S. KREITLER ET AL.
Open Access
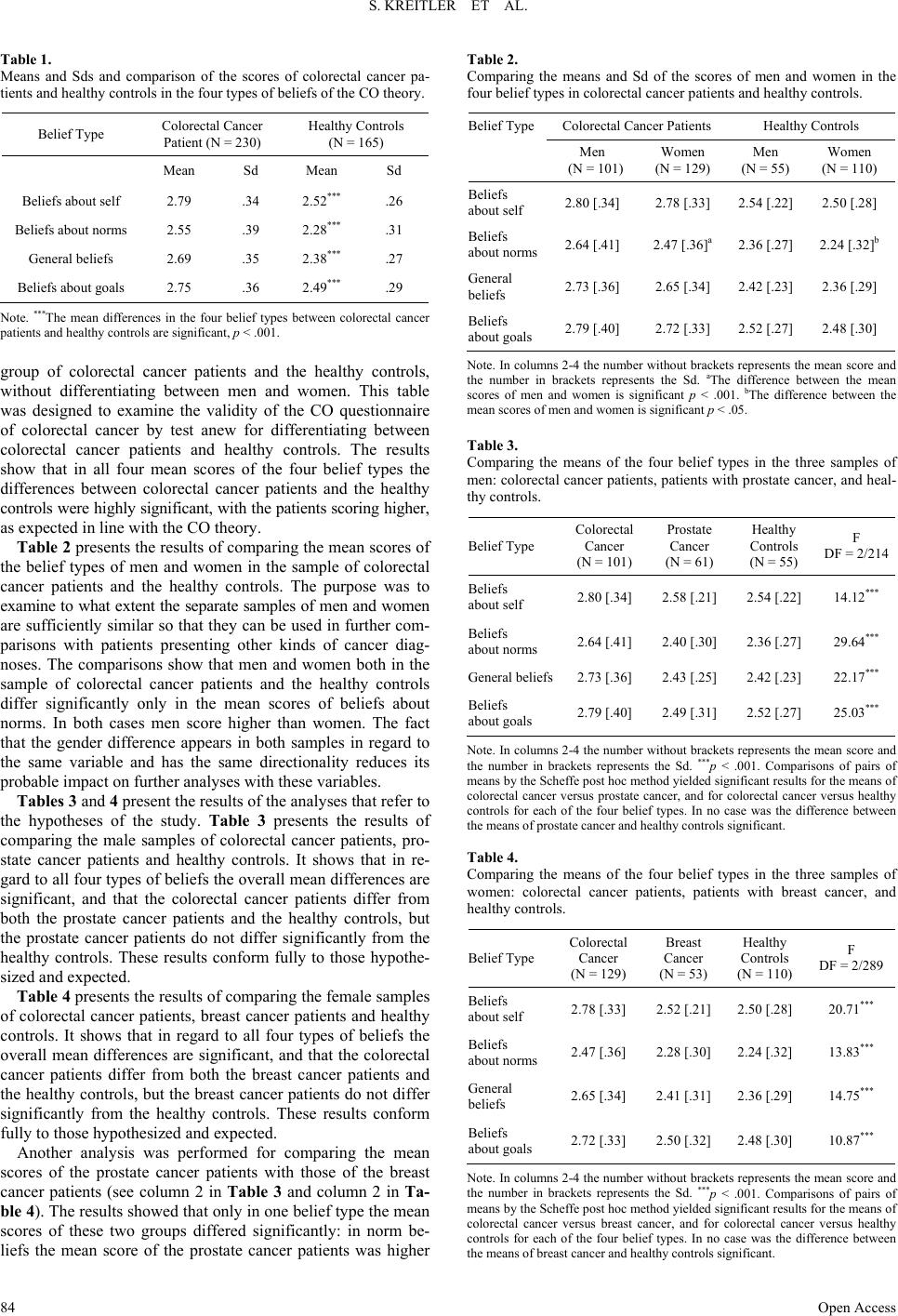
than that of the breast cancer patients (p < .01). Notably the
mean score of norm beliefs was higher for mean than for
women also in the sample of colorectal cancer patients and in
the sample of healthy controls.
Discussion
The results of the presented study show that both hypotheses
were confirmed: the CO questionnaire of colorectal cancer dif-
ferentiated the male colorectal cancer patients from the healthy
controls and prostate cancer patients, but did not differentiate
the prostate cancer patients from the healthy controls. The same
was true of breast cancer patients: the CO questionnaire of co-
lorectal cancer differentiated the female colorectal cancer pa-
tients from the healthy controls and breast cancer patients, but
did not differentiate the breast cancer patients from the healthy
controls. Further, it did not differentiate between the prostate
cancer patients and the breast cancer patients except in regard
to beliefs about norms. Hence, it may be concluded that the CO
questionnaire of colorectal cancer is specifically targeted on
colorectal cancer and differentiates patients with this diagnosis
from healthy controls and from patients with other types of
cancer but does not differentiate the other types of cancer from
healthy controls.
The findings of the study provide a sturdy proof of the speci-
ficity of the CO of disease particularly in regard to colorectal
cancer. The proof is enhanced especially through the finding
that it refers to two types of cancer—prostate cancer and breast
cancer.
