F. A. Andoulo et al. / Open Journal of Gastroenterology 3 (2013) 323-327
326
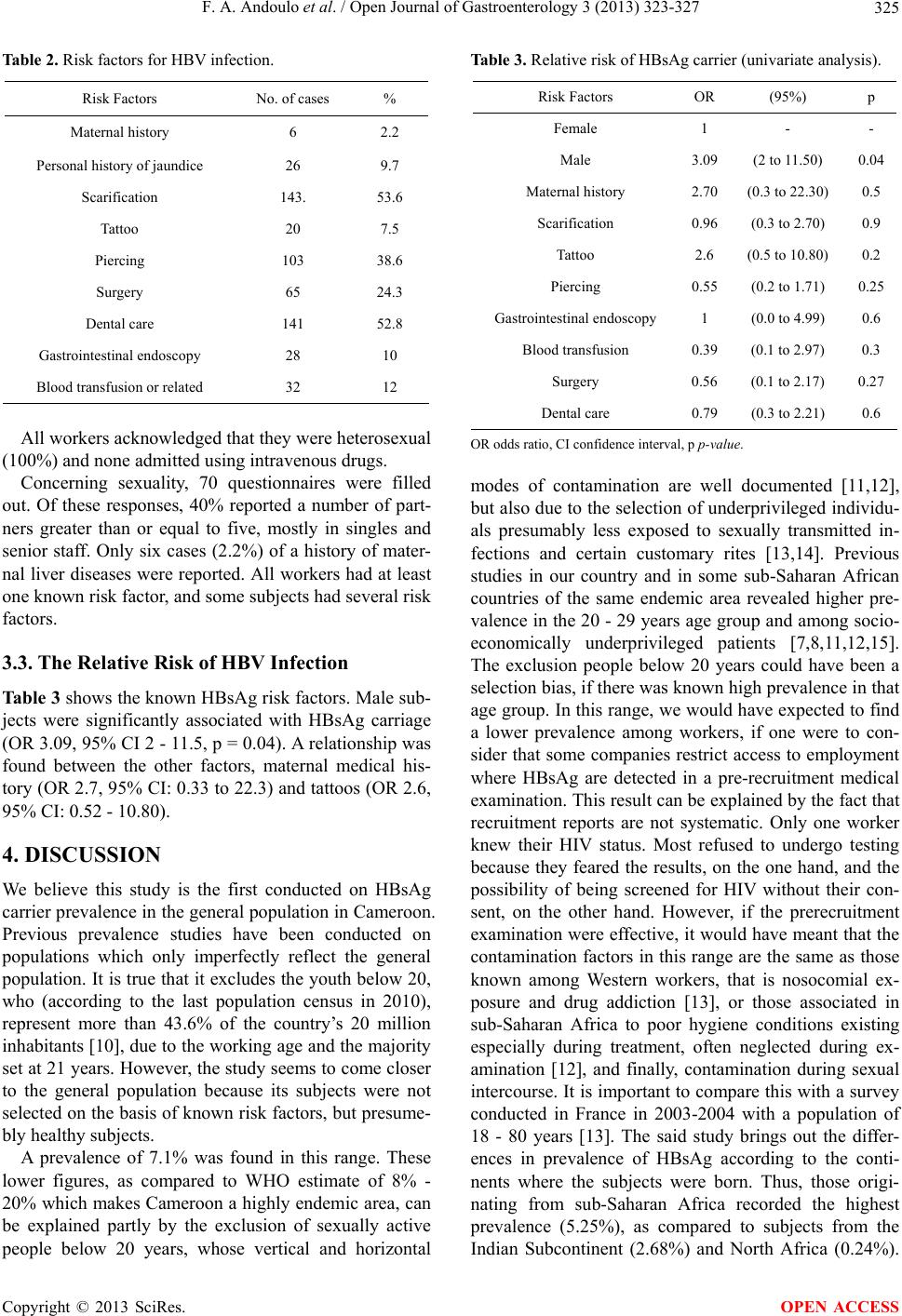
Specific risk factors such as nosocomial exposure, cer-
tain rituals (scarification, tattoos...), sex with multiple
sexual partners and the socio-economic class were dis-
cussed in the study. All things being equal, the persis-
tence of a high prevalence among subjects from sub-
Saharan Africa, compared to other groups, shows that the
neo- and perinatal infection is very high in the sub-Sa-
haran Africa region [15-18]. This neo- and perinatal in-
fection is emphasized in the study carried out by Bigot et
al. in Benin [11], in which eight children from 40 HBV
seropositive mothers (20%) tested positive for HBsAg,
and in the study carried out by Lohouès-Kouacou et al.
in Côte d’Ivoire [19], where the incidence of perinatal
transmission was estimated at 32.8%.
