 Open Journal of Stomatology, 2013, 3, 59-64 OJST http://dx.doi.org/10.4236/ojst.2013.39A009 Published Online December 2013 (http://www.scirp.org/journal/ojst/) Oral health status and performance of oral functions in children and adolescents in the treatment for overweight or obesity Maria Ívina Gomes Janoca, Manoel de Oliveira Dantas Filho, Fernando Henrique Pereira de Vasconcelos, Armiliana Soares Nascimento, Rosa Maria Mariz de Melo Sales Marmhoud Coury, Criseuda Maria Benício Barros, Silvio Romero do Nascimento, Luciana de Barros Correia Fontes* Rua Ester Foigel, 110, ap. 1102, Ed. Victor Rodrigues, Iputinga, Recife, Pernambuco, Brasil Email: *lu.bc.f@hotmail.com Received 25 October 2013; revised 3 December 2013; accepted 21 December 2013 Copyright © 2013 Maria Ívina Gomes Janoca et al. This is an open access article distributed under the Creative Commons Attribu- tion License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT The objective of this study was to evaluate the per- formance of oral functions and oral conditions in children and adolescents with overweight or obesity, investigating possible associations with treatment for weight reduction. Developing a cross-sectional re- search and quantitative approach with inductive and descriptive and critical analysis of data, such as from a range of 95%, the universe was represented by children and adolescents who were overweight or ob ese, in both sexes, treated at reference cente rs f or the treat - ment of obesity by the National Health System, in Campina Grande, Paraíba, 2010-2012. As the con- tro l gr oup considered subjects of the same age, in the process of screening for attention in the places listed, but without the condition of overweight or obese, the research was started after the approval by the Ethics Resarch Committee of the UEPB under the protocol number 0513.0.133.000-09. As instruments for data collection were used in the questionnaire and clinical examination, of the 70 surveyed, most were female, ranging in age from 3 to 17 years, overweight, with- out comorbidities and carriers of deleterious oral habits; especially the nail biting, significantly associ- ated with female sex p < 0.05. Consistency was the preferred food paste and