A notable result is the recurrent finding that men score higher
on norm beliefs in the samples of colorectal cancer, healthy
controls and in comparing prostate cancer patients with breast
cancer. In the sample of colorectal cancer patients the finding is
in accord with the evidence that in men colorectal cancer tends
to be a more severe disease than in women (Gao et al., 2008;
Kotake et al., 2003). However, this interpretation does not hold
for the finding in the other samples. Further research is needed
to clarify the reasons for this finding.
Conclusion
The major thrust of the results is that they contribute to
strengthening the claim that psychological risk factors defined
in terms of the CO theory are disease specific. The implications
of this result are important both in regard to the better under-
standing the disease itself and in regard to enhancing the role of
psychological risk factors in the domain of medicine.
Concerning the disease, it seems justified to conclude that
there exists a profile of psychological tendencies characteristic
of colorectal cancer. Its main characteristics are that it is a pro-
file and not one or another tendency, and that the tendencies
constitute together a matrix of dynamic interactions manifesting
how the individuals experience reality, how they handle them-
selves and how they interact with others. The major focus of
their cognitive orientation concerns striving to be perfect in
performing all one’s duties, commitments and direct as well as
indirect expectations of oneself. The further focus concerns the
relation to oneself as defined in terms of the polarity of self
assertion or self effacement. The relation to others is defined in
terms of the polarity of yearning for closeness and pleasing
others contrasted with the tendency to distancing oneself from
others. The polarities denote the constant potentiality for con-
flict if both contrasting tendencies are activated at the same
time. But if however, only one tendency is activated, the indi-
vidual may feel frustrated at not having expressed oneself fully
or completely. The potential conflicts form major sources of
tension.
In view of the findings of the present study it seems appro-
priate to suggest that the identified personality tendencies could
be considered as likely candidates for psychological risk factors
for colorectal cancer. The justification for this suggestion rests
on the evidence provided by the present study about the speci-
ficity of the identified psychological tendencies as well as on
previous findings, primarily those indicating that they do not
vary with various demographic variables, such as age, country
of origin or marital status; that they are independent of various
medical variables, mainly disease stage, being in treatment or in
remission, and mainly disease duration, which could potentially
change the individual’s behavior and emotional state; and they
are readily amenable to assessment by a reliable and valid tool.
The dictionary of cancer terms prepared by the National Cancer
Institute (NCI) defines risk factors as something that may in-
crease the chance of getting a disease, for example, risk factors
for cancer include age, a family history of certain cancers, use
of tobacco products, certain eating habits, obesity, lack of exer-
cise, exposure to radiation or other cancer-causing agents, and
certain genetic changes. The identified psychological tenden-
cies grounded in the CO theory seem to fit in very well within
this framework of risk factors.
REFERENCES
Amelang, M. (1997). Using personality variables to predict cancer and
heart disease. European Journal of Per s onality, 11, 319-342.
http://dx.doi.org/10.1002/(SICI)1099-0984(199712)11:5<319::AID-
PER304>3.0.CO;2-D
Drechsler, I., Brunner, D., & Kreitler, S. (198 7). Cognitive antecedents
of coronary heart disease. Social Science and Medicine, 24, 581-588.
http://dx.doi.org/10.1016/0277-9536(87)90062-1
Denollet, J. (1998). Personality and ri sk o f cancer in men with co ronary
heart disease. Psychological Medicine, 28, 991-995.
http://dx.doi.org/10.1017/S0033291797006442
Figer, A., Kreitler, S., Kreitler, M. M. et al. (2002). Personality disposi-
tions of colon cancer patients. Gastrointestinal Oncology, 4, 81-92.
http://dx.doi.org/10.1080/1475956021000015095
Fox, B. (1998) Psychos ocial factors in cancer incidence and prognosis.
In J. Hollan d (Ed.), Psycho-oncology (pp. 110-124). New York: Ox-
ford University Press.
Gao, R. N., Neutel, C. I., & Wai, E. (2008). Gender differences in co-
lorectal cancer incidence, mortality, hospitalizations and surgical
procedures in Canada. Journal of Public Health, 30, 194-201.
http://dx.doi.org/10.1093/pubmed/fdn019
Goodkin, K., Antoni, M. H., Sevin, B., et al. (1993). A partially testable
predictive model of psychosocial factors in the etiology of cervical
cancer. I. Biological, psychological and social aspects. Psychoon-
cology, 2, 79-98. http://dx.doi.org/10.1002/pon.2960020203
Kotake, K., Honjo, S., Sug ihara, K. et al. (2003). Changes in colorectal
cancer during a 20-year period: An extended report from the mul-
ti-institutional registry of large bowel cancer, Japan. Diseases of the
Colon & Rectum, 46, S32-S43.
Kreitler, H., & Kreitler, S. (1976). Cognitive orientation and behavior.
New York: Springer Publishing.
Kreitler, H., & Kreitler, S. (1982). The theory of cognitive orientation:
Widening the scope of behavior prediction. In B. Maher, & W. B.
Maher (Eds.), Progress in experimental personality research (Vol.
11, pp. 101-169). New York: Academic Press.
Kreitler, S. (2003). Psycho-oncology. In L. M. Cohen, D. E. McChar-
gue, & F. L. Collins Jr. (Eds.), The health psychology handbook (pp.