 Journal of Environmental Protection, 2011, 2, 379-386 doi: 10.4236/jep.2011.24042 Published Online June 2011 (http://www.SciRP.org/journal/jep) Copyright © 2011 SciRes. JEP 379 Preliminary Risk Assessment Posed by Formaldehyde Residues in Clothing to Vietnamese Consumers Van Nam Thai, Akihiro Tokai Osaka University, Division of Sustainable Energy and Environmental Engineering, Osaka, Japan. Email: thai@em.see.eng.osaka-u.ac.jp, namtv78@yahoo.com Received January 19th, 2011; revised February 26th, 2011; accepted April 6th, 2011. ABSTRACT The assessment of potential health risks posed by formaldehyde in clothing to consumers is of increasing concern worldwide. Because of this, it is necessary to develop an exposure model that can realistically mimic clothes wearing conditions. This study aims to preliminarily develop a health risk assessment model for formaldehyde in clothing, and then to assess the potential health risk posed by formaldehyde in textiles to adults and infants in Vietnam using the model. Finally, this study aims to exam ine the plausibility of the adopted permissible values for fo rmaldehyde in cloth- ing in Vietnam. In the model, two exposure factors for dermal exposure and overall exposure routes, i.e. sweat type and perspiration area, were considered. The margins of exposure (MOE) were calculated to estimate the health risks from worst case and average exposures. The assessment shows that acute exposure via inhalation can pose health risks to Vietnamese consumers in both cases. In regards to chronic exposure, dermal exposure is about four (for infants) and seven (for adults) times higher than exposure via inha lation, but no risks were found for averag e exposure . If a MOE of 100 is defined as ‘safe’ used, dermal and total chronic exposure to worst case cause potential risks, whereas no health risks were found for exposure to average case. With the model, the adopted Vietnamese permissible values for forma l- dehyde in clothing were assessed as not posing a health risk to Vietnamese consumers, hence they are accepted. Keywords: Formaldehyde, Health Risk, Exposure Model, Clothing, Vietnamese Consumers 1. Introduction In 2004, the International Agency for Research on Can- cer (IARC) classified formaldehyde as a human carcino- gen [1] as well as highly toxic, and irritating. Subsequent to this classification, the first serious exposure event oc- curred in New Zealand (2007) [2 ] from Chinese imports. Many countries then carried out analytical studies of formaldehyde in clothes and set limits, e.g. the European Union (EU) (2007) [3], Australia (2007), Netherlands (2008), the US (2008) [4], and the US (2010) [5]. Thus, formaldehyde residue in clothing has become a hot issue for imported textiles. China Daily (2009) reported that 46.5% of clothing produced in Guangdong provin ce, the most indu strialized province in China, which exports clothing to Vietnam, exceeded the permissible levels of formaldehyde in tex- tiles. To control this substance in imported clothing and textiles (mainly from China, 36.6% of total imports) (Vietnam Statistics Office, 2009), the Vietnam Ministry of Industry and Trade (MOIT) issued a contemporary regulation for formaldehyde limits [6]. However, there has been no demonstrated research in terms of risk as- sessments of Vietnamese consumer’s health when using such contaminated textiles. In addition, although the adopted permissible values, based on those of the EU Flower Label and Oeko-tex 100, are appropriate to ex- port textiles, the question ‘Are they suitab le for domestic consumers?’ should be quantitatively answered in terms of scientific grounds. Therefore, it is necessary to create a model to identify any health risks to Vietnamese con- sumers and to check the plausibility of the adopted val- ues. Some recent studies on formaldehyde in clothing have focused on measuring formaldehyde in clothes (both free and extracted partly through hydrolysis), and then com- paring these measurements with standard values [2,5,7]. Others have extensively studied the human health risk assessment from dermal exposure, but there is little in- formation concerning the exposure via inhalation. In gen- 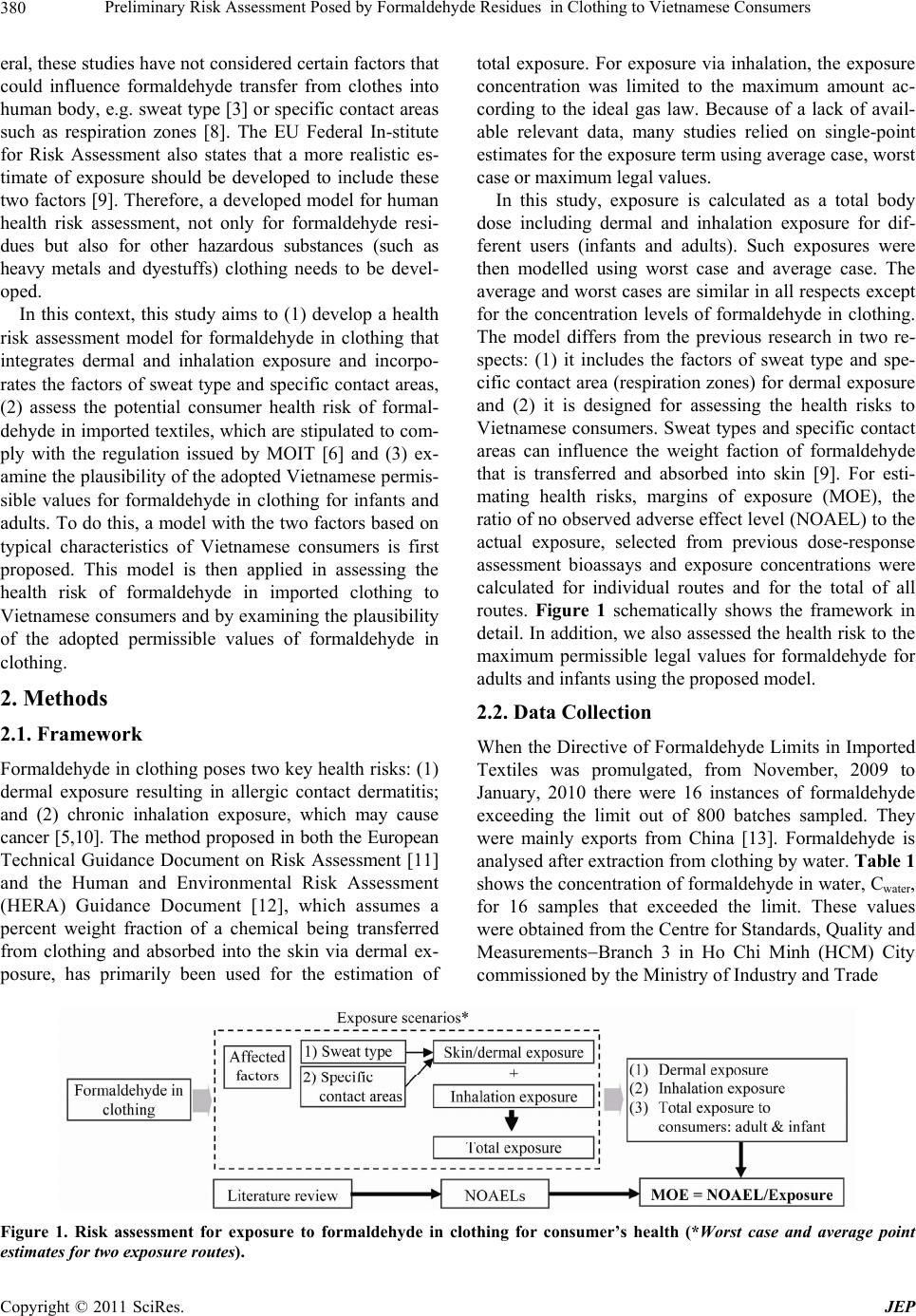 Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers 380 eral, these studies have not considered certain factors that could influence formaldehyde transfer from clothes into human body, e.g. sweat type [3] or specific contact areas such as respiration zones [8]. The EU Federal In-stitute for Risk Assessment also states that a more realistic es- timate of exposure should be developed to include these two factors [9]. Therefore, a developed model for human health risk assessment, not