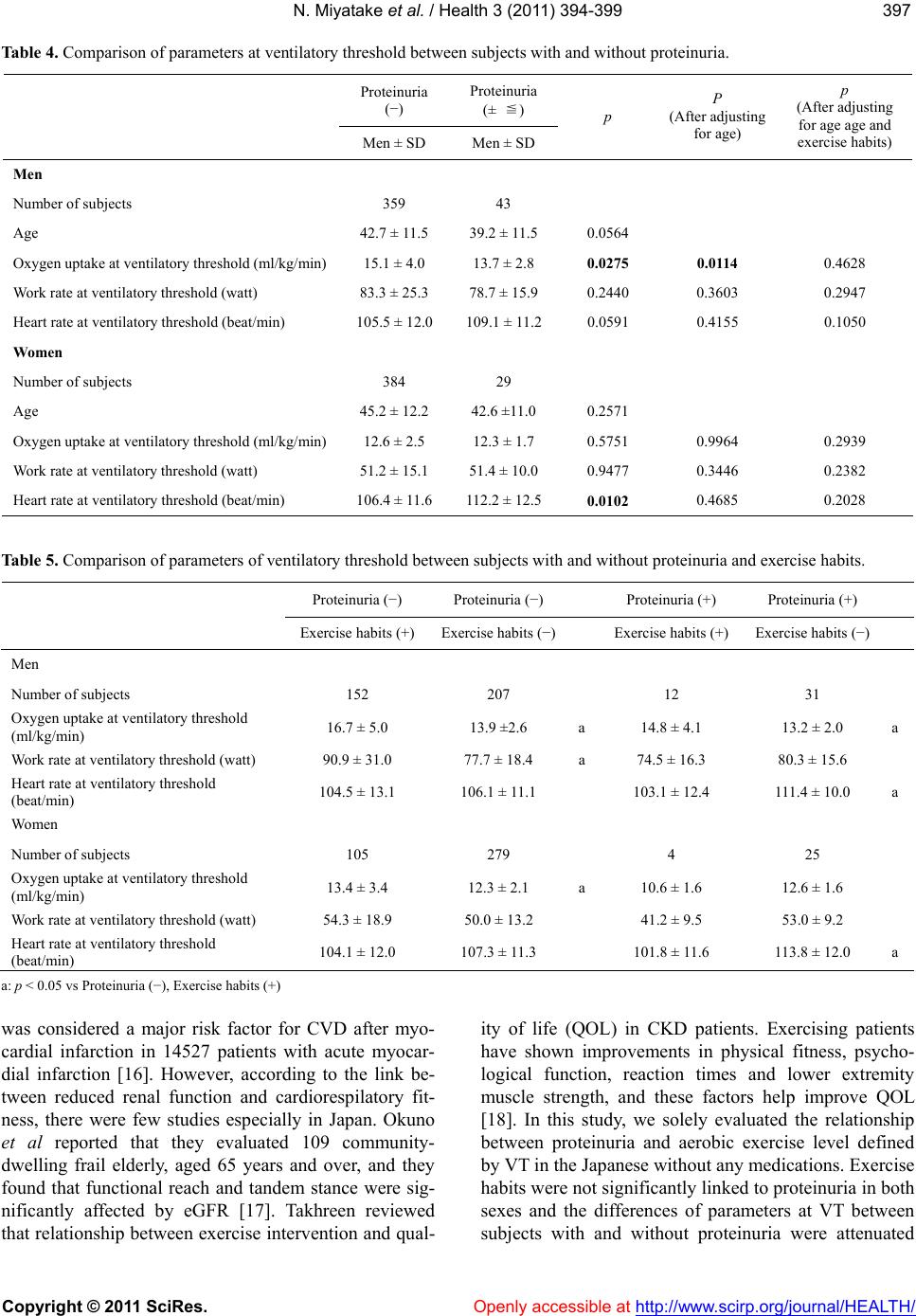
after adjusting for age and exercise habits in men. How-
ever, oxygen uptake at VT in women with proteinuria
was not significantly lower than that in women without.
In addition, we compared oxygen uptake at VT among
subjects with and without proteinuria and exercise habits,
and found that oxygen uptake at VT in Group D was the
lowest among 4 groups in men. Oxygen uptake at VT in
Group A was the highest among 4 groups in both sexes.
Taken together, promoting exercise habits might be con-
sidered for improving aerobic exercise level, and pro-
teinuria might be a modifiable factor of VT, especially in
Japanese men.
Potential limitations still remain in this study. First,
our study was a cross sectional and not a longitudinal
study. Second, 402 men and 413 women in our study
voluntarily underwent measurements: they were there-
fore more likely to be health-conscious compared with
the average person. Third, we could not show clear
mechanism between proteinuria and oxygen uptake at
VT. We have previously reported that brachial-ankle
pulse wave velocity (baPWV) in subjects with reduced
eGFR was significantly higher than that in subjects
without [19]. Arterial stiffness might affect the results. In
addition, low prevalence of proteinuria also affected the
results, especially in women. To show this, further pro-
spective studies are needed in the Japanese.
5. ACKNOWLEDGEMENTS
This research was supported in part by Research Grants from the
Ministry of Health, Labor, and Welfare, Japan. There are no conflicts
of interest.
