Do Tumor Characteristics and Pre-Transplant Locoregional Therapy Predict Survival after OLT in Patients with
Hepatocellular Carcinoma?
30
mor size did not influence survival post-OLT in patients
within Milan criteria [30] compared to those who did not
have TACE.
However, these findings were not shown to be signifi-
cant on univariate analysis, probably because the sample
size was too small. Accordingly, we do not have enough
numbers of patients who survived long enough to show
any statistically significant difference.
Tumor burden and biological behavior:
We assumed that those having well differentiated HCC
might have a better outcome than those having poorly or
moderately differentiated HCC. This was based on a dif-
ferent biological behavior and a tendency to metastasize.
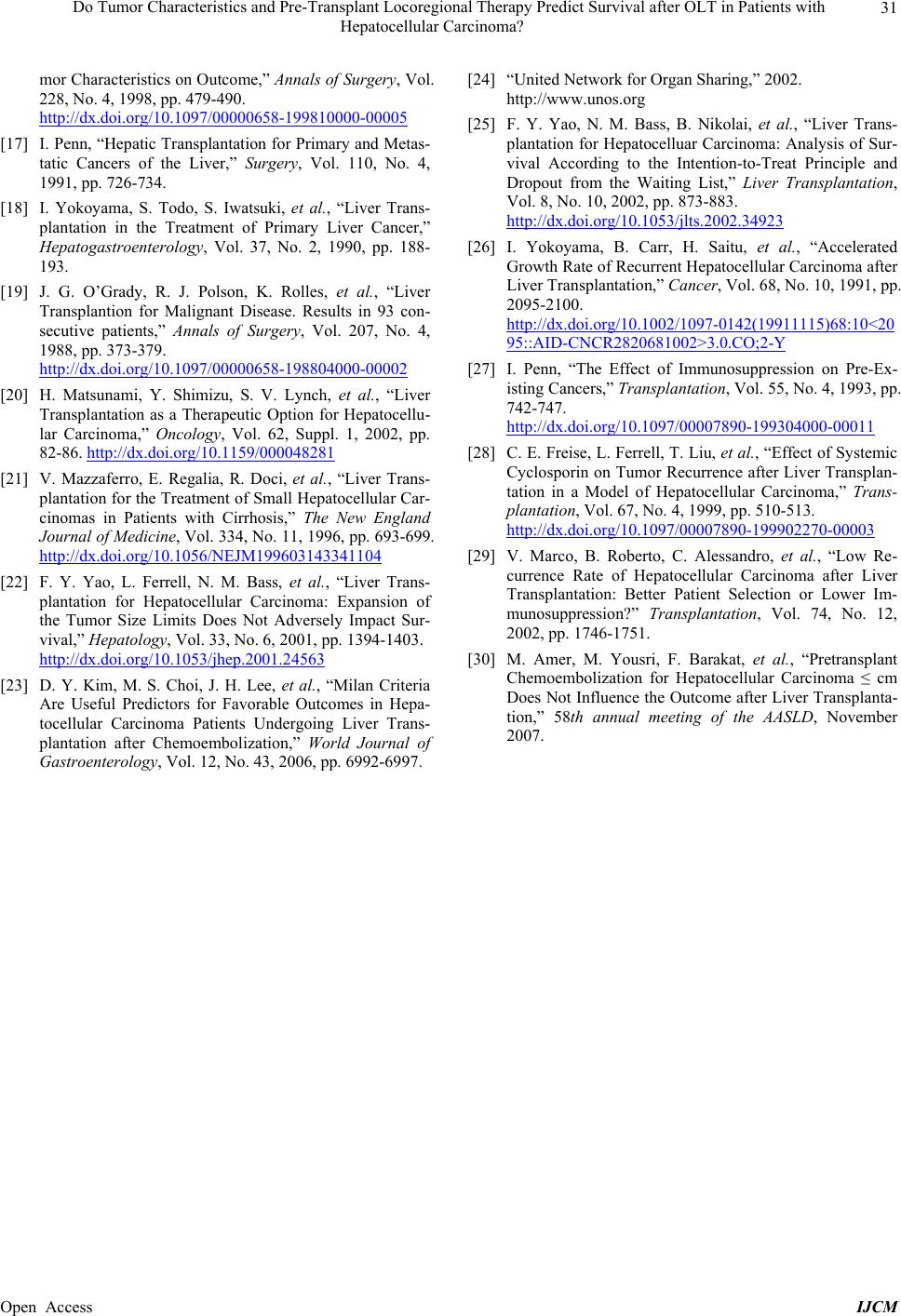
In the univariate analysis, those who had complete ne-
crosis by locoregional therapy at explant were not in-
cluded in this analysis, because the pathologist could not
determine the degree of differentiation. The group having
well differentiated HCC had a trend for better survival.
This variable needs to be studied on a larger number of
patients with longer follow-up periods using death from
metastatic HCC as an end point, excluding all other caus-
es of mortality to minimize confounding factors. As pre-
viously stated in this context, identification of the degree
of differentiation of HCC at the explant is liable to inter-
personal and even intrapersonal variations. This is a po-
tential weakness in all retrospective studies having ex-
plant specimens examined by more than one pathologist
over a relatively long duration of time.
When we tested those having complete necrosis at ex-
plant independently in univariate analysis having the
same assumption of probable better survival by decreas-
ing tumor burden, we did not find any statistically sig-
nificant difference. There was no way to make certain
whether all of this necrotic tissue was tumor tissue, or
some of the surrounding liver tissue which was acciden-
tally targeted by less selective locoregional techniques.
