L. Ousehal et al. / Open Journal of Stomatology 1 (2011) 1-6 5
in an American study [6].
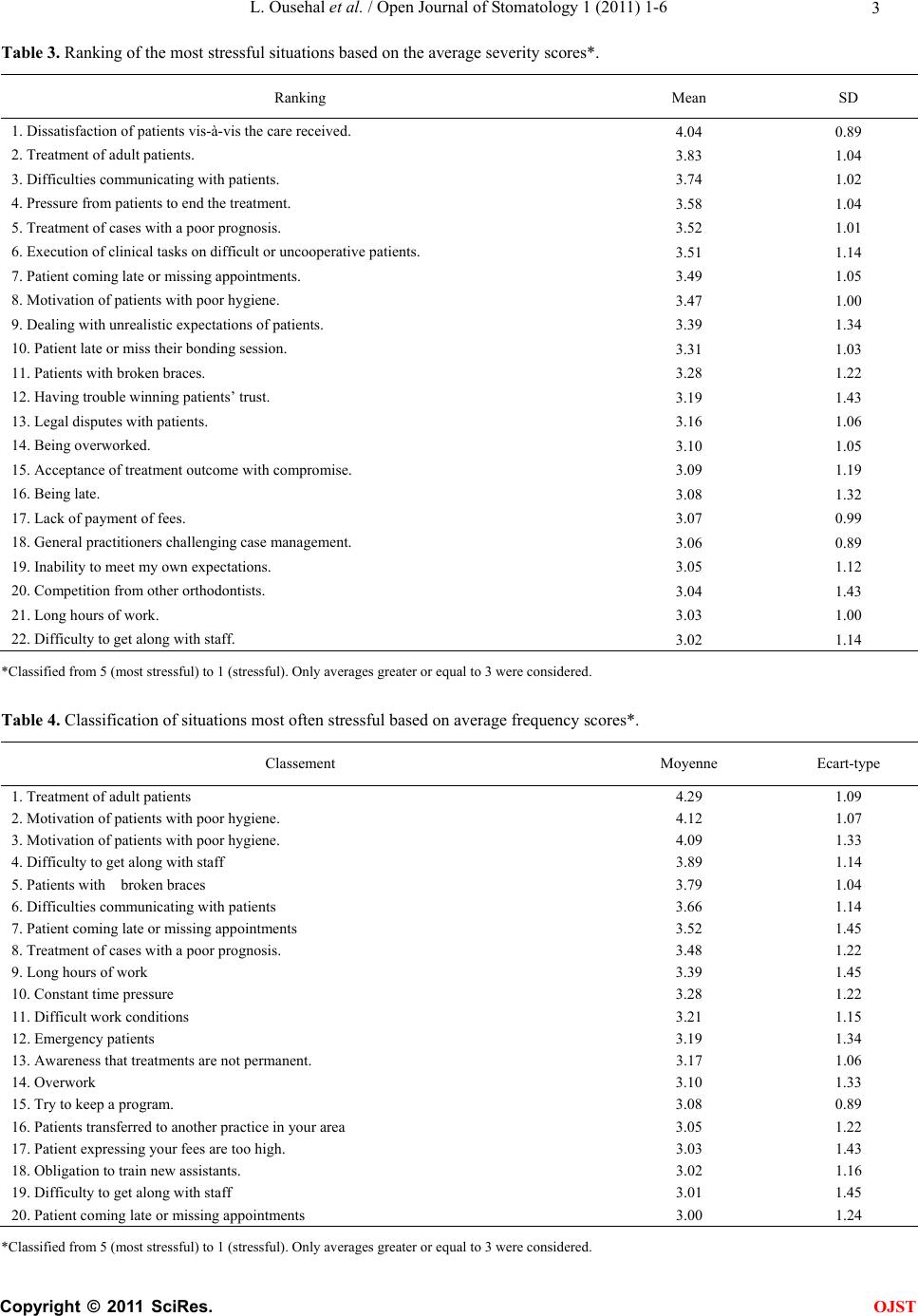
Regarding the most stressful aspects, the three factors
most strongly affected were: patient dissatisfaction
vis-à-vis the care received, treatment of adult patients,
and the lack of communication with patients. Compared
with the Canadian study [5 ], only the first factor has been
ranked among the top three most stressful factors. The
remaining factors are: the execution of clinical tasks on
difficult or uncooperative patients that have fallen be-
hind.
