Advances in Biological Chemistry
Vol.3 No.5(2013), Article ID:38491,5 pages DOI:10.4236/abc.2013.35051
Determination of upper reference value of urinary calcium-creatinine ratio for the paediatric population in Burdwan district
![]()
1Department of Biochemistry, Burdwan Medical College, Burdwan, India
2Department of Anatomy, Burdwan Medical College, Burdwan, India
Email: mrinalpal77@rediffmail.com
Copyright © 2013 Mrinal Pal et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 17 July 2013; revised 26 July 2013; accepted 12 September 2013
Keywords: Urinary Calcium-Creatinine Ratio; Hypercalcuria; Reference Range
ABSTRACT
To estimate the rate of excretion of urinary calcium, a 24-hour sample of urine is required and this is not always easy to collect accurately in infant and children. So, random urine calcium to creatinine ratio (Ca/Cr ratio) has been developed. But as the ratio varies worldwide, reference values of the parameter in paediatric population are not developed. To determine reference value, the present study was conducted in healthy paediatric population in Burdwan district, West Bengal. This study was performed on 693 healthy paediatric subjects, aged between 3 months to 18 years and divided into five groups. Early morning non-fasting urine samples from all study groups were analyzed for Ca/Cr ratio. A negative correlation was observed between age and urinary Ca/Cr ratio, but there was no significant difference of urinary Ca/Cr ratio between two sexes. Considering 97.5th percentile of the underlying distribution of values as the upper limit of reference range, upper reference values of urinary Ca/Cr ratio for age groups of <1, 1 -< 2, 2 -< 5, 5 -< 10 and 10 - 18 years in mg/mg of 1.61, 1.38, 1.13, 0.89 and 0.71 respectively were derived. As the upper reference values of urinary Ca/Cr ratio of different age groups in present study are different from other previous studies conducted in different areas, we conclude that upper reference value of urinary Ca/Cr ratio should be estimated in every geographic area.
1. INTRODUCTION
The prevalence of idiopathic hypercalciuria (IH) has been reported to vary between 2.9% - 6.2% in the age group of 3 months to 18 years [1-6]. The majority of these cases are asymptomatic. Symptomatic cases have various manifestations such as gross hematuria, dysuria, nocturnal enuresis, urinary frequency—urgency syndrome, supra-pubic and abdominal pain and recurrent urinary tract infections [7]. It predisposes to nephrolithiasis that may cause renal damage. These complications are avoidable if appropriate preventive measures are undertaken by early detection of IH. It is done by measurement of urinary calcium excretion, but it is difficult to take the accurate 24 hours urine in young and non-toilet trained children. Therefore, hypercalcuria can be screened by random urine Ca/Cr ratio [8-10] preferably fasting. It is incumbent on a laboratory to report urinary Ca/Cr ratio, and a reference interval must be required above which a result is considered abnormal, but these cut-offs are not firmly established because of difficulties of generating reference intervals for children particularly across the span of ages in childhood [11]. Reference values for urine calcium/ creatinine ratio in normal infant and children have been reported by several authors worldwide, but these data are controversial, possibly due to the differences between study populations, genetic characteristics and the variations in dietary intake of calcium, sodium and protein in different geographic regions [1-4,9, 10,12-15]. So the objective of the present study was to determine urine Ca/Cr ratio in healthy infant and children in Burdwan district, West Bengal.
2. MATERIAL AND METHODS
2.1. Selection of Subjects
A total of 693 normal infant and children aged 3 months to 18 years from three public schools and a well-baby clinic of Burdwan district were selected by simple random sampling after informed consent had been received from the parents between March 2011 and May 2013. Among them three hundred twenty (53.82%) were boys and 195 (46.18%) were girls All of them had normal physical growth and blood pressure. They were told not to change their eating habits and physical activities. Children with conditions that would influence urinary calcium excretion such as being on medical treatment or suffering from malnutrition, chronic disease such as kidney diseases, metabolic disorders were excluded. Then the study population was divided into five groups according to their age: Group I: <1 year, Group II: 1 -< 2 years, Group III: 2 -< 5 years, Group IV: 5 -< 10 years and Group V: 10 - 18 years.