One of the most important observations in our study
was the fact that all workers admitted that they were het-
erosexual. The fact that subjects do not admit to risky
sexual behavior, if any, is well-documented [20,21].
In Sub-Saharan Africa, the prevalence is generally
high. Senegal (17%) [22], Ivory Coast (18.2%) [15],
Madagascar (23%) [18] and Mali (24.9%) [5] are coun-
tries with a high level of HBV infection prevalence.
Cameroon’s prevalence rate is similar to that of countries
such as Benin (8.26%) [11] and the Democratic Republic
of Congo (DRC) (9.2%) [9]. Reunion has a low preva-
lence rate of 0.7%, which is close to that of Metropolitan
France, probably due to a better economy and better
health condition s [12,13 ].
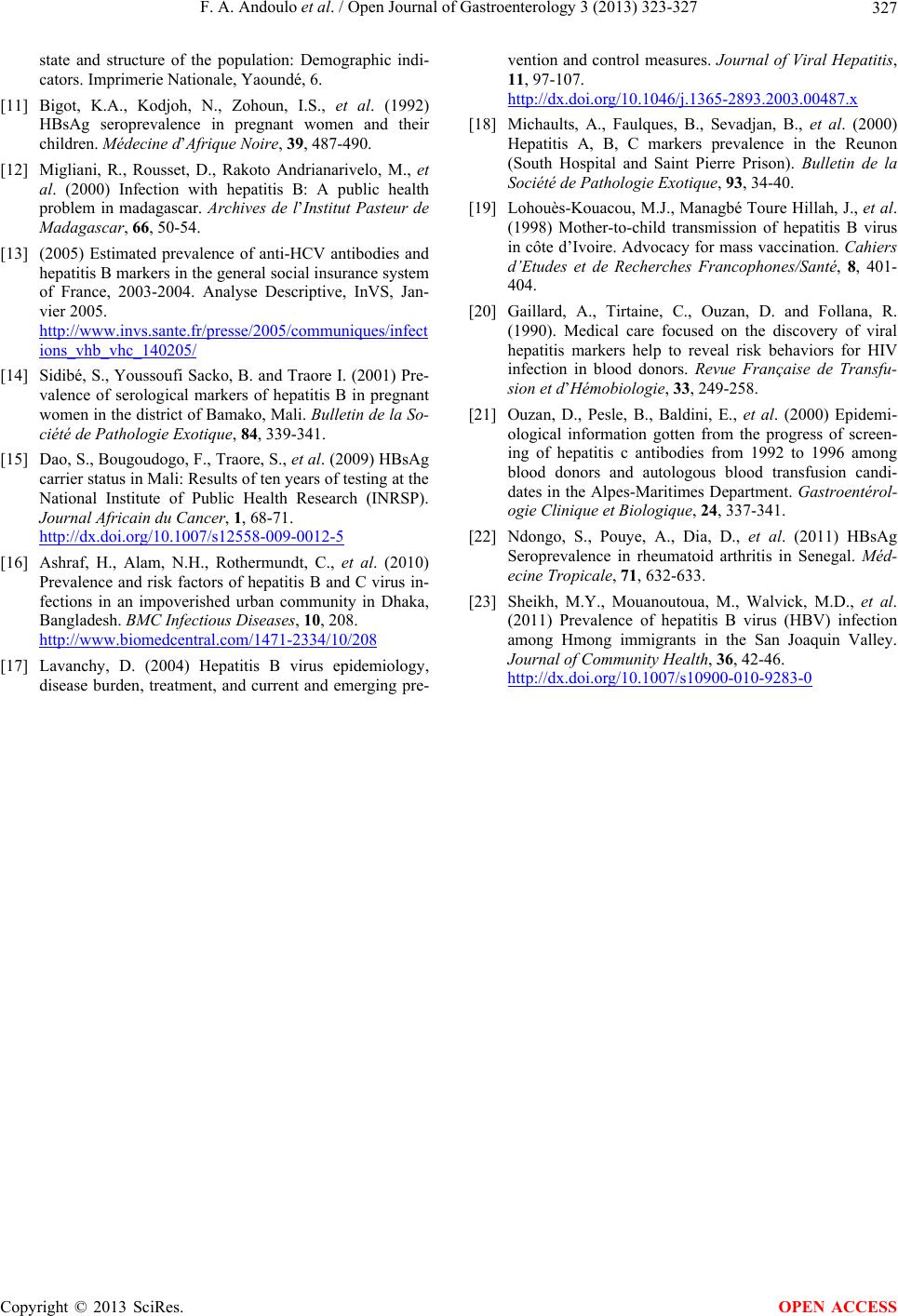
Men were three times more likely to be HBsAg carri-
ers than women. This result tallies with that of other
studies conducted in Cameroon [7 ,8] and in the literature
[2,9,13,15].