only for formaldehyde resi- dues but also for other hazardous substances (such as heavy metals and dyestuffs) clothing needs to be devel- oped. In this context, this study aims to (1) develop a health risk assessment model for formaldehyde in clothing that integrates dermal and inhalation exposure and incorpo- rates the factors of sweat type and specific contact areas, (2) assess the potential consumer health risk of formal- dehyde in imported tex tiles, which are stipulated to com- ply with the regulation issued by MOIT [6] and (3) ex- amine the plausibility of the ad opted Vietnamese permis- sible values for formaldehyde in clothing for infants and adults. To do this, a model with th e two factors based on typical characteristics of Vietnamese consumers is first proposed. This model is then applied in assessing the health risk of formaldehyde in imported clothing to Vietnamese consumers and by examining the p lausibility of the adopted permissible values of formaldehyde in clothing. 2. Methods 2.1. Framework Formaldehyde in clothing poses two key health risks: (1) dermal exposure resulting in allergic contact dermatitis; and (2) chronic inhalation exposure, which may cause cancer [5,10]. The method proposed in both the European Technical Guidance Document on Risk Assessment [11] and the Human and Environmental Risk Assessment (HERA) Guidance Document [12], which assumes a percent weight fraction of a chemical being transferred from clothing and absorbed into the skin via dermal ex- posure, has primarily been used for the estimation of total exposure. For exposure via inhalation, the exposure concentration was limited to the maximum amount ac- cording to the ideal gas law. Because of a lack of avail- able relevant data, many studies relied on single-point estimates for the exposure term using average case, worst case or maximum legal values. In this study, exposure is calculated as a total body dose including dermal and inhalation exposure for dif- ferent users (infants and adults). Such exposures were then modelled using worst case and average case. The average and worst cases are similar in all respects except for the concentration levels of formaldehyde in clothing. The model differs from the previous research in two re- spects: (1) it includes the factors of sweat type and spe- cific contact area (respiration zones) for dermal exposure and (2) it is designed for assessing the health risks to Vietnamese consumers. Sweat types and specific contact areas can influence the weight faction of formaldehyde that is transferred and absorbed into skin [9]. For esti- mating health risks, margins of exposure (MOE), the ratio of no observed adverse effect level (NOAEL) to the actual exposure, selected from previous dose-response assessment bioassays and exposure concentrations were calculated for individual routes and for the total of all routes. Figure 1 schematically shows the framework in detail. In addition, we also assessed the health risk to th e maximum permissible legal values for formaldehyde for adults and infants using the proposed model. 2.2. Data Collection When the Directive of Formaldehyde Limits in Imported Textiles was promulgated, from November, 2009 to January, 2010 there were 16 instances of formaldehyde exceeding the limit out of 800 batches sampled. They were mainly exports from China [13]. Formaldehyde is analysed after extraction from clothing by water. Table 1 shows the concentration of formaldehyde in water, Cwater, for 16 samples that exceeded the limit. These values were obtained from the Cen tre for Stand ard s, Qu ality an d MeasurementsBranch 3 in Ho Chi Minh (HCM) City commissioned by the Ministry of Industry and Trade Figure 1. Risk assessment for exposure to formaldehyde in clothing for consumer’s health (*Worst case and average point estimates for two exposure routes). Copyright © 2011 SciRes. JEP  Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers381 Table 1. Analytical data for formaldehyde in imported textiles (mg/kg fabrics). Nov., Dec., 2009 Jan., 2010 No Sample Value (Cwate r ) No Sample Value (Cwate r ) 1 F27 2,619 11 F623 812 2 F38 750 12 F690 1,337 3 F65 3,517 13 F699 463 4 F96 384 14 F728 784 5 F99 2,035 15 F747 359 6 F113 806 16 F791 982 7 F357 1,334 Formaldehyde limits in textiles [6] 8 F389 872 Infant (<3 year-old) 30 9 F487 397 Direct contact 75 10 F539 537 Indirect contact 300 Mean = 1,124; Max value = 3 ,517; SD = 889 with the 95% confidence interval being 474. Accordingly, formaldehyde concentration = 1,124 474 (mg/kg textile). with the support of a recommendation letter from the HCM Environmental Protection Ag ency. 2.3. Exposure Scenarios To approach the three purposes described in the