2.2. Collection of Samples
Early morning non-fasting urine sample were collected from the study population to determine calcium and creatinine levels. After collection all the tests were done immediately.
2.3. Parameters Assay
Urinary calcium was estimated by 2-cresolphthalein complexone method [16] using semi auto analyser (Chem 5v2 plus). Intra assay CV% was 1.5 and inter assay CV was 2.7 for this method. Urinary creatinine concentration was assayed by modified Jaffes’ method [17] using (Chem 5v2 plus) semiautoanalyser. Intra-assay CV% was 1.8 and inter-assay CV% was 2.9. Then urinary Ca/Cr (mg/mg) ratio was calculated.
2.4. Statistical Analysis
The data for biochemical analysis was subjected to standard statistical analysis using the Statistical Package for Social Science (SPSS) 11.5 software for windows.
3. RESULT
In Burdwan district the distribution of urinary Ca/Cr ratio in the paediatric study population is depicted in Figure 1.
Table 1 showed the mean, standard deviation and percentile values of different age group. It was found that there was decrease in urinary Ca/Cr ratio as age of the study population increased and this ratio significantly negative correlate (Pearson Correlation −0.217) with increasing age (p < 0.01) analysed by Pearson correlation. It was also seen that different percentile values of each age group also decreased according to increased age.
Although urinary Ca/Cr ratio and its 97.5th percentile value were more in girls, the different did not show significant difference (p > 0.01) as shown in the Table 2.
Figure 2 shows the comparison between the percentile values of different age groups and it is shown that there was definite decrease in percentile values according to increasing of age.
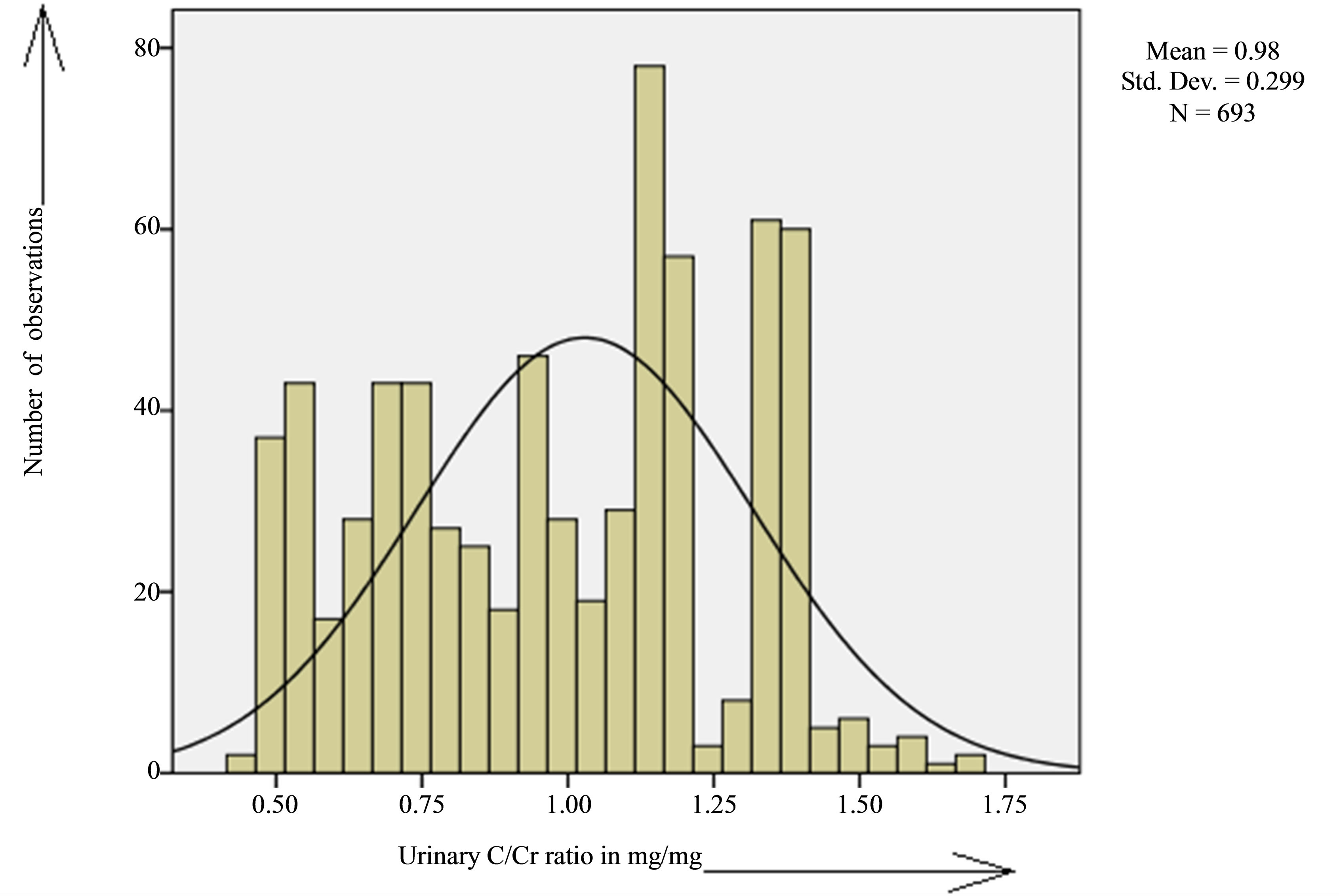
Figure 1. Frequency distribution of urinary Ca/Cr ratio in paediatric study population in Burdwan district.
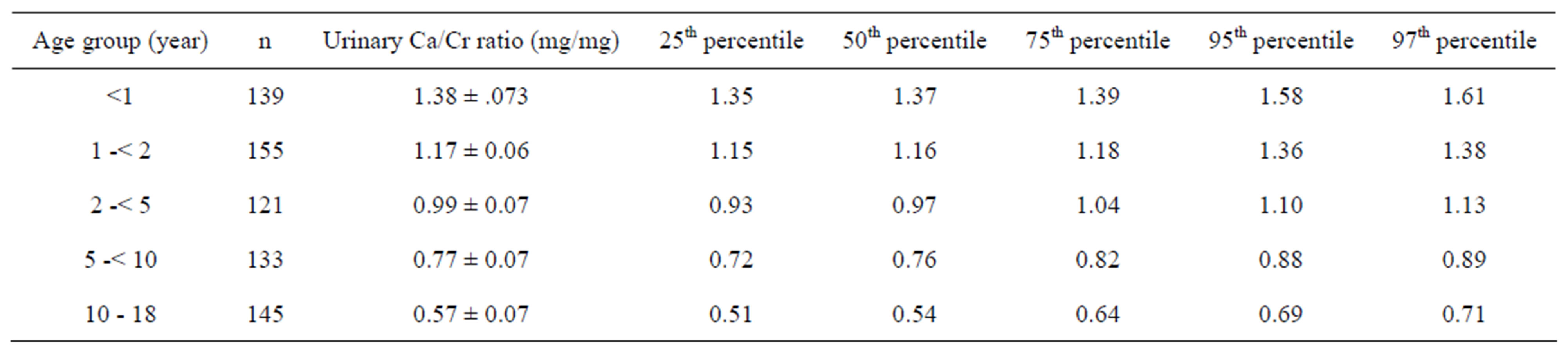
Table 1. Ca/Cr ratio in urine and its percentile values of different age group.
Value are mean ± SD; n = number of cases in each group.

Table 2. Urinary Ca/Cr ratios of study population based on different age groups and sex.
Values are mean ± SD; n = number of cases in each group; p > 0.05 consider statistically insignificant.