Other factors of stress that are similar to the Canadian
[5] study are: patients late or missing their bonding ses-
sions, patients with broken appliances, the constant
pressure of time, acceptance of treatment outcome with
compromises, treatment of cases with a poor prognosis,
and the medico-legal cases.
Many similarities were also observed between the re-
sults of this study and those reported in general dentistry
that also made reference to the factors leading the most
to stress, mainly: the dissatisfaction of patients, patients
with difficult or uncooperative patients and emergency.
Two situations have been reported as being stressful in
general dentistry, but have not proven highly stressful in
orthodontics, these included the perception of the practi-
tioner as a source of pain and frequent decision making.
However, many other situations have been reported as
stressful in the orthodontic population, but they are not
common in studies of general dentistry. These include:
pressure from patients and/or parents to remove the de-
vices before the end of treatment, the awareness that
treatment is not permanent, general practitioners chal-
lenging case management, and deal with unrealistic ex-
pectations of patients. This suggests that stress in ortho-
dontics is associated to the particularity of the specialty
in addition to the general characteristics of dental prac-
tice.
Despite the many similarities between the results of
the study and the Canadian study [5], analysis of the
most concerned factors in orthodontics showed a big
difference.
The four largest factors of stress among Canadian or-
thodontists were those related to time management [5,8 ].
Orthodontists in Casablanca ranked this factor second
after the factor “patient”.
Indeed, treatment of adult patients, the difficulty of
communication with patients require more attention and
therefore more “work hours”, just as patients coming late
or missing their meeting bonding and patients missing