intro- duction, a health risk assessment model for dermal and inhalation exposure was first devised. The calculations of the estimated exposures were performed twice: once based on the highest relevant concentrations (i.e. the worst case) and once based on average concentrations (average case) that consumers could be exposed to. Con- siderations of the individual exposure routes and their respective concentration s, i.e. skin exposur e (Expskin) and inhalation exposure (Expinhalation), led to the expression for the overall exposure (Exptotal) shown in Equation (1): totalskin inhalation ExpExp Exp (1) 2.3.1. Skin Exposure Consumers can be directly exposed to formaldehyde dermally by wearing clothing processed with it (perma- nent press fabrics or anti-wrinkle/crease fabrics). Equa- tion (2), based on the HERA Guidance Document [12], but modified to suit exposure is as follows. (The HERA Guidance Document proposed an exposure model for esterquats, fabric conditioners, that remain in clothes washed and softened with such substances, but not for- maldehyde). 12skin ExpCSFDFFNBW (2) where Expskin.:dermal (skin) systemic consumer exposure (mg/kg of bod y weig ht/ day ) C: formaldehyde concentration in clothing (mg/kg tex- tile) (also called Cwater in this paper) S: surface area of exposed skin (m2) FD: fabric density (g/m2) F1: percent weight fraction of formaldehyde trans- ferred from clothing to skin (migration ratio) (%) F2: percent weight fraction of formaldehyde absorbed by the skin (penetration ratio ) (%) N: exposure frequency (day1) BW: body weight (kg) 2.3.1.1. Parameter Estimations C (mg/kg) was assigned average and maximum values (worst case) from the measured formaldehyde concentra- tion in Table 1. The total body areas (S) for an adult an d a child were assumed to be 18,150 cm2 and 6,700 cm2, respectively [3]. The exposed area was taken to be 85% of a person’s total body area [3], g iving Sadult = 15,430 cm2 and Schild = 5,695 cm2. Cotton and cotton/polyester blended fabrics are the most predominant in Vietnam; hence, the average FD (g/m2) was assigned to be 200 g/m2 [14]. The bases for the assessment of formaldehyde ex- posure from clothing are the migration ratio (F1) and the penetration ratio (F2). The value of F2 is determined by the octanol water partition coefficient (Kow)1. Since log(Kow) of formaldehyde is 0.35 [1], formaldehyde is categorised as hydrophilic. Based on the HERA Guid- ance Document [12]2, we selected F1 as being 100% and F2 as being 5% in normal areas and 10% in high contact 1If a chemical has log (Kow) [3, 1), it is hydrophilic; [1, 4), rela- tively hydrophobic and [4, 7], very hydrophobic. 2Penetration ratios of hydrophilic textile auxiliaries are 5% and 10% or normal and respiration zones, respectively. Copyright © 2011 SciRes. JEP  Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers 382 areas (perspiration areas) [9]. It was assumed that con- sumers wear clothes for the entire day (N = 24 hours)3. The standard BW of a 3-year-old child (BWchild) was assumed to be 13.9 kg [15], while the average weight of a Vietnamese adult (BWadult) was calculated as being 56.0kg. This latter calculation used the following algo- rithm: BWadult (kg) = BMI × H2 (BMI: Body Mass Index, average BMI = 22; H: the height of a Vietnamese adult, average H = 1.59 m [16]). 2.3.1.2. Exp osure Factors Temperature (t, ˚C) and humidity were assumed to be constants with t being 25˚C. We excluded the pH of washing water owning to unavailable data and high un- certainty. Ryan et al. [17] stated that areas with high contact with specific parts of the body (specific contact areas or perspiration areas) are the most allergic to for- maldehyde. The authors studied diagnosis of allergic contact dermatitis from formaldehyde irritation and ob- served that the common eruption sites, such as around the neck, the lateral thorax, the flexor surfaces and the waistband were those highly exposed to clothing. It was concluded that these areas can influence the absorption of formaldehyde into skin. To calculate the perspiration areas we utilised into allergic contact dermatitis by Ryan et al. above and the proportions of the skin surface iden- tified by Mathieu [18]. Using these, perspiration areas were estimated to be 30% of the total exposure area. The penetration ratio in these areas was assigned the variable F2 sweat. As described previously formaldehyde is usually ex- tracted by water (refer to Cwater shown in Table 1. How- ever, according to research by the European Commission [3], it is better to mimic the real extraction conditions in which consumer sweat (either acid or basic) extracts the formaldehyde than using water. The research shows that formaldehyde