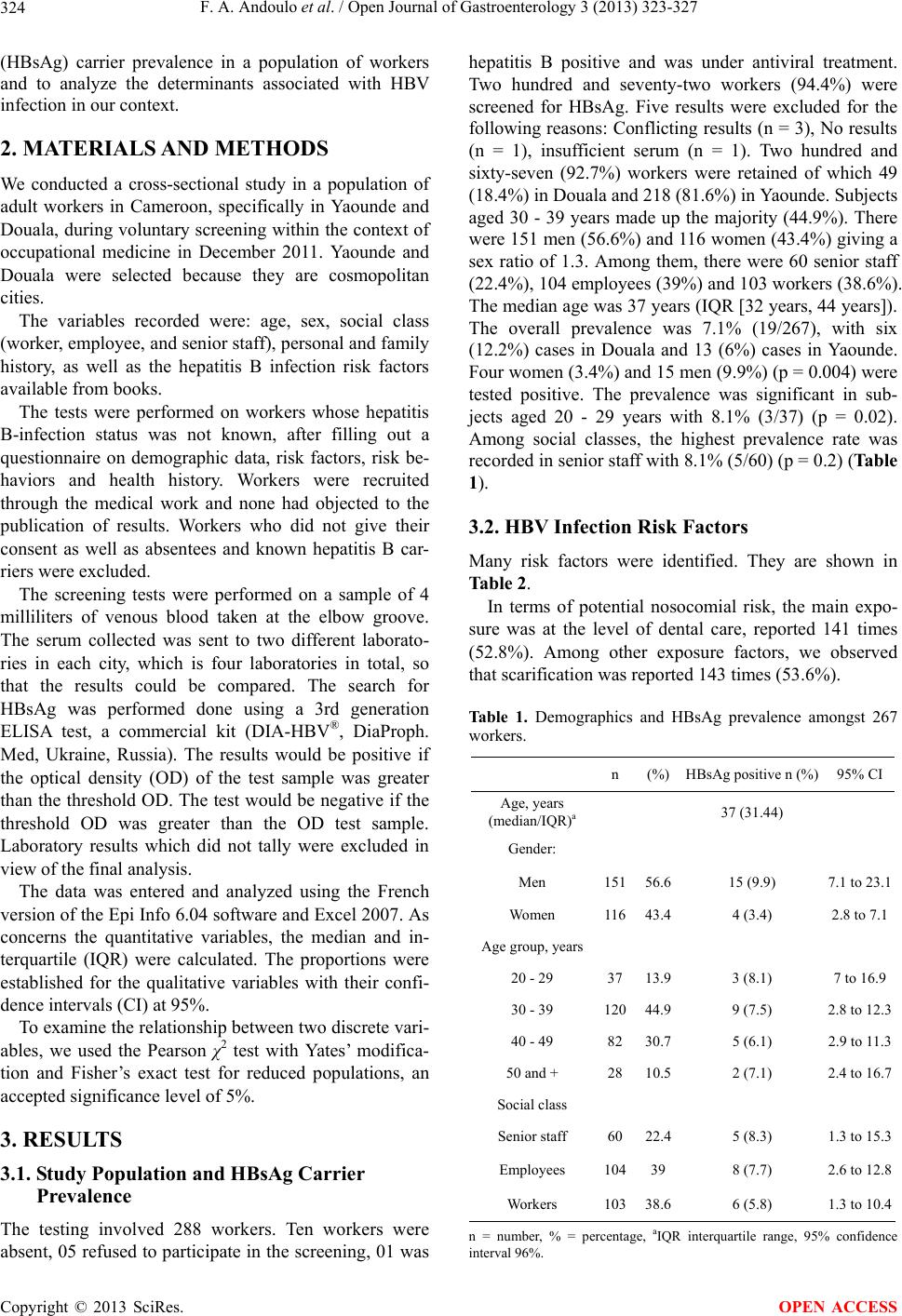
The majority of workers with HBsAg were in the 20 -
29 year s age group. This age-related result is iden tical to
the previous study by Koanga Mogtomo et al. conducted
in our country [7]. Conversely, in mainland France [13],
as well as in DRC [9] and among United States immi-
grants [23], the 30 - 39 year age group that is that most
affected. The difference with the study conducted in the
DRC is at the level of the selection of the sample. The
difference with that carried out in mainland France is
explained by the means of contamination.