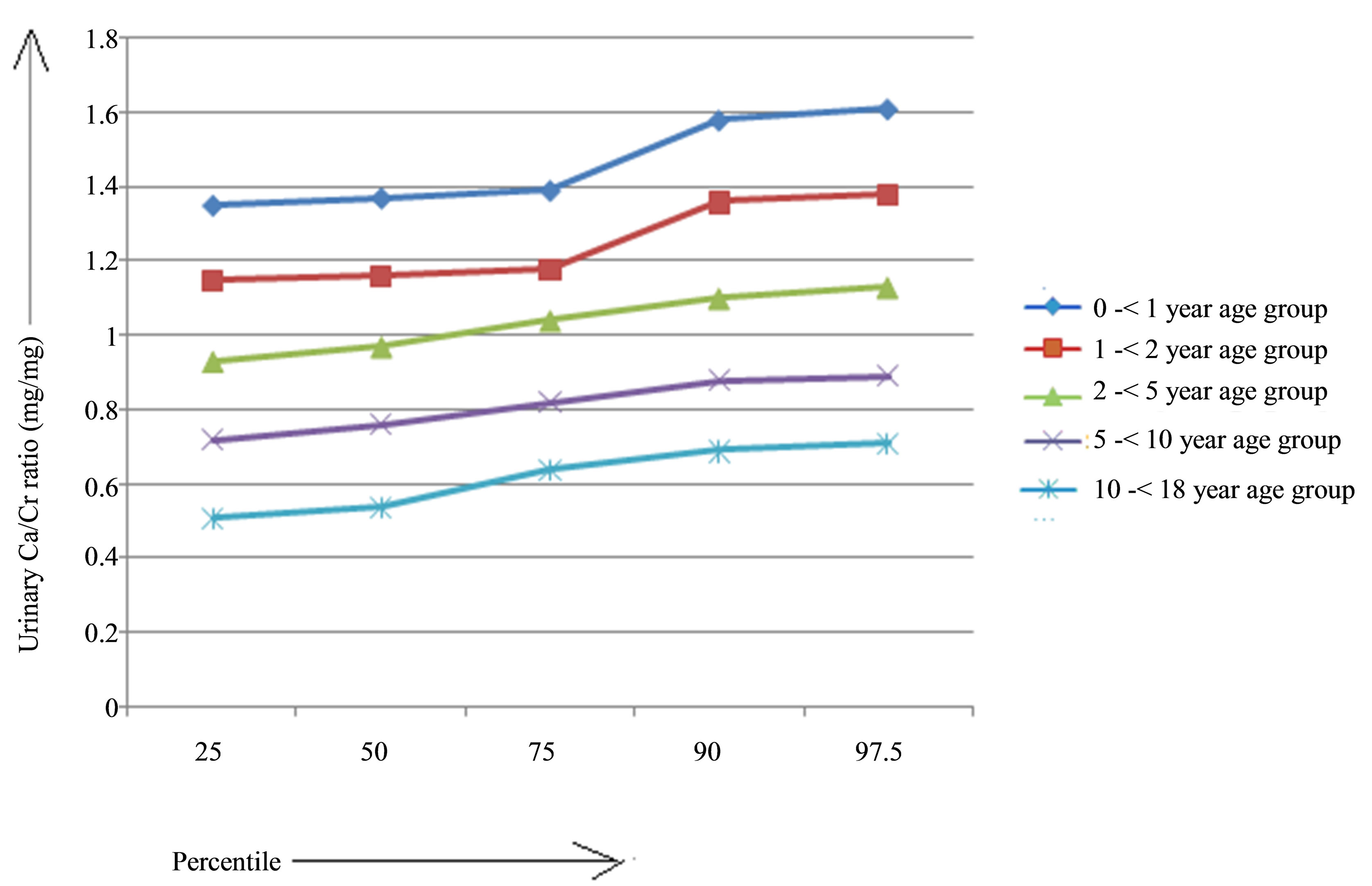
Figure 2. Comparison of percentile values of different age groups in present study population.
After calculating the upper reference of urinary Ca/Cr ratio, it was found that upper reference value of this parameter has got inverse relationship with age as observe in the Table 3.