concentrations after extraction by ba- sic/acid sweat solution are on average 1.3 times higher than those after extraction by a water solution. As a result, a better estimate of concentrations of formaldehyde in the F2 sweat area is Csweat = × Cwater ( = 0.8 - 2.5 with an average of 1.3, = 2.5 in the worst case [3]). Using this, Equation 2 can be written as follows: 22 1 0.7 0.3 kin watersweatsweat ExpCS FCSF FDFN BW (3) 2.3.2. Inhalation Exposure Exposure via inhalation is expressed as the concentration of formaldehyde in the air in a breathing zone and is given as an average concentration over a reference period. The vapour immediately produces local irritation in mu- cous membranes, including the eyes, nose and upper res- piratory tract (acute exposure) [1,17] and recently it has been reported that inhaled formaldehyde may cause can- cer (from chronic exposure) [5]. Because buildings in Vietnam commonly have minimal use of external win- dows and openings, and poor natural and mechanical ventilation [19], the ventilation of a given room is as- sumed to be insufficient. It is also assumed that formal- dehyde is released instan taneously to the entire roo m and distributed homogenously. Equations (4)-(6) are based on the European Technical Guidance Document on Risk Assessment [11], modified to suit clothing contact and were used to estimate formaldehyde entering the body via inhalation. For the calculation of theoretical maxi- mum concentration of formaldehyde in the air (Cvapour), the ideal gas law was utilised (see Equation 6). 3inhalationinhair breathed ExpCVFn BW (4) clothing inh vapourroom Q CC V (5) 273 22.4 101325 a vapour watera P MW CC TEM (6) where Expinhalation: formaldehyde intake to the body via mu- cous membranes (mg/kg of body weight/day) Cinh: formaldehyde concentration in air at specific sites (mg/m3) Vair breathed : the volume of air that a person breathes per day; 15 m3 for an adult, 6 m3 for a child [20] F3: fraction of formaldehyde inhaled or respired (%) (F3 = 100%) [10,21] n: exposure frequency; according to the study by Shin et al. [22] an adult stays indoor for 20 hours (13.7 hours at home, 6.4 hours for working) while a child is also in a room for 20 hours (8 hours at h ome, 12 hours at school). Assuming that if they are outdoor, there is no effect by inhalation of formaldehyde from clothing. Hence, nadult = 20/24 (day1) and nchild = 20/24 (day1). BW: body weight (kg). BWchild = 13.9 kg and BWadult = 56 kg (see Section 2.3.1). Qclothing = S × FD (kg); hence, Qclothing for adults and children is 0.3 1 (k g) and 0. 1 1 (kg ), res pect i v el y . Cvapour: concentration of formaldehyde vapours from clothing at the examined temperature of 25˚C (mg/kg). It is estimated from Cwater (the concentration of formalde- hyde in clothing as shown in Table 1). Vroom: the volume of a closed room in which people stay/work; 30 m3 for an adult, 18 m3 for a child (m3) [8]. MW: molecular weight of formaldehyde (30.03 g/mole); TEMa and Pa are the actual temperature in K and the va- pour pressure in Pascals (3,466.4 Pa at 25˚C) f or formal- dehyde, respec t ively [1]. 3Actually, consumers can change their clothes, but it is as umed that and FD are constants. Copyright © 2011 SciRes. JEP  Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers Copyright © 2011 SciRes. JEP 383 3. Results and Discussion 2.4. Acute and Chronic Exposures Many people have a habit of wearing new clothing without washing it first [23,24]. Accordingly, we distin- guished between acute exposure while wearing new clothes with a possibly higher migration rate and chronic exposure during the whole course of usage. Based on Equations (3) and (4), we first estimated acute exposure by using the first migration data, and then undertook a risk assessment of acute exposure and allergic reactions. Chronic exposure depends on experimental tests using si mulated wash, wear cycles, pH of detergents, etc, which are not readily available. Hence, alternatively, to deter- mine chronic exposure for the risk assessment of chronic toxicity, the Danish Ministry of Environment [8] and the EU Federal Institute for Risk Assessment [9] recommend using a safety factor of one-tenth (1/10) of the acute ex- posure estimates. This study concentrates on both acute and chronic exposures. 