M. Saita et al. / Health 3 (2011) 300-303
Copyright © 2011 SciRes. Openly accessible at http://www.scirp.org/journal/HEALTH/
303303
greater efficacy than oseltamivir or zanamivir in im-
proving joint pain . This finding is corroborated by Ku bo
and Nishimura who found that treatment with maoto or
maoto-oseltamivir combination was more effective than
oseltamivir alone in shortening the duration of fever [12].
If we take into account the fact that maoto has been his-
torically used to treat cold symptoms based on (symptom)
pattern diagnosis in Kampo medicine, it is not surprising
to discover its efficacy to be on par with antivirals which
are specifically designed to suppress viral replication.
Hence, our results are clinically significant, given the
scarcity of data on maoto’s efficacy in influenze from
prospective randomized trials.
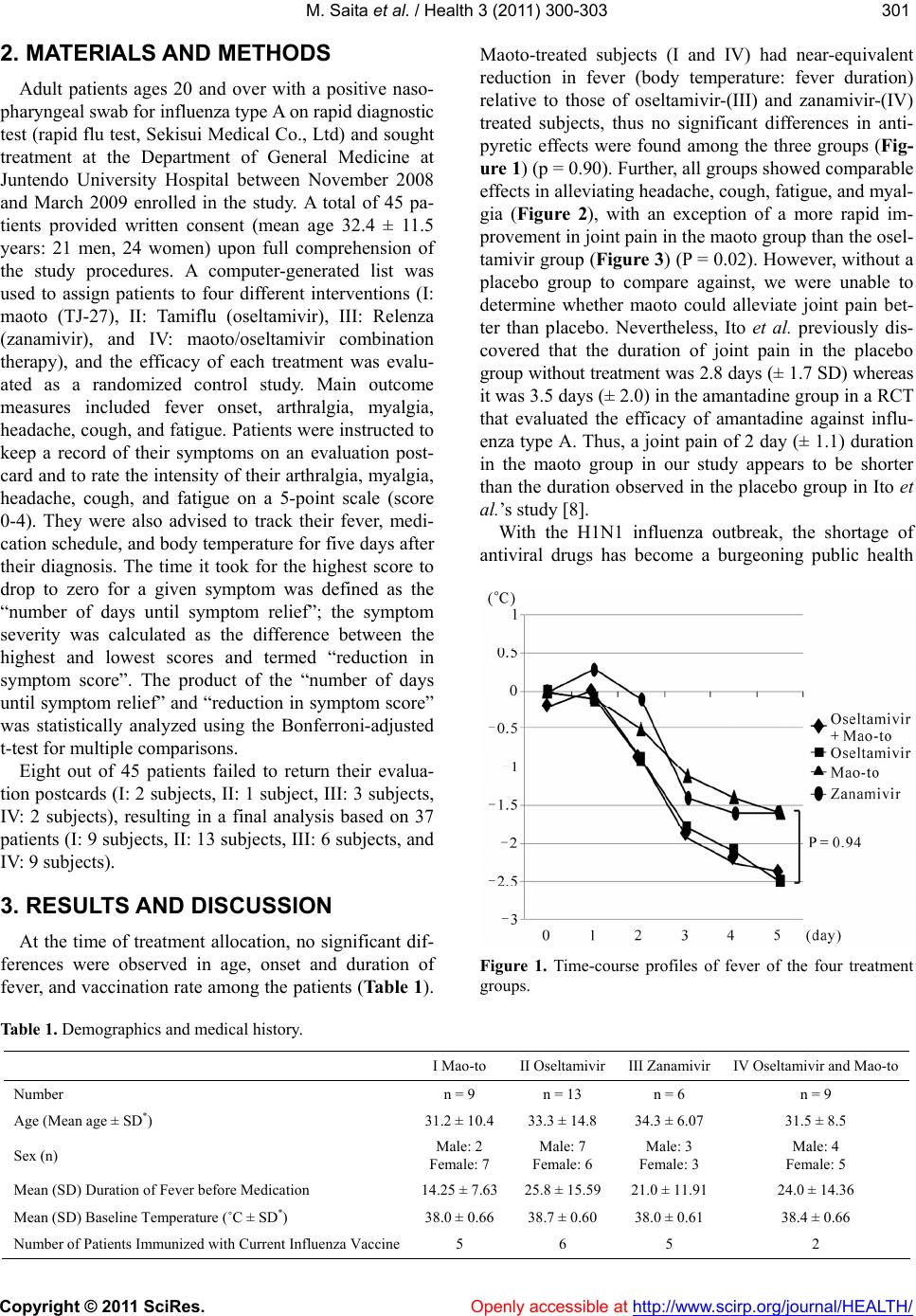
Oseltamivir showed strong but statistically insignifi-
cant antipyretic effect. Figure 1 depicts the antipyretic
effect of both oseltamivir administered groups (II and
IV).
Zanamivir-treated group showed a rapid improvement
in cough than the other three group s. Though statistically
unremarkable, our results un dergird the trad itiona l use o f
Zanamivir as a potent respiratory agent.