chewing quickly, unilater- ally, without discomfort or gagging constant. There was a significant difference between the values of the DMFT index, the presence of visible biofilm and the frequency of halitosis, for groups with overweight or obe sit y, w i t h asso ciation between time of treatment and medications. Keywords: Stomatognathic System; Oral Health; Overweight; Obesity; Comprehensive Health Care of Children and Adolescents; Pediatric Dentistry 1. INTRODUCTION Obesity is a serious public health problem worldwide due to the increase in its incidence and prevalence rates, the notorious impairment of a population increasingly young (particularly juvenile) and possible implications on life quality of affected individuals and their care needs. Brazil is passing through the nutritional transition pe- riod, where malnutrition is giving way to overweight and obesity as a nutritional disorder is most prevalent in vir- tually all strata of population; evidencing polarization in regions with high poverty levels, such as the northeast of the country [1]. This situation is characterized by abnormal accumula- tion of body fat compared with body size. Usually, the Body Mass Index or BMI (kg/m2) is overall used for the body weight assessment. This should be linked to other parameters in order to identify the risk conditions to health, particularly in children and adolescents. The lev- els related to the problem vary from the overweight or pre-obesity, with BMI between 25 and 29.9, obesity class I from 30 to 34.9, obesity class II from 35 to 39.9 and obesity class III, also called morbid obesity over 40 [2]. The treatment of obesity is difficult due to its multi- factorial etiology resulting from the complex interaction of environmental, genetic and psychological factors, as- suming different clinical situations to individuals in dif- ferent socioeconomic realities. In th is context, p r even tio n *Corresponding a uthor. OPEN ACCESS 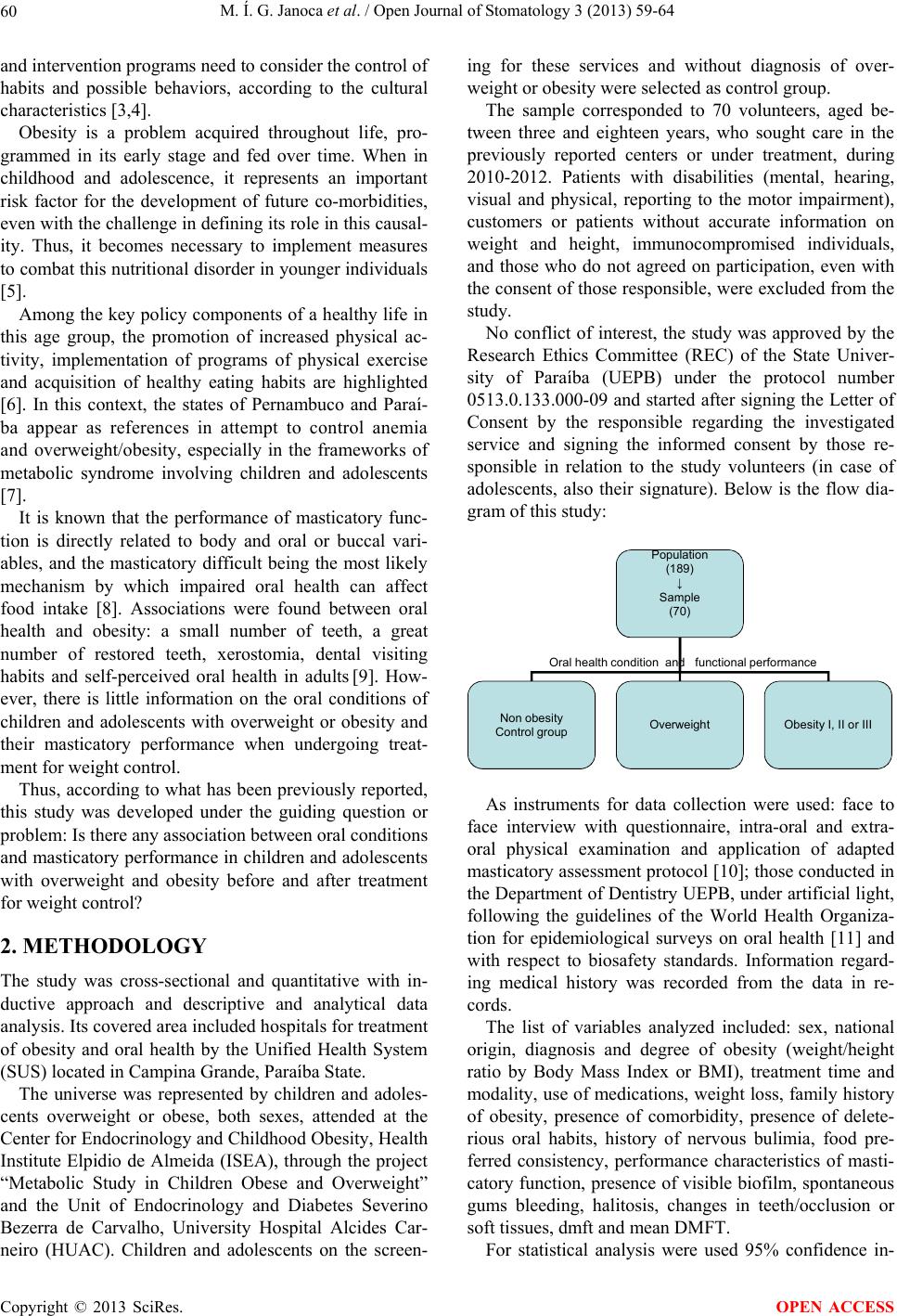 M. Í. G. Janoca et al. / Open Journal of Stomatology 3 (2013) 59-64 60 and intervention programs need to consid er the co ntro l of habits and possible behaviors, according to the cultural characteristics [3,4]. Obesity is a problem acquired throughout