3.1. Assessment of Human Health Risk from Formaldehyde From the monitored concentrations of formaldehyde (Cwater), we estimated Csweat for dermal exposure and Cva- pour for exposure via inha lation. The results of the exposure calculations are given in Table 2 for dermal, inhalation and total exposure. Der- mal exposure is about four times (for infants) to seven times (for adults) higher than exposure via inhalation, meaning dermal exposure is the dominant route. This result agrees with the existing medical literature, i.e. the greatest concern for human health associated with for- maldehyde in clothing is allergic contact dermatitis that stems from dermal exposure [5]. It is apparent that the potential dermal exposure of a child is higher than that of an adu lt owning to lower BW of children. The results show that the average (and worst case) dermal uptakes were 0.46 (2.13 worst case) and 0.68 (3.17 worst case) mg/kg bw/day for an adult and for a child, respectively. These exposures are similar to those in the worst case research by Ellebak et al. for Danish consumers, i.e. 0.31 (adult) and 1.10 (child) mg/kg bw/day [27] and slightly lower than those in a study for European consumers (1.2 and 3.1 mg/kg bw/day, respect- tively, in the worst case). However, the maximum dose of formal- dehyde in imported clothing in Vietnam (3,517 mg/kg) is very much higher than that in Europe (162.5 mg/kg). This difference is because the research for Dan- ish and European consumers used F2 = 100% owning to absence of data, whereas we used F2 = 10% for perspire- tion zones and 5% for other zones based on the latest discus- sion for garment textiles of the EU Federal Institute for Risk Assessment [9] and the fact that that the weights of Vietnamese people are less than those of Europeans. Re- garding exposure via inhalation, estimated formaldehyde concentrations in the room sizes assumed are higher than the recommended threshold li mit value (TLV) for indoor conditions (0.15 mg/m3) [8] by three times in the average case and ten times in the worst case. Rumchev et al. [28] state that children exposed to a formaldehyde level of 60 gm3 are at increased risk of contracting asthma; in contrast, the average inhalation exposure for children in 2.5. Preliminary Risk Assessment As mentioned in the method section, MOEs can be used to assess whether formaldehyde contained in clothing has a potential adverse health effect when using such cloth- ing. To do this, data on NOAEL has been selected from available literature, where the focu s has typically been on the skin’s ability to absorb formaldehyde and inhalation of it through mucous membranes (via th e eyes, throat and nose). In this study, the two lowest NOAELs were used, namely NOAELoral (chronic) = 10 (mg/kg.day) established on the basis of a 24-month oral toxicity study of total exposure (including dermal and inhalation routes) and NOAELinhalation (acute) = 1.3 (mg/m3) based on a 3-con- secutive-day inhalation exposure [25]. The latter was also considered because many studies show that the in- halation of formaldehyde can immediately cause local irritation in mucous membranes when consumers are in contact with formaldehyde. By using MOEs it is possible to assess the human health risk to consumers from for- maldehyde in monitored clothing. The values of MOEs are calculated by Equation7, i.e. MOEtotal = NOAELo- ral/Exptotal while MOEinh = NOAELinhalation/Expinhalation [26]. OENOAEL Exp (7) Table 2. Worst case and average exposure estimates for users via each route and as a total. Route Inhalation (mg/m3) Inhalation (mg/kg/day)1 Dermal (mg/kg/day)2 Total (mg/kg/day)1 + 2 User Adult Child Adult Child Adult Child Adult Child Average 0.49 0.21 0.29 0.12 0.11 0.05 0.10 0.04 0.46 0.19 0.68 0.29 0.57 0.24 0.78 0.33 Worst case 1.53 0.90 0.34 0.32 2.13 3.17 2.47 3.49 Values in this table are acute exposures. Chronic exposures are estimated to be one-tenth of acute exposures  Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers 384 this study for children was about 290 gm3, five times higher than the level suggested by Rumchev. With respect to chronic exposure, almost all exposure routes and users have MOEs much larger than 1, even for the worst cases. Most exposure is again via the dermal route. For acute exposure, e.g. consumers wearing new clothes without washing, after ironing or hot washing (which can generate free formaldehyde from formalde- hyde carriers), MOEs are around 1, suggesting potential health risks, e.g. histopathological effects or increased cell proliferation in the nasal cavity. Since formaldehyde is highly absorbed in the respiratory and gastro-intestinal tracts [29], acute exposure via inhalation plays an impor- tant role in assessing the health risk of formaldehyde. To reduce the risk of acute inhalation exposure, washing new clothes (which results in a 90% decrease in formal- dehyde levels after one wash and a further decrease to 5% of original levels after several washes [30] and/or living in a well-ventilated room [22 ,28,31] are two of the best solutions that past studies have demonstrated. For chronic exposure, some