S. Abuzinada, F. Alsulaimani / Open Journal of Stomatology 3 (2013) 515-519
518
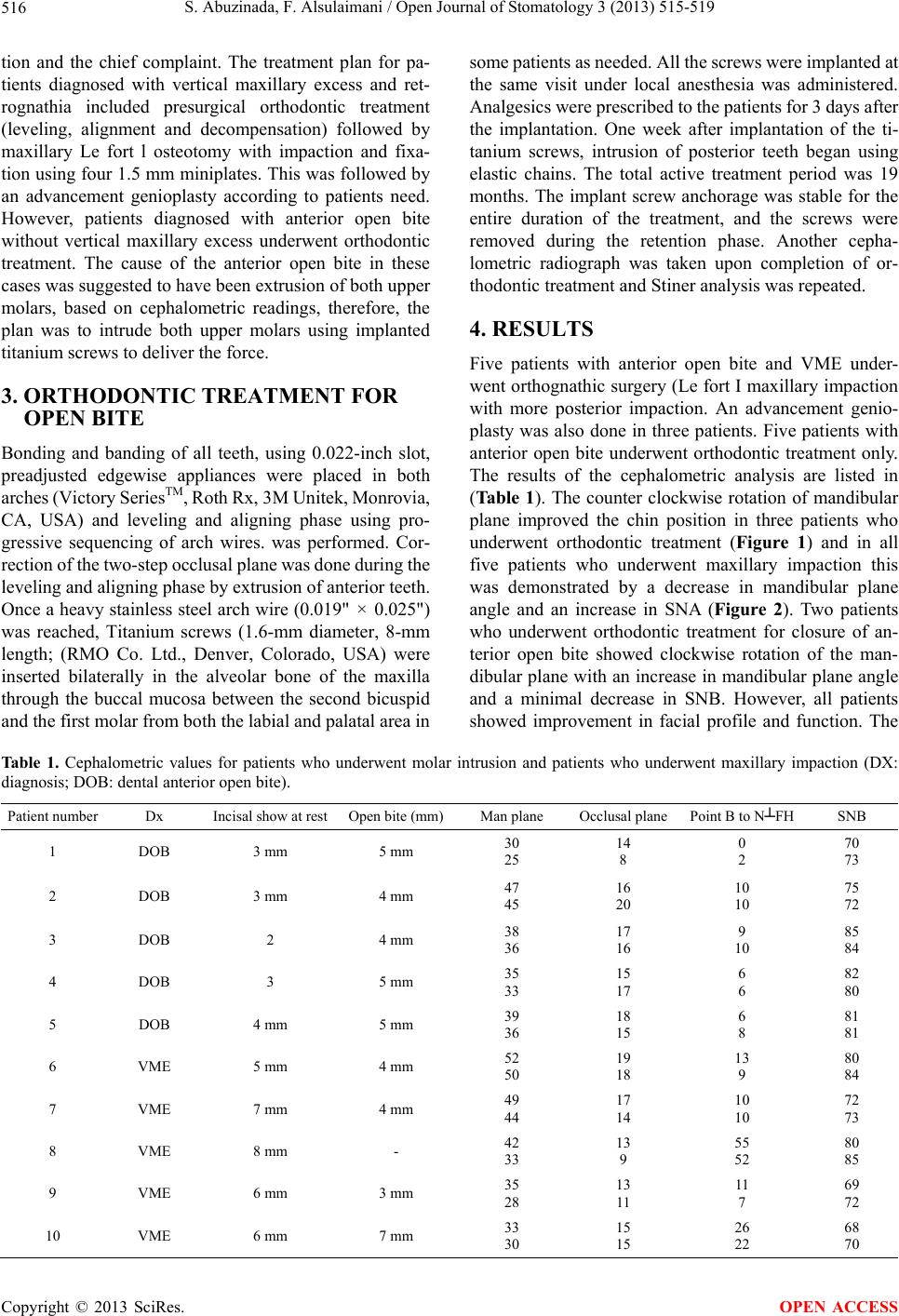
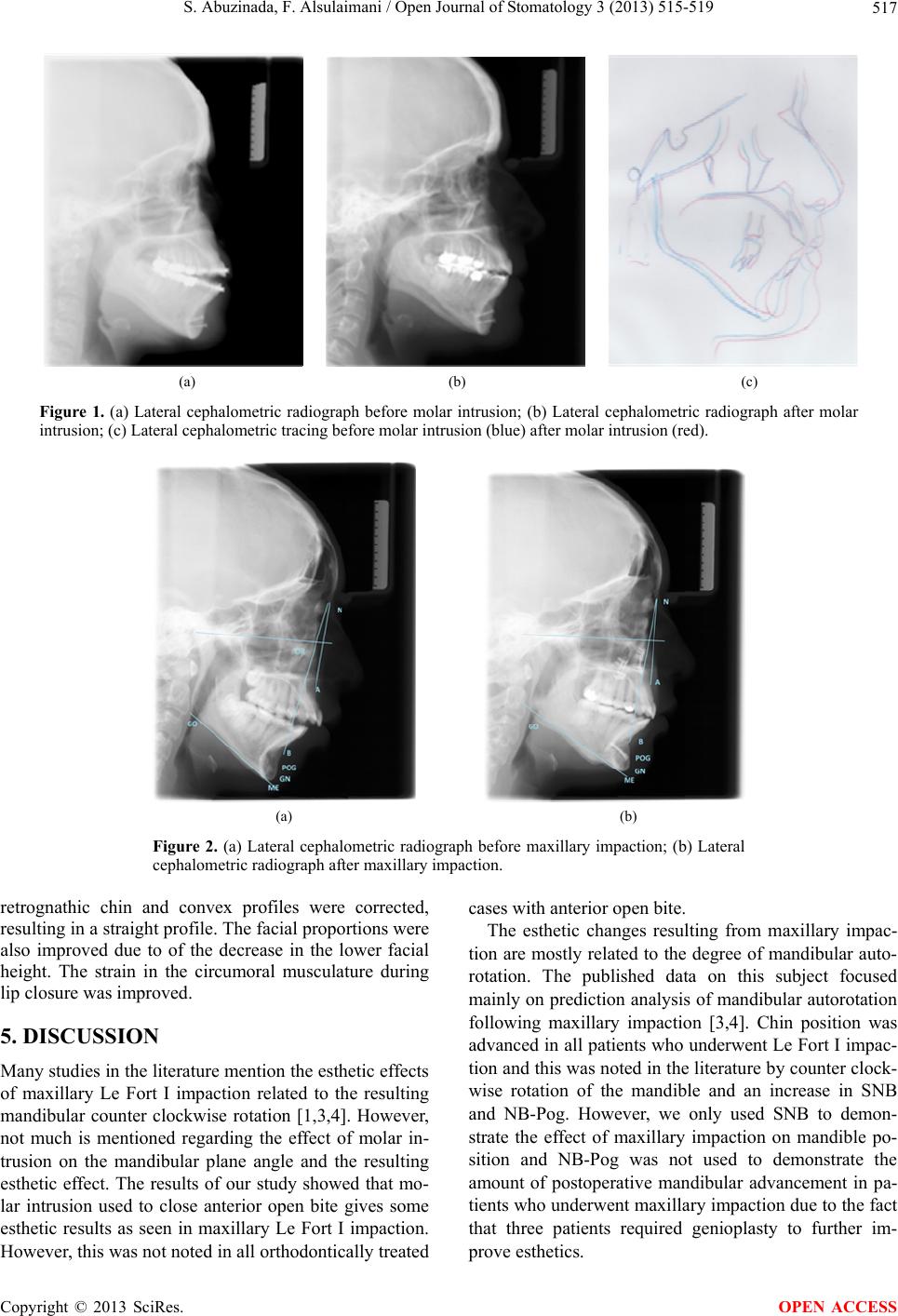
Patients who underwent orthodontic treatment for
open bite closure showed improved esthetics, however,
not all patients showed mandibular counter clockwise
rotation as seen in Le Fort I impaction. Some patients
showed clockwise mandibular rotation. This was ex-
plained by the orthodontic treatment, since two of the
patients have constricted maxilla. Expansion appliance
such as Quad-Helix was used to expand the maxillary
teeth. It is well documented with expansion clock wise
rotation of the mandibular plane which has taken place
due to extrusion of the palatal cusp. The clock wise rota-
tion point pog will also rotate backward. The difference
between pre and post treatment was in average 2 degrees
which could be due to the occlusal plane measured at
functional occlusion with no anterior teeth contacting a
measurement error that was possible. The most important
is the reduction of the mandibular plane which showed a
counter clock wise rotation in all the patients with es-
thetic improvement.
On the other hand, the skeletal improvement is poor
due to failure to establish absolute anchorage during mo-
lar intrusion. To obtain absolute anchorage, several de-
vises have been used such as dental implant [11-14],
screws [15,16] and miniplates [17,18]. The advantages of
these devices are by providing absolute anchorage dif-
ferent teeth movement without the need for patient’s co-
operation. Several reports have been reported on the use
of screw for anchorage in teeth movement, intrusion or
retraction of anterior teeth [10,11], and protraction of
posterior teeth in the mandible. In addition, few papers
have reported the use of titanium screws for orthodontic
anchorage to intrude upper and/or lower molars of an
adult patient with severe skeletal anterior open bite.