life, pro- grammed in its early stage and fed over time. When in childhood and adolescence, it represents an important risk factor for the development of future co-morbidities, even with the challenge in definin g its role in this causal- ity. Thus, it becomes necessary to implement measures to combat this nutrition al disorder in younger indiv iduals [5]. Among the key policy components of a healthy life in this age group, the promotion of increased physical ac- tivity, implementation of programs of physical exercise and acquisition of healthy eating habits are highlighted [6]. In this context, the states of Pernambuco and Paraí- ba appear as references in attempt to control anemia and overweight/obesity, especially in the frameworks of metabolic syndrome involving children and adolescents [7]. It is known that the performance of masticatory func- tion is directly related to body and oral or buccal vari- ables, and the masticatory difficult being the most likely mechanism by which impaired oral health can affect food intake [8]. Associations were found between oral health and obesity: a small number of teeth, a great number of restored teeth, xerostomia, dental visiting habits and self-perceived oral health in adults [9]. How- ever, there is little information on the oral conditions of children and adolescents with overweight or obesity and their masticatory performance when undergoing treat- ment for weight control. Thus, according to what has been previously reported, this study was developed under the guiding question or problem: Is there any association between oral conditions and masticatory performance in children and adolescents with overweight and obesity before and after treatment for weight control? 2. METHODOLOGY The study was cross-sectional and quantitative with in- ductive approach and descriptive and analytical data analysis. Its covered area included hospitals for treatment of obesity and oral health by the Unified Health System (SUS) located in Campina Grande, Paraíba State. The universe was represented by children and adoles- cents overweight or obese, both sexes, attended at the Center for Endocrinology and Childhood Obesity, Health Institute Elpidio de Almeida (ISEA), through the project “Metabolic Study in Children Obese and Overweight” and the Unit of Endocrinology and Diabetes Severino Bezerra de Carvalho, University Hospital Alcides Car- neiro (HUAC). Children and adolescents on the screen- ing for these services and without diagnosis of over- weight or obesity were selected as control group. The sample corresponded to 70 volunteers, aged be- tween three and eighteen years, who sought care in the previously reported centers or under treatment, during 2010-2012. Patients with disabilities (mental, hearing, visual and physical, reporting to the motor impairment), customers or patients without accurate information on weight and height, immunocompromised individuals, and those who do not agreed on participation, even with the consent of those responsible, were excluded from the study. No conflict of interest, the study was approved by the Research Ethics Committee (REC) of the State Univer- sity of Paraíba (UEPB) under the protocol number 0513.0.133.000-09 and started after signing the Letter of Consent by the responsible regarding the investigated service and signing the informed consent by those re- sponsible in relation to the study volunteers (in case of adolescents, also their signature). Below is the flow dia- gram of this study: Population (189) ↓ Sample (70) Non obesity Control groupOverweight Obesity I, II or III Oral health condition and functional performance As instruments for data collection were used: face to face interview with questionnaire, intra-oral and extra- oral physical examination and application of adapted masticatory assessment protocol [10]; those conducted in the Department of Dentistry UEPB, under artificial light, following the guidelines of the World Health Organiza- tion for epidemiological surveys on oral health [11] and with respect to biosafety standards. Information regard- ing medical history was recorded from the data in re- cords. The list of variables analyzed included: sex, national origin, diagnosis and degree of obesity (weight/height ratio by Body Mass Index or BMI), treatment time and modality, use of medications, weight loss, family history of obesity, presence of comorbidity, presence of delete- rious oral habits, history of nervous bulimia, food