REFERENCES
[1] National Kidney Foundation. (2002) K/DOQI clinical
practice guidelines for chronic kidney disease: evaluation,
classification, and stratification. American Journal of
Kidney Diseases, 39, S1-S266.
[2] Foley, R.N., Parfrey, P.S. and Sarnak, M.J. (1998) Clini-
cal epidemiology of cardiovascular disease in choronic
renal disease. American Journal of Kidney Diseases, 32,
S112-S119.
doi:10.1053/ajkd.1998.v32.pm9820470
[3] Imai, E., Horio, M., Iseki, K., Yamagata, K., Watanabe,
T., Hara, S., Ura, N., Kiyohara, Y., Hirakata, H., Mori-
yama, T., Ando, Y., Nitta, K., Inaguma, D., Narita, I., Iso,
H., Wakai, K., Yasuda, Y., Tsukamoto, Y., Ito, S., Makino,
H., Hishida, A. and Matsuo, S. (2007) Prevalence of
chronic kidney disease (CKD) in the Japanese general
population predicted by the MDRD equation modified by
a Japanese coefficient. Clinical and Experimental Ne-
phrology, 11 , 156-163.
doi:10.1007/s10157-007-0463-x
[4] Matsuo, S., Imai, E., Horio, M., Yasuda, Y., Tomita, K.,
Nitta, K., Yamagata, K., Tomino, Y., Yokoyama, H. and
Hishida, A. (2009) Revised equations for estimated GFR
from serum creatinine in Japan. American Journal of
Kidney Diseases, 53, 982-992.
doi:10.1053/j.ajkd.2008.12.034
[5] Miyatake, N., Shikata, K., Makino, H. and Numata, T.
(2010) Relationship between estimated glomerular fila-
tration rate (eGFR) and metabolic syndrome in the Japa-
nese population. Acta Medica Okayama, 64, 203-208.
[6] Miyatake, N., Shikata, K., Makino, H. and Numata, T.
(2011) The relation between estimated glomerular filtra-
tion rate (eGFR) and proteinuria in okayama prefecture,
Japan. Environmental Health and Preventive Medicine,
16, 191-195.
doi:10.1007/s12199-010-0183-9
[7] Wasserman, K., Whipp, B.J., Koyl, S.N. and Beaver, W.L.
(1973) Anaerobic threshold and respiratory gas exchange
during exercise. Journal of Applied Physiology, 35,
236-243.
[8] Weber, K.T. and Janicki, J.S. (1985) Cardiopulmonary
exercise testing for evaluation of chronic cardiac failure.
American Journal of Cardiology, 55, 22-31.
doi:10.1016/0002-9149(85)90792-1
[9] (2005) Definition and the diagnostic standard for meta-
bolic syndrome—Committee to Evaluate Diagnostic
Standards for Metabolic Syndrome. Nippon Naika Gak-
kai Zasshi, 94, 794-809 (in Japanese).
[10] Jones, N.L., Makrides, L., Hitchcock, C., Chypchar, T.
and McCartney, N. (1985) Normal standards for an in-
cremental progressive cycle ergometer test. American
Review of Respiratory Disease, 131, 700-708.
[11] Davis, J.A., Frank, M.H., Whipp, B.J. and Wasserman, K.
(1979) Anaerobic threshold alterations caused by endur-
ance training in middle-aged men. Journal of Applied
Physiology, 46, 1039-1046.
[12] Beaver, W.L., Wasserman, K. and Whipp, B.J. (1986) A
new method for detecting anaerobic threshold by gas
exchange. Journal of Applied Physiology, 60, 2020-2027.
[13] Wallace, J.F., Pugia, M.J., Lott, J.A., Luke, K.E., Shihabi,
Z.K., Sheehan, M. and Bucksa, J.M. (2001) Multisite
evaluation of a new dipstick for albumin, protein and
creatinine. Journal of Clinical Laboratory Analysis, 15,
231-235.
doi:10.1002/jcla.1032
[14] Miyatake, N., Miyachi, M., Tabata, I., Sakano, N., Suzue,
T., Hirao, T. and Numata, T. (2010) Evaluation of venti-
latory threshold and its relation to exercise habits among
Japanese. Environmental Health and Preventive Medi-
cine, 15, 374-380.
doi:10.1007/s12199-010-0147-0
[15] Irie, F., Iso, H., Sairenchi, T., Fukasawa, N., Yamagishi,
K., Ikehara, S., Kanasahiki, M., Saito, Y., Ota, H. and
Nose, T. (2006) The relationships of proteinuria, serum
creatinine, glomerular filtration rate with cardiovascular
disease mortality in Japanese general population. Kidney
International, 69, 1264-1271.
doi:10.1038/sj.ki.5000284
[16] Anavekar, N.S., McMurray, J.J., Velazquez, E.J., Solo-
mon, S.D., Kober, L., Rouleau, J.L., White, H.D., Nord-
lander, R., Maggioni, A., Dickstein, K., Zelenkofske, S.,
Leimberger, J.D., Califf, R.M. and Pfeffer, M.A. (2004)
Relation between renal dysfunction and cardiovascular
outcomes after myocardial infarction. The New England