REFERENCES
[1] M. Shimoda, R. M. Ghobrial, I. C. Carmody, et al., “Pre-
dictors of Survival after Liver Transplantation for Hepa-
tocellualr Carcinoma Associated with Hepatitis C,” Liver
Transplantation, Vol. 10, No. 12, 2004, pp. 1478-1486.
http://dx.doi.org/10.1002/lt.20303
[2] B. Ringe, R. Pichlmayr, C. Wittekind, et al., “Surgical
Treatment of Hepatocellular Carcinoma: Experience with
Liver Resection and Transplantation in 198 Patients,”
World Journal of Surgery, Vol. 15, No. 2, 1991, pp. 270-
285. http://dx.doi.org/10.1007/BF01659064
[3] S. Iwatsuki, T. E. Starzl, D. G. Sheahan, et al., “Hepatic
Resection versus Transplantation for Hepatocellular Car-
cinoma,” Annals of Surgery, Vol. 214, No. 3, 1991, pp.
221-228.
http://dx.doi.org/10.1097/00000658-199109000-00005
[4] H. Bismuth, L. Chiche, R. Adam, et al., “Surgical Treat-
ment of Hepatocellular Carcinoma in Cirrhosis: Liver
Resection or Transplantation?” Transplantation Proceed-
ings, Vol. 25, No. 1, 1993, pp. 1066-1067.
[5] Y. Muto, H. Moriwaki, M. Ninomaya, et al., “Prevention
of Second Primary Tumors by an Acyclic Retinoid, Poly-
prenoic Acid, in Patients with Hepatocellular Carci-
noma,” The New England Journal of Medicine, Vol. 334,
No. 24, 1996, pp. 1561-1567.
http://dx.doi.org/10.1056/NEJM199606133342402
[6] W. Y. Lau, T. W. Leung, S. K. Ho, et al., “Adjuvant in-
tra-Arterial Iodine-131-Labelled Lipiodol for Respectable
hepatocellular Carcinoma: A Prospective Randomized
Trial,” Lancet, Vol. 353, No. 9155, 1999, pp. 797-801.
http://dx.doi.org/10.1016/S0140-6736(98)06475-7
[7] J. M. Llovet, J. Fuster and J. Bruix, “Intention-to-Treat
Analysis of Surgical Treatment for Early Carcinoma: Re-
section versus Transplantation,” Hepatology, Vol. 30, No.
6, 1999, pp. 1434-1440.
http://dx.doi.org/10.1002/hep.510300629
[8] Z. Y. Tang, Y. Q. Yu and X. D. Zhou, “Evolution of Sur-
gery in the Treatment of Hepatocellular Carcinoma from
the 1950s to the 1990s,” Seminars in Surgical Oncology,
Vol. 9, No. 4, 1993, pp. 293-297.
http://dx.doi.org/10.1002/ssu.2980090403
[9] M. Makuuchi, “Surgical Management for Hepatocellular
Carcinoma,” In: V. Arroyo, J. Bosch and J. Rodēs, Eds.,
Treatments in Hepatology, Barcelona, Masson, Vol. 1995,
pp. 341-352.
[10] The Liver Cancer Study Group of Japan, “Predictive Fac-
tors for Long Term Prognosis after Partial Hepatectomy
for Patients with Hepatocellular Carcinoma in Japan,”
Cancer, Vol. 74, No. 10, 1994, pp. 2772-2780.
http://dx.doi.org/10.1002/1097-0142(19941115)74:10<27
72::AID-CNCR2820741006>3.0.CO;2-V
[11] B. Ringe, R. Pichlmyar, C. Wittekind, et al., “Surgical
Treatment of Hepatocellular Carcinoma: Experience with
Liver Resection and Transplantation in 198 Patients,”
World Journal of Surgery, Vol. 15, No. 2, 1991, pp.
270-285. http://dx.doi.org/10.1007/BF01659064
[12] P. Moreno, E. Jaurrieta, J. Figueras, et al., “Orthotopic
Liver Transplantation: Treatment of Choice in Cirrhotic
Patients with Hepatocellular Carcinoma?” Transplanta-
tion Proceedings, Vol. 27, No. 4, 1995, pp. 2296-2298.
[13] H. Bismuth, L. Chiche, R. Adam, et al., “Liver Resection
versus Transplantation for Hepatocellular Carcinoma in
Cirrhotic Patients,” Annals of Surgery, Vol. 218, No. 2,
1993, pp. 145-151.
http://dx.doi.org/10.1097/00000658-199308000-00005
[14] D. G. Farmer, M. H. Rosove, A. Shaked, et al., “Current
Treatment Modalities for Hepatocellular Carcinoma,”
Annals of Surgery, Vol. 219, No. 3, 1994, pp. 236-247.
http://dx.doi.org/10.1097/00000658-199403000-00003
[15] H. Bismuth, P. E. Majno and R. Adam, “Liver Trans-
plantation for Hepatocelluar Carcinoma,” Seminars in
Liver Disease, Vol. 19, No. 3, 1999, pp. 311-322.
http://dx.doi.org/10.1055/s-2007-1007120
[16] G. B. Kliontmalm, “Liver Transplantation for Hepatocel-
lular Carcinoma: A Registry Report of the Impact of Tu-
Open Access IJCM