J. Bircher et al. / Health 3 (2011) 378-382
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
381381
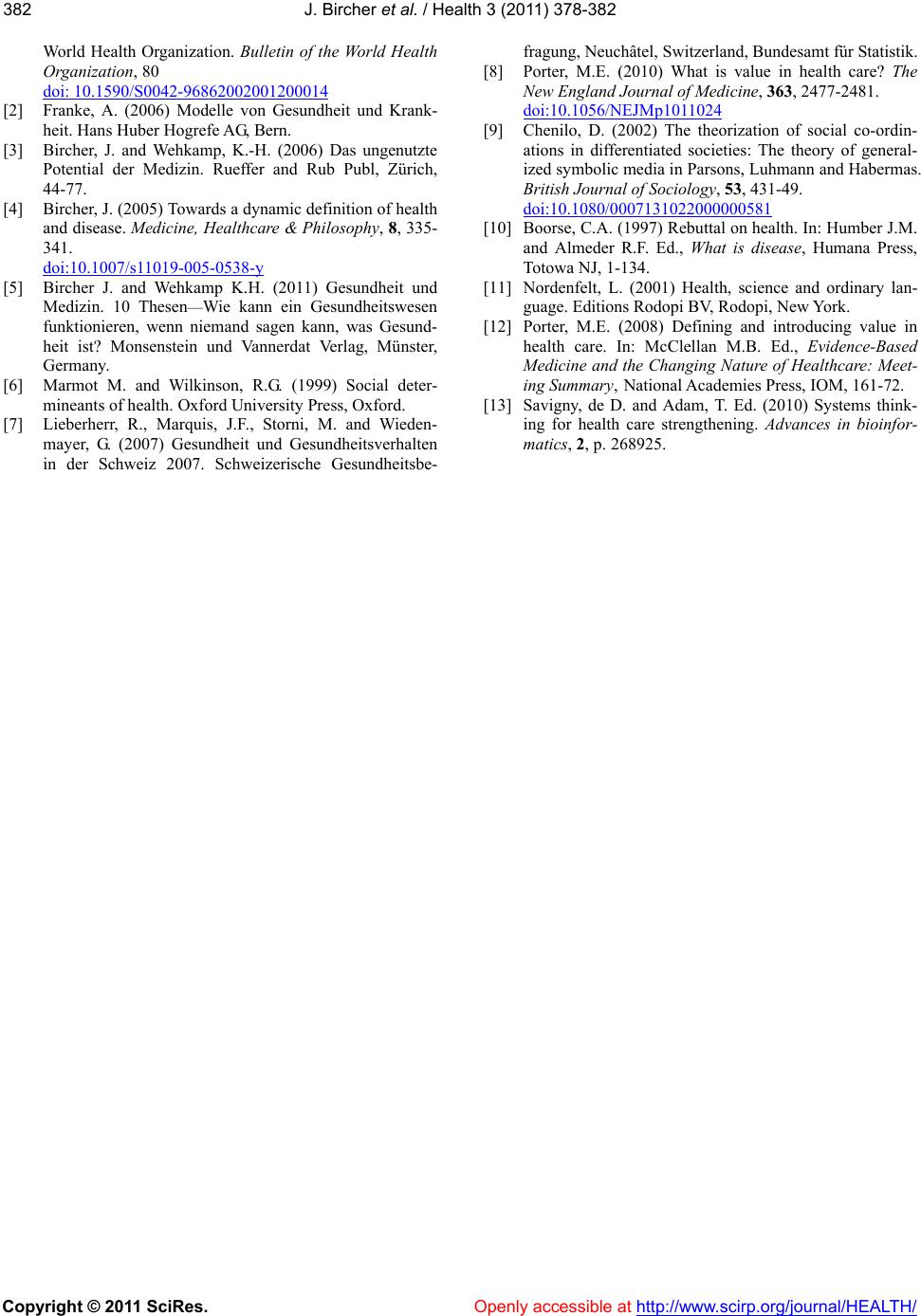
features of a system. Each of them responds to demands
that induce actions. Whether or not this action occurs is
governed in each specific case by a generalized symbolic
medium of communication. For instance, in an economy,
people demand goods and services. Whether these are
purchased or not depends on money. Only if the price is
adequate for the goods or services, are they bought. In
the legal system there may be a demand for justice,
which can be responded to by an agreement or by a court
order. Both cases must conform to the law in order to be
valid. Therefore, in the legal system, the laws play the
role of the generalized symbolic medium of communica-
tion. In science there is a demand for new knowledge.