studies report that while formal- dehyde levels may decline initially after washing, the levels may start increasing again after multiple washes. This can be explained by noting that during washing and ironing, resins fixed on clothes are broken down, be- coming more ingrained in th e fabrics [5]. This underpins the assumption that one is exposed to formaldehyde dermally and via vapours in the room during the long- term exposure. Average and worst case exposure approaches such as those in this research are often used for the screening of risk. Estimated MOEs are only a rough guide for assess- ing the health risks of formaldehyde. It has to be taken into account that exposure levels obtained from such approaches might be 10 to 100 lower than the actual ex- posure, i.e. the MOEs estimated in th is research might be 10 - 100 higher than they actually are [32,33]. A MOE of 100 is considered for defining a safe level in risk as- sessment [34] because of inter- and intra-specie varia- tions or any inherent uncertainty in databases. If a MOE of 100 is considered as ‘safe’, then one can examine Ta- ble 3 and see that for chronic exposure via inhalation, even in the worst case, and chronic dermal exposure in average cases poses no potential risks. However, the fur- ther research on the accumulation of formaldehyde in the human body should be considered to understand when formaldehyde could cause potential health risk. On the other hand, especially for the worst cases of dermal and total exposure, they are potential health risks. In short, the clothing examined in this study could cause local irritation in mucous membranes, including the eyes, nose and upper respiratory tract (owning to acute exposure via inhalation), and create health risks for Vietnamese con- sumers with chronic dermal exposure to the worst case concentrations. The advantage of the proposed model is that two fac- tors, perspiration zones and the sweat type, which were not modelled in the previous studies, are included. Fur- thermore, the model deals with the penetration ratio based on latest studies. In addition, the model combines two exposure routes (inhalation and dermal exposure), whereas past research in the EU, New Zealand and Denmark only considered dermal exposure. However, the research presented on this pape r has so me li mitation s : (1) it only uses point estimates and (2) it assesses health risks associated with imported clothing only. The former should be replaced by probabilistic estimates where suf- ficient information is available and the latter by domes- tically made clothes. With such enhancements, a more detailed and comprehensive picture of the health risk associated with formaldehyde in clothing could be made. However, since this study is the first study in terms of health risk of household produ cts in Vietnam, the lack of relevant data has limited this research. The validity of the proposed model comes from the fact that it is based on exposure models for health risk assessment developed by the European Commission (EC, 2003). The latest research by the EC on the release of formaldehyde from textiles [3] concludes that it would be better to mimic real textile usage conditions b y replacing the present water extraction analysis of formaldehyde with a modified method using artificial perspiration solu- tions. This was the reason that we changed Cwater to Csweat for the perspiration zones, thereby describing more real- istic conditions. We also based the model on the latest dermatological studies [17,18] to identify the perspiration zones where there is a high risk of irritation caused by formaldehyde. The usage of a more acute penetration ratio (F2) and inhalable ratio (F3)—as compared to past research is also appropriate, as exposure studies state that close to 100% of formaldehyde is readily absorbed in the respiratory and gastro-intestinal tracts while dermal ab- sorption of formaldehyde appears to be less [29]. 3.2. Plausibility of Adopted Legal Values of Formaldehyde The third purpose of this study is to examine the plausi- bility of the adopted Vietnamese permissible values for formaldehyde exposure for adults and children. They are set in terms of maximum legal values, being Cchild = 30 and Cadult = 75 (mg/kg textile) [6] (for comparison to ac- tual values, see Table 1). Exposure estimates and MOE values derived from the maximum legal permissible concentration are shown in Table 4. The results in Table 4 show that there should be no health problems connected with chronic exposure to the Copyright © 2011 SciRes. JEP 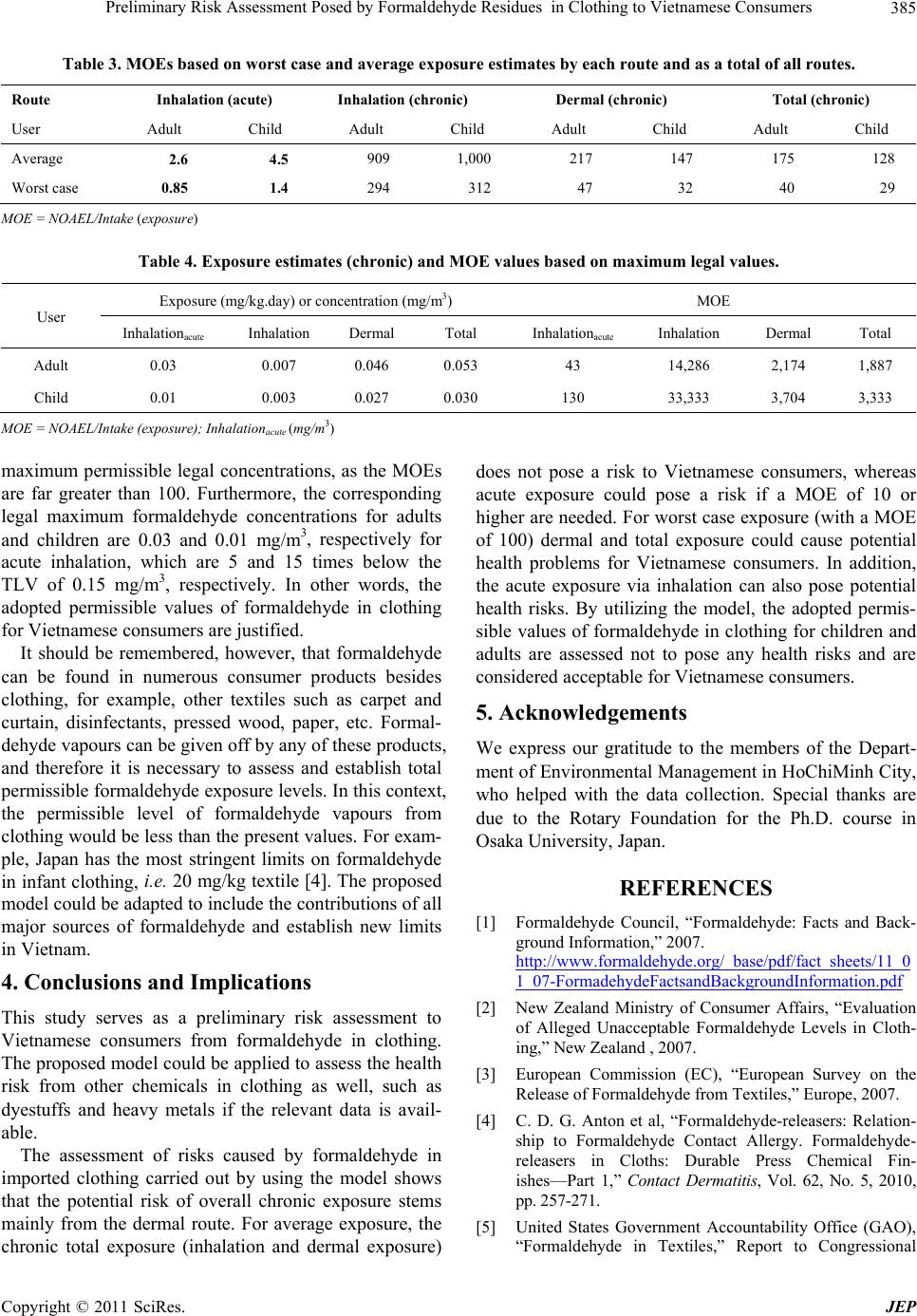 Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers385 Table 3. MOEs based on worst case and