their appointments also generate disturbances at the level
of “hours”.
So all these factors cause an increase in working hours,
leading orthodontists to be under stress.
This result is consistent with that of Vander Hulst [9]
which proved an association between long working hours
and adverse health manifested by fatigue, stress and gen-
eral diseases such as diabetes and cardiovascular disease.
5.3. Factors Affecting the Occupational Stress in
Orthodontics
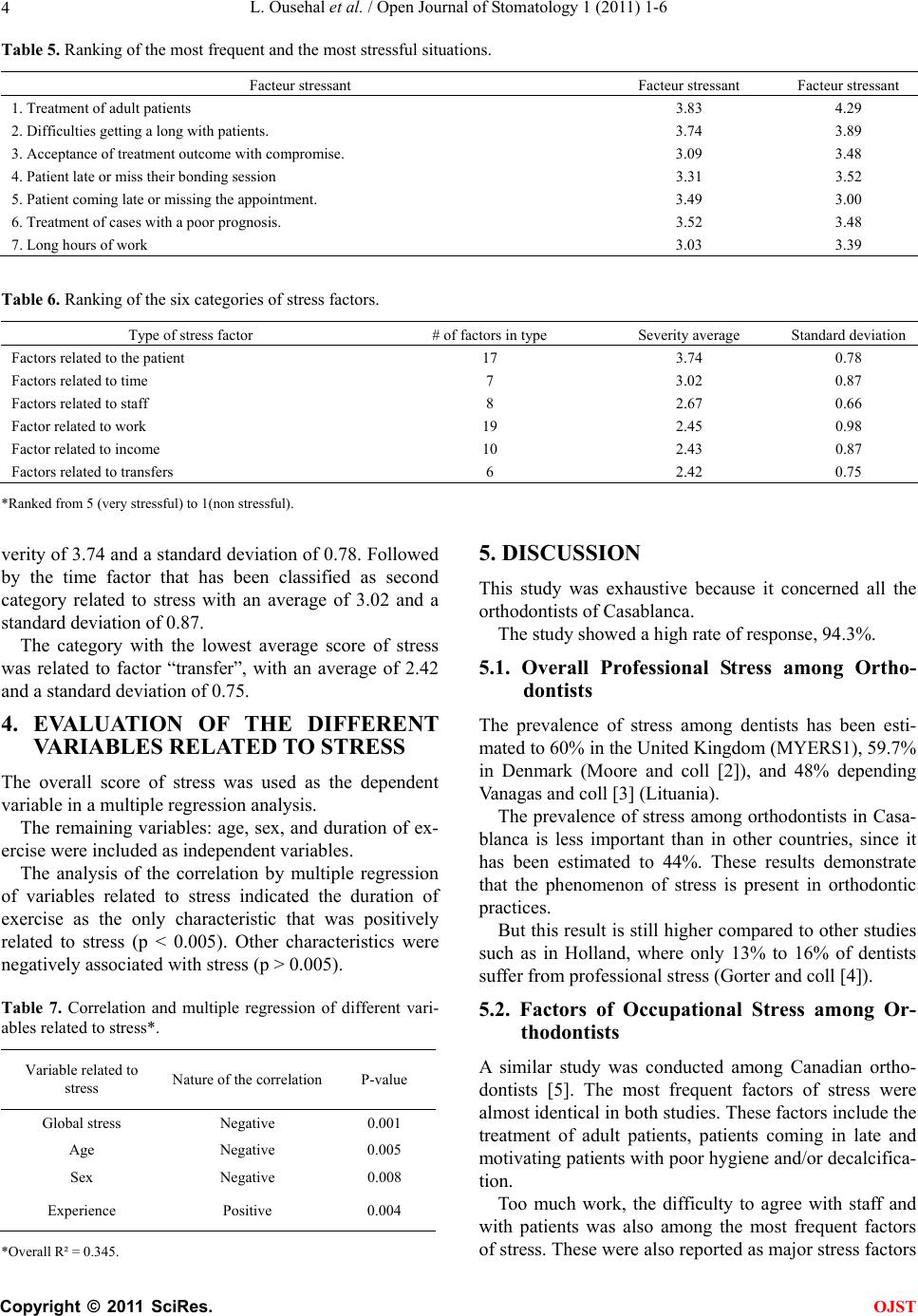
Although the difference between groups was low, analy-
sis of the scores of the six factors of stress ranked the
factor in relation to the patient first of the list, followed
by the one related to time.
A similar result was reported by numerous foreign
studies like those conducted with Lithuanian [10] and
South Korea [11] dentists.
General dentistry Doctors [10-12] also ranked these
two factors as most importa nt .
The study on Canadian orthodontists [5] revealed
similar results, and classified these two factors as the
main source of stress.
These results showed the importance of these factors
and suggest that orthodontists who want to reduce stress
should first improve their management skills with their
patients and that of time of their work.
5.4. The Role of Various Personal Characteristics
and Practice on Stress in Orthodontics
Personality and indiv idual differences are known to have
important influences on the stress response. Indeed,
marked differences were observed in response to the 66
potential stress factors. Each case was classified as “very
stressful” by at least one orthodontist and not as “stress-
ful” by at least one other. Similarly for frequency, since
facing the same situation at least two orthodontists have
responded diff erent l y.
But these influences played a larger role in the estima-
tion of stress in orthodontics, whose answers have in-
cluded almost the entire scale and have reached 90 points
on the scale of 100 points.