4. DISCUSSION
In children urinary Ca/Cr ratio is a useful and reliable method for determining hypercalcuria and also is a non-invasive and relatively inexpensive method [18]. But reference interval of this parameter for the paediatric age group is not yet established as it is dependent on several factors such as age, geographical area. So the present study was conducted to establish a reference interval in our study area and it was first found that there was a significant inverse relationship between urinary Ca/Cr ratio and age. This finding was well corroborated with several previous studies [9,16,19-22]. It also observed that for every age group, different urine Ca/Cr ratio was reported [3,8,23]. This difference may be due to exposure to sunlight, climate, genetics, nutritional habits, drinking water and ethnicity. In respect to relationship between Ca/Cr ratio of urine and age, another important observation was that same as few older studies [8], there was higher level of urinary Ca/Cr ratio in infant than other age group. It is may be secondary to low creatinine excretion per unit body mass [8] and also tubular immaturity to excrete creatinine [11]. If sex factor is considered, as previous reports it was found that there was no significant difference in urinary Ca/Cr ratio between both sex [9,13,19,22]. As for most analytes, the lower and upper reference limits are assumed to demarcate the estimated 2.5th and 97.5th percentiles respectively, of the underlying distribution of values [24], percentile values of urinary Ca/Cr ratio were calculated. 95th and 97.5th percentile for urinary Ca/Cr ratio of different age groups in present study in this geographic area was the same as some reports and different with other [1,6,9,10,14-15,18- 23,25-29]. Then upper reference value of urinary Ca/Cr ratio of different age group were found and this to some extent different from one previous study [11]. Despite the disagreement between the upper reference value in
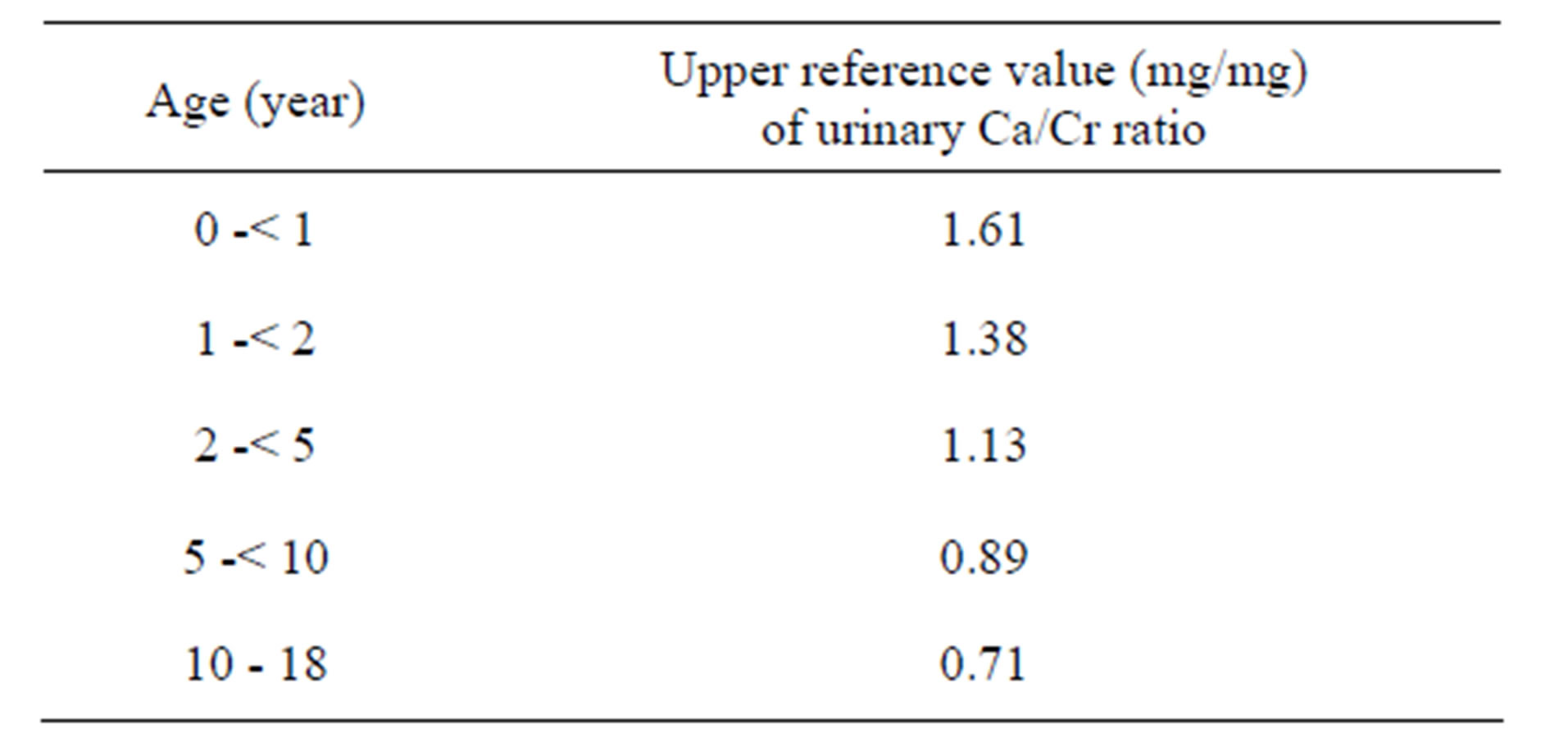
Table 3. Determined upper reference value of urinary Ca/Cr ratio in different age groups.