While efforts to discover novel antiviral agents and
oseltamivir-related problems continue to attract attention,
maoto’s effect in influenza as endorsed by the NHI and
observed in our prospective study are useful information
for both healthcare practitioners and patients.
Except for one patient developing nausea from the
maoto’s distinct odor, no other serious adverse events
were reported during the study. Based on our observa-
tions, nine patients on maoto/oseltamivir combination
therapy, who were anticipated to achieve a greater over-
all symptom relief than patients in other treatment
groups, did not demonstrate apparent benefits of the
combination therapy.
The absence of a control group with inert placebo and
a control group without treatment due to insurance pur-
poses were two important caveats in this study. Addi-
tionally, we did not investigate the effect of maoto in
other influenza types because all patients recruited for
the study were uniformly infected with type A virus,
although Toriumi et al. had previously found that maoto
was as effective as oseltamivir and zanamivir in reduc-
ing fever in pediatric patients with type B influenza [13].
As the speed and routes of H1N1 propagation gain mo-
mentum, clinically-oriented studies based on isolated
strains may halt further global catastrophe.
In summary, we found that maoto improved systemic
influenza symptoms during the active disease phase as
effectively, if not, better than antiviral drugs. Moreover,
because none of the patients receiving maoto or maoto/
antiviral combination therapy suffered adverse drug re-
actions, maoto appeared to have a slightly wider safety
margin than antiviral drugs. Maoto may curb the devel-
opment of drug resistance to antivirals caused by their
misuse and overuse, and serve as an elegant option for
the treatment of influenza.
REFERENCES
[1] WHO (2008) Brief summary of analyses of the 2007
survey on the capacity of National Influenza Centres.
World Health Organization Geneva, 83, 133-1448.
[2] WHO (2009) Interim planning considerations for mass
gatherings in the context of pandemic (H1N1) 2009 in-
fluenza.
[3] Dharan, N.J., Gubareva, L.V., Meyer, J.J., Okomo-
Adhiambo, M., McClinton, R.C., Marshall, S.A., St.
George, K., Epperson, S., Brammer, L., Klimov, A.I.,
Bresee, J.S., Fry, A.M. (2009) Infections with osel-
tamivir-resistant influenza A(H1N1) virus in the United
States. Journal of the American Medical Association, 301,
1034-1041. doi:10.1001/jama.2009.294
[4] Hatoyama, S. and Koeike, K. (2009) Development and
management of oseltamivir-resistant influenza. The Japa-
nese Society of Internal Medicine, 98, 1733-1741.
[5] Centers for Disease Control and Prevention (CDC) (2006)
High levels of adamantane resistance among influenza A
(H3N2) viruses and interim guidelines for use of antiviral
agents-United States, 2005-2006 influenza season. Mor-
bidity and Mortality Weekly Report, 55, 44-46.
[6] IDSC (2008) Infectious Disease Surveillance Center,
2007/2008 influenza season, Japan. Infectious Agents
Surveillance Report, 29, 297-298.
[7] World Health Organization 2009) Influenza A(H1N1)
virus resistance to oseltamivir—2008/2009 influenza
season, northern hemisphere.
[8] Ito, S., Iijima, N., Kanemaki, K., Hayashi, S., Hujii, S.,
Watanabe, T., Hosokawa, T. and Kakehi, K. (2000)
Therapeutic efficacy of amantadine hydrochloride in pa-
tients with epidemic influenza A virus infection. Nihon
Kokyuki Gakkai Zasshi, 38, 897-902.
[9] Chiharu, K., Masatsugu, O., Miwako, S., Yuzo, N., Ma-
koto, U., Takako, O., Mami, I., Takahiro, T. and Masato,
T. (2009) Isolation of oseltamivir-resistant influenza
A/H1N1 virus of different origins in Yokohama city, Ja-
pan, during the 2007-2008 influenza season. Japanese
Journal of Infectious Diseases, 62, 83-86.
[10] Hayashi, K., Imanishi, N., Kashiway ama, Y., Kawano, A.,
Terasawa, K., Shimada, Y. and Ochiai, H. (2007) Inhibi-
tory effect of cinnamaldehyde, derived from Cinnamomi
cortex, on the growth of influenza A/PR/8 virus in vitro
and in vivo. Antiviral Research, 74, 1-8.
doi:10.1016/j.antiviral.2007.01.003
[11] Hattori, T. (2007) Hochuekito for biodefense and viral
infections. Mebio, 24, 16-21.
[12] Kubo, T. and Nishimura, H. (2007) Antipyretic effect of
Mao-to, a Japanese herbal medicine, for treatment of
type A influenza infection in children. Phytomedicine, 14,
96-101 (article in Japanese with En g l i s h ab s t r a c t ).
doi:10.1016/j.phymed.2006.09.015
[13] Toriumi, Y., Takahashi, I., Kamei, T. and Murata, K.
(2010) Antipyretic effect of Maoto in treatment of type B
influenza infection in children. Journal of Epidemiology,
20, 360, (Article and abstract in Japanese).