pre- ferred consistency, performance characteristics of masti- catory function, pr esence of visible biofilm, spontaneou s gums bleeding, halitosis, changes in teeth/occlusion or soft tissues, dmft and mean DMFT. For statistical analysis were used 95% confidence in- Copyright © 2013 SciRes. OPEN ACCESS 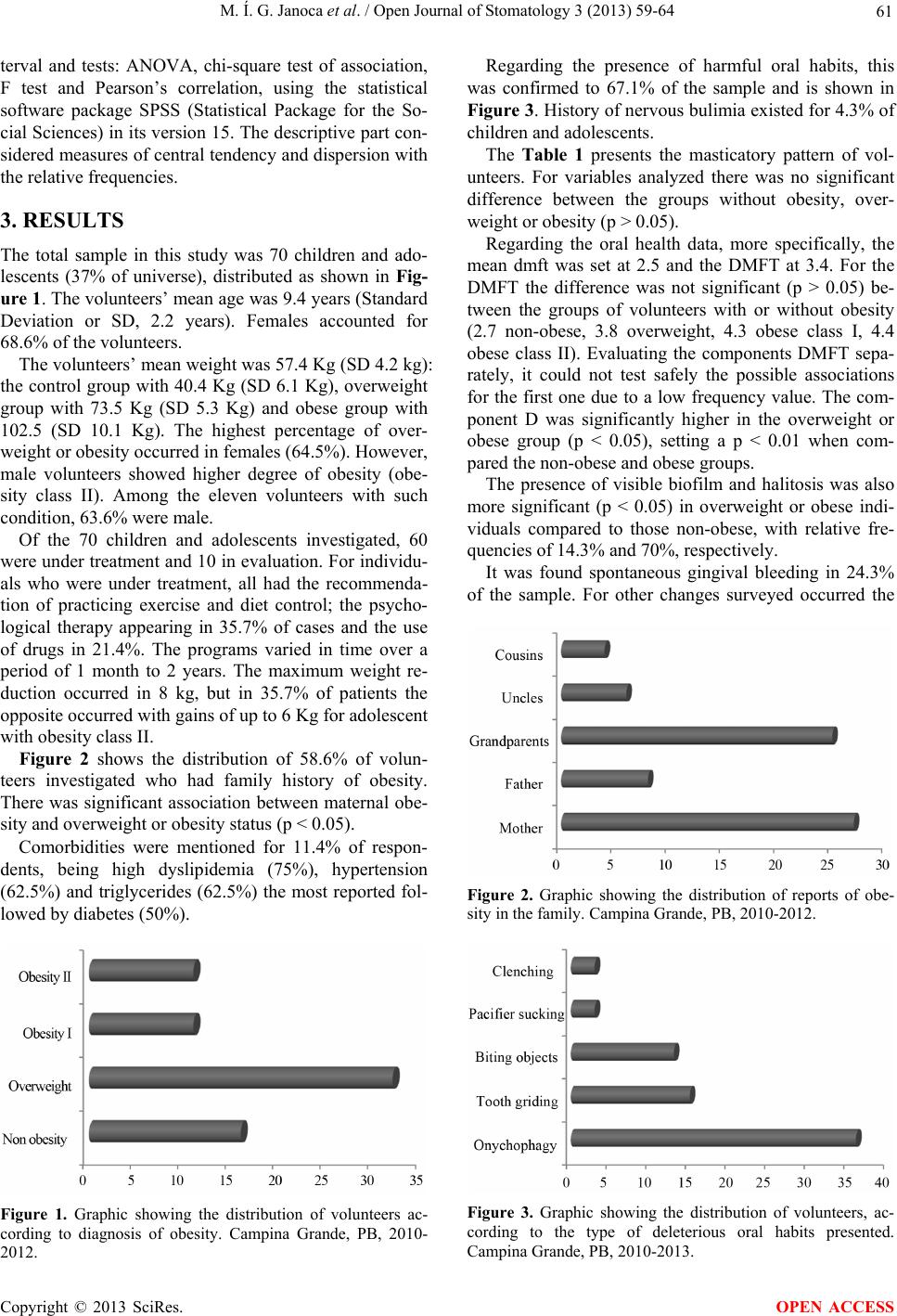 M. Í. G. Janoca et al. / Open Journal of Stomatology 3 (2013) 59-64 61 terval and tests: ANOVA, chi-square test of association, F test and Pearson’s correlation, using the statistical software package SPSS (Statistical Package for the So- cial Sciences) in its version 15. The descriptive part con- sidered measures of central tendency and dispersion with the relative frequencies. 3. RESULTS The total sample in this study was 70 children and ado- lescents (37% of universe), distributed as shown in Fig- ure 1. The volunteers’ mean age was 9.4 years (Standard Deviation or SD, 2.2 years). Females accounted for 68.6% of the volunteers. The volunteers’ mean weight was 57.4 Kg (SD 4.2 kg): the control group with 40.4 Kg (SD 6.1 Kg), overweight group with 73.5 Kg (SD 5.3 Kg) and obese group with 102.5 (SD 10.1 Kg). The highest percentage of over- weight or obesity occurred in females (64.5%). However, male volunteers showed higher degree of obesity (obe- sity class II). Among the eleven volunteers with such condition, 63.6% were male. Of the 70 children and adolescents investigated, 60 were under treatment and 10 in evaluation. For individu- als who were under treatment, all had the recommenda- tion of practicing exercise and diet control; the psycho- logical therapy appearing in 35.7% of cases and the use of drugs in 21.4%. The programs varied in time over a period of 1 month to 2 years. The maximum weight re- duction occurred in 8 kg, but in 35.7% of patients the opposite occurred with gains of up to 6 Kg for adolescent with obesity class II. Figure 2 shows the distribution of 58.6% of volun- teers investigated who had family history of obesity. There was significant association between maternal obe- sity and overweight or obesity status (p < 0.05). Comorbidities were mentioned for 11.4% of respon- dents, being high dyslipidemia (75%), hypertension (62.5%) and triglycerides (62.5%) the