E. M. Karabulut, T. Ibrikci
problem from different area, can fail for a different problem. Therefore, search should be broadened for a com-
puter solution especially for a medical decision. Therefore, the results of prior studies are considered in our
analysis of CTG. The determination of state of fetus is especially important for early intervention of required
cases, i.e. fetal distress or preventing unnecessary surgeries.
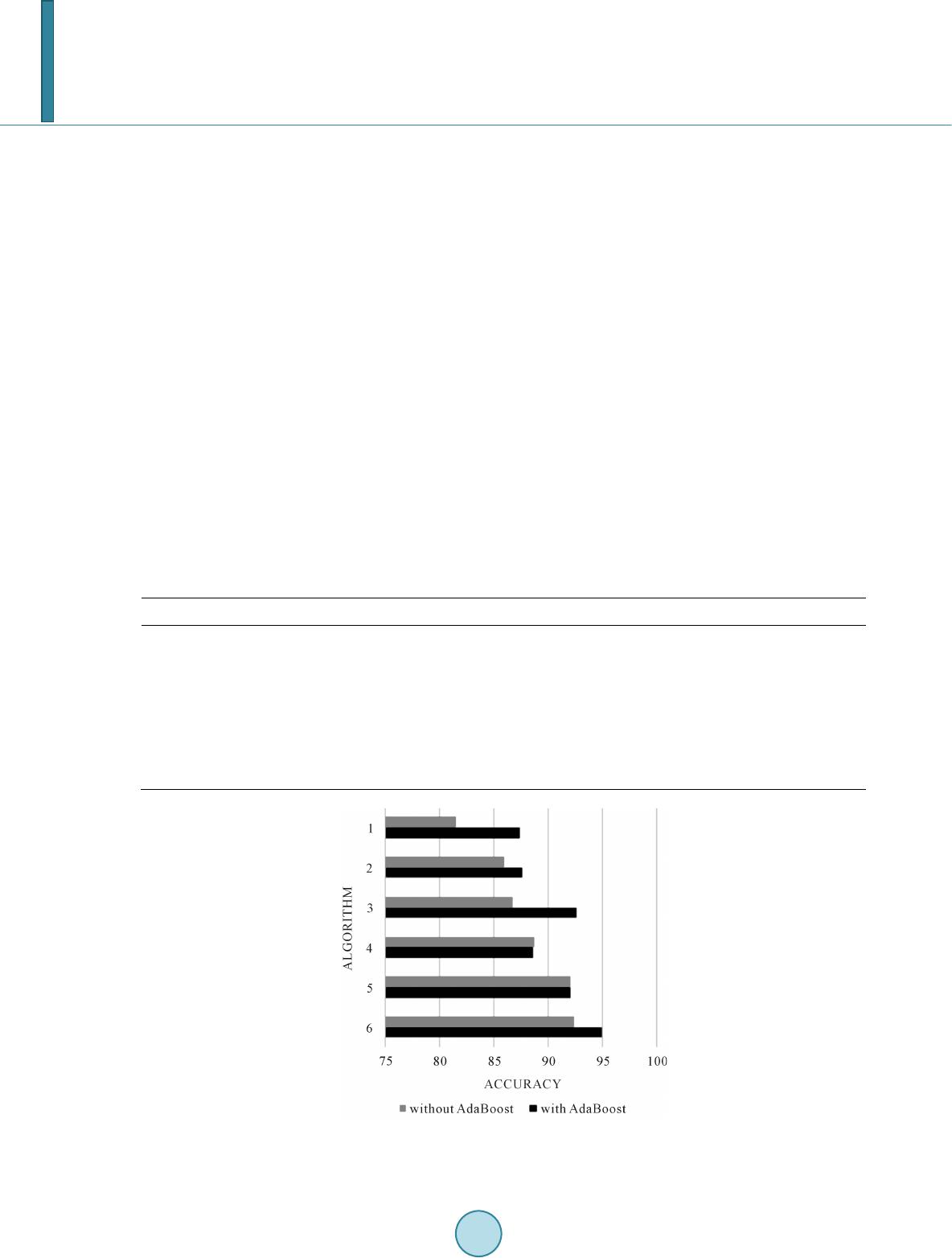
The effect of using AdaBoost ensemble on classifiers is investigated for perfect determination of fetal distress
from CTG data in this study. Figure 2 visually represents the promising results of experiments related to contri-
bution of AdaBoost ensemble on classifying machine learning algorithms, confirming the fact that ensemble
machine learning approaches often performs much better than single classifiers that make them up [12]. The
most prominent result belongs to decision tree based AdaBoost algorithm by 0.034 MAE, 0.861 kappa statistics
and 95.01% accuracy, meaning that 2020 of 2126 samples are perfectly predicted. These results are an improved
next step following the related studies carried out in literature.
References
[1] Steer, P.J. (2008) Has Electronic Fetal Heart Rate Monitoring Made a Difference? Seminars in Fetal and Neonatal Me-
dicine, 13, WB Saunders, 2-7.
[2] Huang, M. and Hsu, Y. (2012) Fetal Distress Prediction Using Discriminant Analysis, Decision Tree, and Artificial
Neural Network. Journal of Biomedical Science & Engineering, 5, 526-533.
http://dx.doi.org/10.4236/jbise.2012.59065
[3] Sundar, C., Chi tra devi , M. and Geetharamani, G. (2012) Classification of Cardiotocogram Data Using Neural Network
Based Machine Learning Technique. International Journal of Computer Applications, 47, 19-25.
http://dx.doi.org/10.5120/7256-0279
[4] Sundar, C., Chi trad evi, M. and Geetharamani, G. (2013) An Overview of Research Challenges for Classification of
Cardiotocogram Data. Journal of Computer Science, 9, 198-206. http://dx.doi.org/10.3844/jcssp.2013.198.206
[5] Yılmaz, E. and Kılıkçıer, Ç. (2013) Determination of Fetal State from Cardiotocogram Using LS-SVM with Particle
Swarm Optimization and Binary Decision Tree. Computational and Mathematical Methods in Medicine, 20 13, 2013.
http://dx.doi.org/10.1155/2013/487179
[6] Newman, D.J., Heittech, S., Blake, C.L. and Merz, C.J. (1998) UCI Repository of Machine Learning Datab ases. Uni-
versity California Irvine, Department of Information and Computer Science.
[7] Fr eu nd, Y. and Schapire, R. (1996) Experiments with a New Boosting Algorithm. Machine Learning: Proceedings of
the Thirteenth International Conference, 1996, 148-156.
[8] Kuncheva, L. (2004) Combining Pattern Classifiers Methods and Algorithms. Wiley-Interscience, 360.
http://dx.doi.org/10.1002/0471660264
[9] Duda, O.R., Hart, P.E. and Stork, D.G. (2006) Pattern Classification. John Wiley & Sons Inc.
[10] Tanner, L., et al. (2008) Decision Tree Algorithms Predict the Diagnosis and Outcome of Dengue Fever in the Early
Phase of Illness. PLoS Neglected Tropical Diseases, 2, e196. http://dx.doi.org/10.1371/journal.pntd.0000196
[11] Hall, M., Frank, E., Holmes, G., Pfahringer, B., Reutemann, P. and Witten, I.H. The WEKA Data Mining Software: An
Update. SIGKDD Explorations, 11, 1.
[12] Wang, C.W. (2006) New Ensemble Machine Learning Method for Classification and Prediction on Gene Expression
Data. Engineering in Medicine and Biology Society, 2006. EMBS’06. 28th Annual International Conference of the
IEEE, 2006, 3478-34 81 .