this report and other, the accumulated data support the higher and changing upper reference value that have been adopted for use in day-to-day clinical practice at this institution.
5. CONCLUSION
The present study showed parallel to other studies that urinary Ca/Cr ratio values of different age groups may differ according to geographic location. So, for screening of hypercalciuria, upper reference values of random urinary Ca/Cr ratio in different paediatric age groups should be determined in each geographic location.
6. ACKNOWLEDGEMENTS
Authors are thankful to Professor (Dr). Keya Pal, Mr. Naba Kumar Das and Mr. Chandi Charan Das of Burdwan Medical College and Hospital for constant assistance & support.
REFERENCES
- Esbjörner, E. and Jones, I.L. (1995) Urinary calcium excretion in Swedish children. Acta Paediatrica, 84, 156- 159. http://dx.doi.org/10.1111/j.1651-2227.1995.tb13600.x
- Alconcher, L.F., Castro, C., Quintana, D., et al. (1997) Urinary calcium excretion in healthy school children. Pediatric Nephrology, 11, 186-188. http://dx.doi.org/10.1007/s004670050256
- Sweid, H.A., Bagga, A., Vaswani, M., Vasudev, V., Ahuja, R.K. and Srivastava, N. (1997) Urinary excretion of minerals, oxalate, and uric acid in North Indian children, Pediatric Nephrology, 11, 189-192. http://dx.doi.org/10.1007/s004670050257
- Lopez, M.M., Castillo, L.A., Chavez, J.B. and Ramones, C. (1999) Hypercalciuria and recurrent urinary tract infection in Venezuelan children. Pediatric Nephrology, 13, 433-437. http://dx.doi.org/10.1007/s004670050635
- Moore, E.S., Coe, F.L., Me Mann, B.J. and Farus, M.J. (1978) Idiopathic hypercalciuria in children: Prevalence and metabolic characteristics. Journal of Pediatrics, 92, 906-910. http://dx.doi.org/10.1016/S0022-3476(78)80358-8
- Kruse, K., Kracht, U. and Kruse, U. (1984) Reference values for urinary calcium excretion and screening for hypercalciuria in children and adolescents. European Journal of Pediatrics, 143, 25-31. http://dx.doi.org/10.1007/BF00442743
- Heiliczer, J.D., Canonigo, B.B., Bishof, N.F. and Moore, E.S. (1987) Noncalculi urinary tract disorders secondary to idiopathic hypercalciuria in children. Pediatric Clinics of North America, 34, 711-717.
- Sargent, J.D., Stukel, T.A. and Kresel, J. (1993) Normal values for random urinary calcium to creatinine ratios in infancy. Journal of Pediatrics, 123, 393-397. http://dx.doi.org/10.1016/S0022-3476(05)81738-X
- Safarinejad, M.R. (2003) Urinary mineral excretion in healthy Iranian children. Pediatric Nephrology, 18, 140- 144.