average exposure estimates by each route and as a total of all routes. Route Inhalation (acute) Inhalation (chronic) Dermal (chronic) Total (chronic) User Adult Child Adult Child Adult Child Adult Child Average 2.6 4.5 909 1,000 217 147 175 128 Worst case 0.85 1.4 294 312 47 32 40 29 MOE = NOAEL/Intake (exposure) Table 4. Exposure estimates (chronic) and MOE values based on maximum legal values. Exposure (mg/kg.day) or concentration (mg/m3) MOE User Inhalationacute Inhalation Dermal Total Inhalationacute Inhalation Dermal Total Adult 0.03 0.007 0.046 0.053 43 14,286 2,174 1,887 Child 0.01 0.003 0.027 0.030 130 33,333 3,704 3,333 MOE = NOAEL/Intake (exposure); Inhalationacute (mg/m3) maximum permissible legal concentrations, as the MOEs are far greater than 100. Furthermore, the corresponding legal maximum formaldehyde concentrations for adults and children are 0.03 and 0.01 mg/m3, respectively for acute inhalation, which are 5 and 15 times below the TLV of 0.15 mg/m3, respectively. In other words, the adopted permissible values of formaldehyde in clothing for Vietnamese consumers are justified. It should be remembered, however, that formaldehyde can be found in numerous consumer products besides clothing, for example, other textiles such as carpet and curtain, disinfectants, pressed wood, paper, etc. Formal- dehyde vapours can be given off by any of these products, and therefore it is necessary to assess and establish total permissible formaldehyde exposure levels. In this context, the permissible level of formaldehyde vapours from clothing would be less than the present values. For exam- ple, Japan has the most stringent limits on formaldehyde in infant clothing, i.e. 20 mg/kg textile [4]. The propo sed model could be adapted to include the contributions of all major sources of formaldehyde and establish new limits in Vietnam. 4. Conclusions and Implications This study serves as a preliminary risk assessment to Vietnamese consumers from formaldehyde in clothing. The proposed model could be applied to assess the health risk from other chemicals in clothing as well, such as dyestuffs and heavy metals if the relevant data is avail- able. The assessment of risks caused by formaldehyde in imported clothing carried out by using the model shows that the potential risk of overall chronic exposure stems mainly from the dermal route. For average exposure, the chronic total exposure (inhalation and dermal exposure) does not pose a risk to Vietnamese consumers, whereas acute exposure could pose a risk if a MOE of 10 or higher are needed. For worst case exposure (with a MOE of 100) dermal and total exposure could cause potential health problems for Vietnamese consumers. In addition, the acute exposure via inhalation can also pose potential health risks. By utilizing the model, the adopted permis- sible values of formaldehyde in clothing for children and adults are assessed not to pose any health risks and are considered acceptable f or Vietname se consumers. 5. Acknowledgements We express our gratitude to the members of the Depart- ment of Environmental Management in HoChiMinh City, who helped with the data collection. Special thanks are due to the Rotary Foundation for the Ph.D. course in Osaka University, Japan. REFERENCES [1] Formaldehyde Council, “Formaldehyde: Facts and Back- ground Information,” 2007. http://www.formaldehyde.org/_base/pdf/fact_sheets/11_0 1_07-FormadehydeFactsandBackgroundInformation.pdf [2] New Zealand Ministry of Consumer Affairs, “Evaluation of Alleged Unacceptable Formaldehyde Levels in Cloth- ing,” New Zealand , 2007. [3] European Commission (EC), “European Survey on the Release of Formaldehyde from Textiles,” Europe, 2007. [4] C. D. G. Anton et al, “Formaldehyde-releasers: Relation- ship to Formaldehyde Contact Allergy. Formaldehyde- releasers in Cloths: Durable Press Chemical Fin- ishes—Part 1,” Contact Dermatitis, Vol. 62, No. 5, 2010, pp. 257-271. [5] United States Government Accountability Office (GAO), “Formaldehyde in Textiles,” Report to Congressional Copyright © 2011 SciRes. JEP  Preliminary Risk Assessment Posed by Fo rmaldehyde Resid ues in Clothing to Vietnamese Consumers 386 Committees, 2010. [6] Vietnamese Ministry of Industry and Trading, “The Con- temporary Regulation of Limits of Formaldehyde and Aromatic Amines Releasing from Dyes in Import Tex- tiles,” Vietnam, 2009. [7] A. J. Scheman, P. A. Carroll, K. H. Brown and A. H. Os- burn, “Formaldehyde-Related Textile Allergy: An Up- date,” Contact Dermatitis, Vol. 38, No. 6, 1998, pp. 332-336. doi:10.1111/j.1600-0536.1998.tb05769.x [8] L. H. Paul et al., “Survey and Health Assessment of Chemical Substances in Hobby Products for Children,” Survey of Chemical Substances