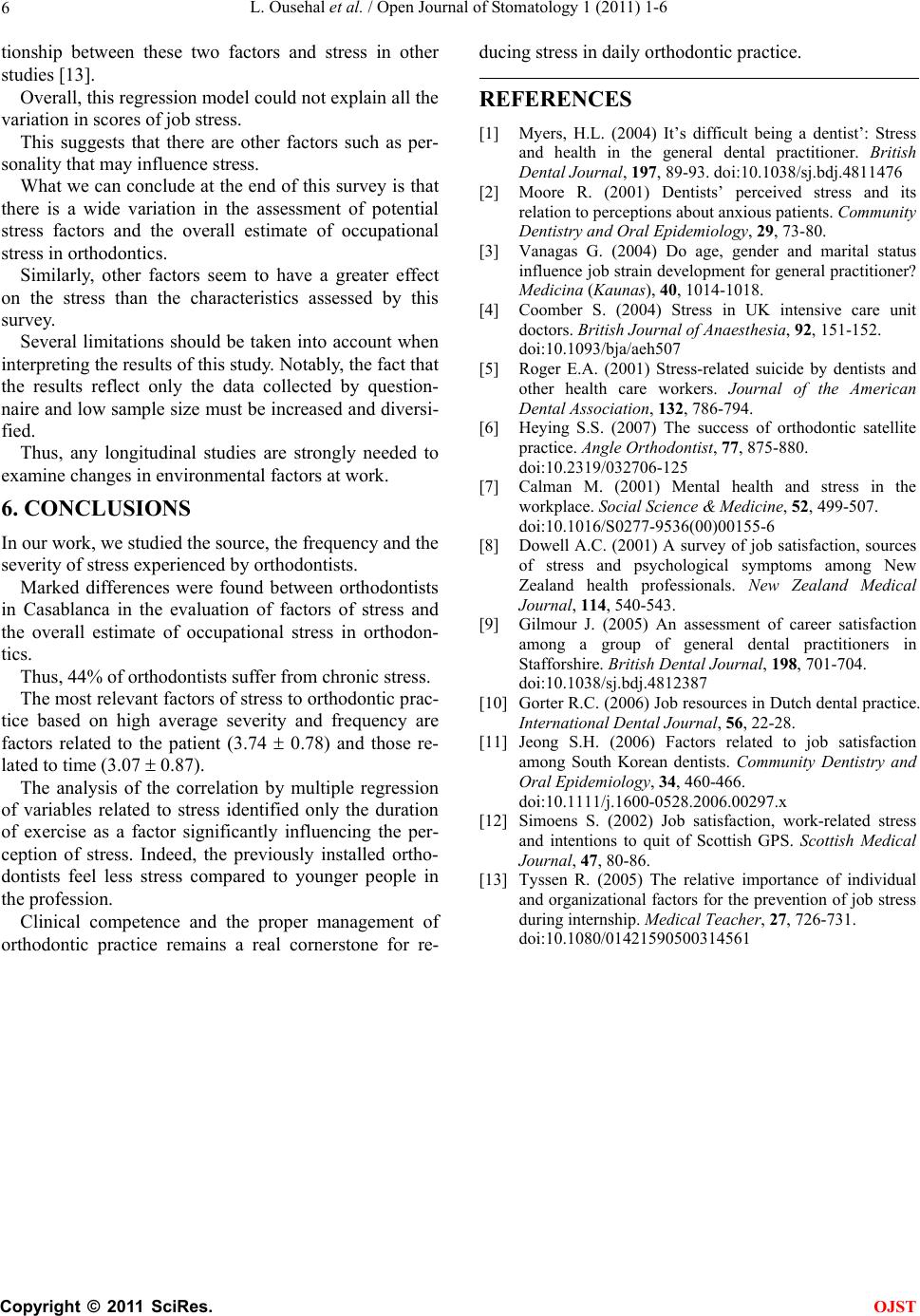
In our study, age, sex and years of practice have been
described in a final regression model to explain some of
the variation of occup a tional stress.
These characteristics have been reported as affecting
the relationship of stress in global dentistry [7] and or-
thodontics [5].
The duration of exercise was reported as the only fac-
tor significantly associated with stress according to the
regression model. This suggests that as and when the
duration of exercise increases, stress decreases.
So it is reasonable to assume that orthodontists prac-
ticing for several years become more knowledgeable and
more aware of stress, and therefore more likely to take
steps to manage it.
It is interesting that the age and sex were not signifi-
cant in our study, although there is a possible interrela-
C
opyright © 2011 SciRes. OJST