- Kaneko, K., Tsuchiya, K., Kawamura, R., et al. (2002) Low prevalence of hypercalciuria in Japanese children. Nephron, 91, 439-443. http://dx.doi.org/10.1159/000064284
- Metz, M.P. (2006) Determining urinary calcium/createnine cut-offs for the paediatric population using published data. Annals of Clinical Biochemistry, 43, 398-401. http://dx.doi.org/10.1258/000456306778520106
- De Santo G., Di Lorio, B. and Capasso, G. (1992) Population based data on urinary excretion of calcium, magnesium, oxalate, phosphate and uric acid in children from Cimitile (southern Italy). Pediatric Nephrology, 6, 149- 157. http://dx.doi.org/10.1007/BF00866297
- Kaneko, K., Chiba, M., Hashizume, M., et al. (2002) Extremely high prevalence of hypercalciuria in children living in the Aral Sea region. Acta Paediatrica, 91, 1116-1120. http://dx.doi.org/10.1111/j.1651-2227.2002.tb00108.x
- Nikibakhsh, A., Seyedzadeh, A. and Mahmoodzadeh, H. (2008) Normal values for random urinary calcium to creatinine ratio in Iranian children. Iranian Journal of Pediatrics, 18, 263-266.
- Honarpisheh, A., Hooman, N. and Taghavi, A. (2009) Urinary calcium excretion in healthy children living in Kashan/Iran. Iranian Journal of Pediatrics, 19, 154-158.
- Lorentz, K. (1982) Improved determination of serum calcium with 2-cresolphthalein Complexone. Clinica Chimica Acta, 126, 327-334. http://dx.doi.org/10.1016/0009-8981(82)90308-4
- Varley, H. (1975) Practical clinical biochemistry. 4th edn. India Arnold Heinemann Publisher, 197-198.
- Emamghorashi, F., Davami, M.H. and Rohi, R. (2010) Hypercalciuria in Jahrom’s school—Age children what is normal calcium-creatinine ratio? Iranian Journal of Kidney Diseases, 4, 112-115.
- Vachvanichsanong, P., Lebel, L. and Moore, E.S. (2000) Urinary calcium excretion in healthy Thai children. Pediatric Nephrology, 14, 847-850. http://dx.doi.org/10.1007/s004679900229
- Kaufman, J.M., Martin, L.G. and Seegmiller, J.E. (1968) Urine uric acid to creatinine ratio, a secreening test for inherited disorders of purine metabolism. Journal of Pediatrics, 4, 583-592. http://dx.doi.org/10.1016/S0022-3476(68)80274-4
- Caren, O., Akin, M. and Akturk, Z. (2003) Normal urinary calcium/creatinine ratios in Turkish children. Indian Pediatrics, 40, 884-887.
- Sorkhi, H. and Aahmadi, M.H. (2005) Urinary calcium to creatinine ratio in children. Indian Journal of Pediatrics, 72, 1055-1056. http://dx.doi.org/10.1007/BF02724412
- Chen, Y.H., Lee, A.J., Chen, C.H., et al. (1994) Urinary mineral excretion among normal Taiwanese children. Pediatric Nephrology, 8, 36-39. http://dx.doi.org/10.1007/BF00868256
- Horn, P.S. (2010) Reference intervals and clinical decision limits. In: Kaplan, L.A. and Pesce, A.J., Eds., Clinical Chemistry, 5th Edition, Missouri USA, Mosby Elsevier, 444.
- So, N.P., Osorio, A.V., Simon, S.D., et al. (2001) Normal urinary calcium creatinine ratios in African-American and Caucasian children. Pediatric Nephrology, 16, 133- 139. http://dx.doi.org/10.1007/s004670000510
- Rath, B., Aggarwal, M.K., Mishra, T.K., Talukdar, B., Murthy, N.S. and Kabi, B.C. (1994) Urinary calcium creatinine raio and hypercalciuria. Indian Pediatr, 31, 311-316.
- Davis, I.D. and Avner, E.D. (2007) Upper urinary tract causes of hematuria. In: Kliegman, R.M., Behrman, R.E., Jenson, H.E., Stanton, B.M.D., Eds., Nelson Textbook of Pediatrics, 18th Edition, WB Saunders, Philadelphia, 2184.
- Sonmez, F., Akcanal, B., Altincik, A., et al. (2007) Urinary calcium excretion in healthy Turkish children. International Urology and Nephrology, 39, 917-922. http://dx.doi.org/10.1007/s004670000510
- Vachvanichsanong, P., Lebel, L. and Moore, E.S. (2000) Urinary calcium excretion in healthy Thai children. Pediatric Nephrology, 14, 847-850. http://dx.doi.org/10.1007/s004679900229