For both, the financing of projects and for their publica-
tion in scientific journals peer review is required. These
examples may illustrate two features of a generalized
symbolic medium of communication: It plays a central
role for the processes that occur within the system and
its nature is specific for each system. In medicine and
health care by necessity the concept of health and dis-
ease serves as symbolic medium of communication.
Consequently, it is pivotal for the health care system not
to leave health and disease within the realm of arbitrary
individual judgments, but to define them in such a way
that everyone can agree about them. If in health care
money would serve as generalized symbolic medium of
communication, medicine would become part of the
economy and lose its specific nature.
4. WHY CHOOSE THE MEIKIRCH
MODEL?
When opting for a definition of health, it is important
to compare it with the best possible alternatives. For lack
of space only two eminent examples are discussed here:
1) Christopher Boorse [10] proposed a biostatistical
value-free definition. He explains “health as the absence
of disease” and “disease as a type of internal state, which
is either an impairment of normal functional ability, i.e. a
reduction of one or more functional abilities below typi-
cal efficiency, or a limitation of functional ability caused
by environmental agents”. Normal functional ability is
defined by statistical comparison with an age and sex
specific reference group. The value of this definition of
health and disease consists in the fact that it is based on
measurements and statistics. It has been criticized, how-
ever, on the basis that the selection of a reference group
is not truly value-free, but requires a normative judg-
ment. In addition the definition does not structure the
health problem of p atients. If a statistical significance of
p < 0.05 is chosen, 5% of normal subjects are diseased.
In addition, to define health, it is needed to measure the
appropriate parameter. In practice this is difficult.
2) Lennart Nordenfelt [11] proposes a welfare theory
of health. He considers health to be the primary concept
in the web of medical thinking. He states: “A is com-
pletely healthy if, and on ly if, A is in a bodily and mental
state which is such that A has an ability to realize all his
or her vital goals, given accepted circumstances.” This
ingenious definition is normative and derived from the
action theory. For the purpose of medicine and health
care, though, the terms he uses are difficult to apply in
practice. How do we assess e.g. vital goals or accepted
circumstances?
3) Several other normative definitions use among
other criteria the need or lack of need for medical care as
a decisive factor to define health or disease. This leads to
circular reasoning because disease in turn justifies by
itself the administration of medical care.
The Meikirch Model is also normative. Its practical
importance lies in the fact that all six criteria for the de-
scription of health or disease may be assessed in consul-
tations with patients. Therefore they may serve as crite-
ria to analyze value in health care, i.e. health outcome
per dollar spent [12]. In addition, it structures the com-
ponents of health in such a way, that they may be used in
research, in advising individual patients, in medico legal
expertises and in policy decisions for public health. The
Meikirch Model may also serve to explain the nature of
medicine to members of other social systems, e.g.
economists, managers, politicians, lawyers, and scien-
tists. If they understand the model, it may provide the
common denominator for joint policy decisions [13].
This is particularly pertinent, because health care con-
tinuously evolves together with the other social systems.
If, as postulated by Porter [12], the measurement of
value must be its fundamental goal an d improving value
the driving force for every participant, the Meikirch
Model could become a pivotal reference point for this
purpose.
As a next step the different stakeholders need to be
able to perceive the usefulness of the Meikirch Model
and to agree to apply it for interdisciplinary communica-
tion about health care. For this purpose it probably is
useful to start with a widespread discussion on this sub-
ject. More details may be found on a website [5]. Once
the Meikirch Model corresponds to a general under-
standing, it is expected that medicine and health care
will tangibly be more beneficial socially.
5. CONFLICT OF INTEREST
STATEMENT
There are no funds involved from any side. For both authors there
are no conflicts of interest.
REFERENCES
[1] Grad, F.P. (2002) Preamble of the constitution of the