The relationship between HBsAg prevalence and low
socio-economic levels has been treated by other authors
[11,13-15]. Our results did not tally with theirs. This is
probably due to the social ascension of individuals from
underprivileged backgrounds and the fact that senior
staff had several sex partners.
The difference in the prevalence rate between Douala
(12.2%) and Yaounde (6%) supports th e idea that there is
a huge difference in infection patterns according to re-
gion, according to socio-economic status, and according
to hygiene, in the same city. This result is similar to that
obtained in the study by Mbendi Nlombi et al. in eastern
Kinshasa in DRC [9].
5. CONCLUSION
Our study shows a significant HBsAg carrier prevalence
in a population of workers close to the general popula-
tion in Cameroon, particularly among young people un-
der 30 years, in men and in Douala. It is not different
from that of the population of blood donors, which tends
to confirm the hypothesis of the existence of neo-Peri-
natal infection in our country. This result clearly high-
ghts the importance of strategies for vaccinating new-
borns and those for the treatment of pregnant women
who are chronic carriers of HBsAg in controlling the
risks of HBV c ont amination.
6. ACKNOWLEDGEMENTS
Hoffmann-La Roche Ltd. Cameroon Branch. Avenue De Gaulle, Rue
Noury. P.O. Box 8 71 Do ua la-Bonapriso, Cameroon.
REFERENCES
[1] Liang, T.J. (2009) Hepatitis B: The virus and disease.
Hepatology, 49, S13-S21.
http://dx.doi.org/10.1002/hep.22881
[2] Lin, S.Y., Chang, E.T. and So, S.K. (2007) Why we
should routinely screen Asian American adults for heap-
titis B: A cross-sectional study of Asians in California.
Hepatology, 46, 1034-1040.
http://dx.doi.org/10.1002/hep.21784
[3] (2012) Hepatitis B vaccine.
www.who.int/vaccines/en/hepatitisb.shtml
[4] Sharma, S.K., Saini, N. and Chwla, Y. (2005) Hepatitis B
virus: Inactive carriers. Virology Journal, 2, 82.
http://www.virologyj.com/content/2/1/82
[5] Dény, P. and Zoulim, F. (2010) Hepatitis B virus: From
diagnosis to treatment. Pathologie Biologie, 58, 245-253.
http://dx.doi.org/10.1016/j.patbio.2010.05.002
[6] Nwokediuko, S.C. (2011) Chronic hepatitis B: Manage-
ment challenges in resource-poor countries. Hepatitis
Monthly, 11, 786-793.
[7] Koanga Mogtomo, M.L., Louandji Fomekong, S., Fotso
Kuate, H. and Ngono Ngane, A. (2009) Detection of
infectious agents in blood banks in Douala (1995-2004).
Cahiers d’Etudes et de Recherches Francophones/Santé,
19, 3-8.
[8] Zekeng, L. and Kaptue, L. (1990) HIV 1 serology and
HBsAg and HBeAg carrier status in blood donors at the
Yaounde University Hospital, Cameroon. Annales de la
Société Belge de Médecine Tropicale, 70, 49-53.
[9] Mbendi Nlombi, C., Longo-Mbenza, B. Mbendi Nsukimi,
S., et al. (2001) HIV and HBsAg prevalence in blood
donors. Residual contamination risk in blood recipients in
east Kinshasa, Democratic Republic of Congo. Médecine
Tropicale, 61, 139-142.
[10] National Institute of Statistics of Cameroon (2010) The
Copyright © 2013 SciRes. OPEN ACCESS