The mandible will follow any changes in occlusion
resulting from maxillary impaction or molar intrusion.
The noted changes in mandibular and chin position were
quite variable and less predictable following molar intru-
sion, however, the improved esthetics can be appreciated
in all patients. Future standardized studies will help us
make accurate predictions following molar intrusion or
maxillary impaction.
REFERENCES
[1] Schendel, S., Eisenfeld, J., Bell, W., et al. (1976) Supe-
rior repositioning of the maxilla: stability and soft tissue
osseous relations. American Journal of Orthodontics, 70,
663-674.
http://dx.doi.org/10.1016/0002-9416(76)90226-8
[2] Sherwood, K. (2007) Correction of skeletal open bite
with implant anchored molar/bicuspid intrusion. Oral &
Maxillofacial Surgery Clinics of North America, 19, 339-
350. http://dx.doi.org/10.1016/0002-9416(76)90226-8
[3] Nadjmi, N., Mommaerts, M., Abeloos, J. and Clercq, C.
(1998) Prediction of mandibular autorotation. Journal of
Oral and Maxillofacial Surgery, 56, 1241-1247.
http://dx.doi.org/10.1016/S0278-2391(98)90599-7
[4] Y.-C. Wang, Ko, E.W.-C., Huang, C.-S. and Chen, Y.-R.
(2006) The inter-relationship between mandibular auto-
rotation and maxillary LeFort I impaction osteotomies.
Journal of Craniofacial Surgery, 17, 898-904.
http://dx.doi.org/10.1097/01.scs.0000234985.99863.97
[5] Sperry, T.P., Steinberg, M.J. and Gans, B.J. (1982) Man-
dibular movement during autorotation as a result of max-
illary impaction surgery. American Journal of Orthodon-
tics, 81, 116-123.
http://dx.doi.org/10.1016/0002-9416(82)90035-5
[6] Bryan, D.C. (1994) An investigation into the accuracy
and validity of three points used in the assessment of
autorotation in orthognathic surgery. British Journal of
Oral and Maxillofacial Surgery, 32, 363-272.
http://dx.doi.org/10.1016/0266-4356(94)90026-4
[7] Nattestad, A. and Vedtofte, P. (1992) Mandibular autoro-
tation in orthognathic surgery: A new method of locating
the centre of mandibular rotation and determining its
consequence in orthognathic surgery. Journal of Cranio-
facial Surgery, 20, 163-170.
[8] Rekow, E.D., Speidel, T.M. and Koening, R.A. (1993)
Location of the mandibular center of autorotation in max-
illary impaction surgery. American Journal of Orthodon-
tics and Dentofacial Orthopedics, 103, 530-536.
http://dx.doi.org/10.1016/0889-5406(93)70093-4
[9] Wang, Y., Ko, E., Huang, C. and Chen, Y. (2006) The
inter-relationship between mandibular autorotation and
maxillary LeFort I impaction osteotomies. Journal of
Craniofacial Surgery, 17, 898-904.
http://dx.doi.org/10.1097/01.scs.0000234985.99863.97
[10] Alsulaimani, F. (2012) Severe anterior open-bite case
treated using miniscrew anchorage: A case report. Jour-
nal of American Science, 8, 102-107.
[11] Turley, P.K., Kean, C., Schur, J., Stefanac, J., Gray, J.,
Hennes, J. and Poon, L.C. (1988) Orthodontic force ap-
plication to titanium endosseous implants. Angle Ortho-
dontist, 58, 151-162.
[12] Odman, J., Lekholm, U., Jemt, T., Branemark, P.I. and
Thilander, B. (1988) Osseointegrated titanium implants—
A new approach in orthodontic treatment. European
Journal of Orthodontics, 10, 98-105.
http://dx.doi.org/10.1093/ejo/10.2.98
[13] Prosterman, B., Prosterman, L., Fisher, R. and Gornitsky,
M. (1995) The use of implants for orthodontic correction
of an open bite. American Journal of Orthodontics and
Dentofacial Orthopedics, 107, 245-250.
http://dx.doi.org/10.1016/S0889-5406(95)70139-7
[14] Roberts, W.E., Helm, F.R., Marshall, K.J. and Gongloff,
R.K. (1989) Rigid endosseous implants for orthodontic
and orthopedic anchorage. Angle Orthodontist, 59, 247-
256.
[15] Creekmore, T.D. and Eklund, M.K. (1983) The possibil-
ity of skeletal anchorage. Journal of Clinical Orthodon-
tics, 17, 266-269.
[16] Costa, A., Raffainl, M. and Melsen, B. (1998) Mini-
screws as orthodontic anchorage: A preliminary report.
Copyright © 2013 SciRes. OPEN ACCESS