in Consumer Product, No. 93, 2008. [9] EU Federal Institute for Risk Assessment, “Introduction to the Problems Surrounding Garment Textiles,” 2007. [10] The Danish EPA, “Surveys on Chemicals in Consumer Products. Screening for Health Effects from Chemical Substances in Textile Colorants,” Survey, No. 57, 2005. [11] European Commission (EC), “Technical Guidance Docu- ment on Risk Assessment in Support of Directive 93/67/EEC on Risk Assessment for New Notified,” Europe, 2003. [12] Human and Environmental Risk Assessment (HERA), “Es- terquats—Human Health Risk Assessment Report,” 2009. [13] VietChina Business, 2010. http://www.vietchinabusiness.vn/i-sng/tieu-im/15213-vai- nhiem-doc-vao-viet-nam [14] V. N. Thai, A. Tokai and D. T. Nguyen, “Eco-Labeling Criteria for Textile Products with the Support of Textile Flows: A Case Study Of The Vietnamese Textile Indus- try,” Journal of Sustainable Energy & Environment, In reviewing. [15] WHO, “The Table of Height and Weight of Under-5- Year-Old Children,” 2008. http://www.choicungbe.com/tre-thong-minh/bang-chieu-c ao-va-can-nang-chuan-o-tre-duoi- 5-tuoi.ccb [16] Vietnam National Institute of Physical Science, “Survey Of The Height Of Vietnamese People,” Vietnam, 2010. [17] M.C. Ryan Et Al., “Diagnosis and Treatment of Dermati- tis Due to Formaldehyde Resins in Clothing,” American Contact Dermatitis Society, Vol. 15 , No. 4, 2004, pp. 169-175. [18] B. Mathieu Et Al., “Proportion of Skin Surface of Chil- dren and Young Infants from 2 to 18 Years Old,” Journal of Investigative Dermatology, Vol.128, 2008, pp. 461-464. [19] T.H. Dinh, “Current Status of Existing Condominium Buildings in Vietnam: Common Problems, Main Causes and Proposed Maintenance Strategies,” International Conference on Sustainable Architectural Design and Ur- ban Planning, Hanoi, 2007. [20] R. Raghunath Et Al., “Retention Times of Pb, Cd, Cu and Zn in Children’S Blood,” the Science of the Total Envi- ronment, Vol. 207, No. 2-3, 1997, pp. 133-139. doi:10.1016/S0048-9697(97)00255-6 [21] United States Department of Energy, “Guidance for Con- ducting Risk Assessment and Related Risk Activities for DOE-ORO Environmental Management,” DOE/BJC/OR -271, 1999. http://risk.lsd.ornl.gov/homepage/bjc_or–271.pdf [22] Y. Shin, D. Lee, D. Won and H. Lim, “Risk Management of Hazardous Chemicals Considering Interaction between Indoor and Outdoor Rources,” Korea Environment Insti- tute, 2007. [23] Everyday tips and thoughts, “Make Sure You Wash Those Clothes after You buy Them and before You Wear Them,” 2010 http://everydaytipsandthoughts.com/health-and-fitness/ma ke-sure-you-wash-those-clothes-after-you-buy-them-and- before-you -wear-them/ [24] H. Jill, “Wash Clothes before You Wear Them,” Fashion, Science & Technology, 2010. http://www.neatorama.com/2010/01/21/wash-clothes-befo re-you-wear-them/ [25] World Health Organization, “Formaldehyde,” Concise In- ternational Chemical Assessment Document 40, 2002. [26] H. Stefan et al., “Consumer Exposure to Biocides–identi- fication of Relevant Sources and Evaluation of Possible Health Effects,” Environmental Health, Vol. 9, 2010, p. 7. doi:10.1186/1476-069X-9-7 [27] L. S. Ellebak et al., “Survey of Chemicals in Consumer Products,” Danish Ministry of Environment and Energy, No. 23, 2003. [28] K. B. Rumchev, J. T. Speckett, M. K. Bulsara, M. R. Phil- lips and S. M. Stick, Domestic Exposure to Formaldehyde Significantly Increases the Risk of Asthma in Young Children, European Respiratory Journal, Vol. 20, No. 2, 2002, pp. 403-408. doi:10.1183/09031936.02.00245002 [29] Chemical Safety Information from Intergovernmental Organizations, “Environment Health Criteria 89–Formal- dehyde,” 2010. http://www.inchem.org/documents/ehc/ehc/ehc89.htm [30] National Institute for Public Health and Environment, “Allergens in Consumer Products,” RIVM Report 3200- 25001/2008, 2008. [31] M. H. Sherman and A. T. Hodgson, “Formaldehyde as a Basis for Residential Ventilation Rates,” Lawrence Berke- ley National Laboratory, Canada, 2002. [32] S. Hahn et al., “Health Risks from Biocide-containing Products and Articles of Daily Use,” Final Report Re- search Project 204 61 218/05 on Behalf of the German Federal Environmental Agency, 2005. [33] M. P. Van Veen, J. G. M. van Engelen and M. T. M. van Raaij, “Crossing the River Stone by Stone: Approaches For Residential Risk Assessment For Consumers,” Annual Occupational Hygiene , Vol. 45, No. S1, 2000, pp. 107- 118 . doi:10.1016/S0003-4878(00)00101-0 [34] WHO, “Assessing Human Health Risks of Chemicals: Derivation Of Guidance Values For Health-based Ex- posure Limits,” EHC 170 World Health Organization, Geneva, 1994. http://www.inchem.org/document s /ehc/e hc/ehc170.ht m. Copyright © 2011 SciRes. JEP
|