most reported fol- lowed by diabetes (50%). Figure 1. Graphic showing the distribution of volunteers ac- cording to diagnosis of obesity. Campina Grande, PB, 2010- 2012. Regarding the presence of harmful oral habits, this was confirmed to 67.1% of the sample and is shown in Figure 3. History of nervous bulimia existed for 4.3% of children and adolescents. The Table 1 presents the masticatory pattern of vol- unteers. For variables analyzed there was no significant difference between the groups without obesity, over- weight or obesity (p > 0.05). Regarding the oral health data, more specifically, the mean dmft was set at 2.5 and the DMFT at 3.4. For the DMFT the difference was not significant (p > 0.05) be- tween the groups of volunteers with or without obesity (2.7 non-obese, 3.8 overweight, 4.3 obese class I, 4.4 obese class II). Evaluating the components DMFT sepa- rately, it could not test safely the possible associations for the first one due to a low frequency value. The com- ponent D was significantly higher in the overweight or obese group (p < 0.05), setting a p < 0.01 when com- pared the non-obese and obese groups. The presence of visible biofilm and halitosis was also more significant (p < 0.05) in overweight or obese indi- viduals compared to those non-obese, with relative fre- quencies of 14. 3% an d 70%, respecti vel y . It was found spontaneous gingival bleeding in 24.3% of the sample. For other changes surveyed occurred the Figure 2. Graphic showing the distribution of reports of obe- sity in the family. Campina Grande, PB, 2010-2012. Figure 3. Graphic showing the distribution of volunteers, ac- cording to the type of deleterious oral habits presented. Campina Grande, PB, 2010-2013. Copyright © 2013 SciRes. OPEN ACCESS 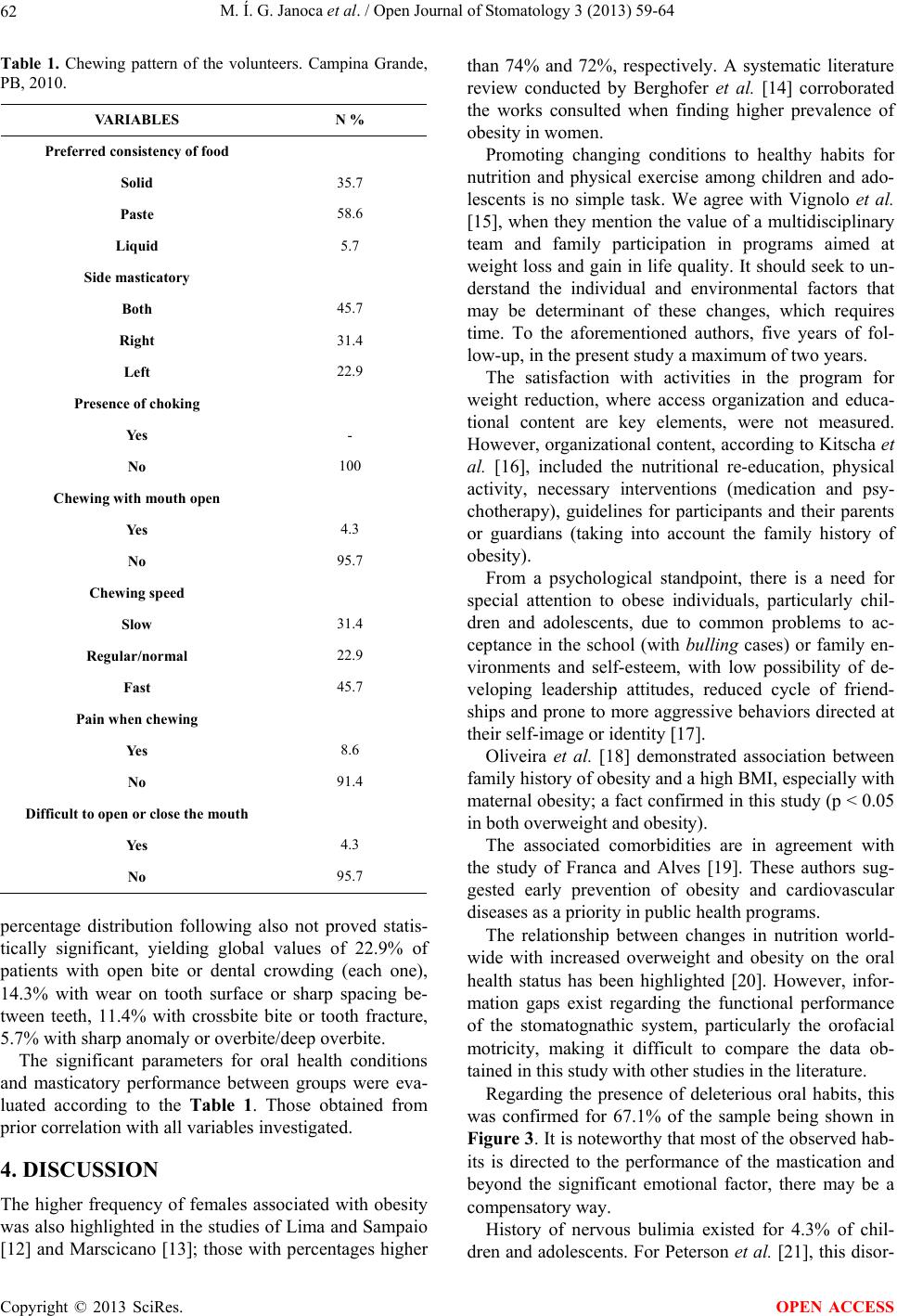 M. Í. G. Janoca et al. / Open Journal of Stomatology 3 (2013) 59-64 62 Table 1. Chewing pattern of the volunteers. Campina Grande, PB, 2010. VARIABLES N % Preferr ed consistency of food Solid 35.7 Paste 58.6 Liquid 5.7 Side masticatory Both 45.7 Right 31.4 Left 22.9 Presence of choking Yes - No 100 Chewing with mouth open Yes 4.3 No 95.7 Chewing speed Slow 31.4 Regular/normal 22.9 Fast 45.7 Pain when chewing Yes 8.6 No 91.4 Difficult to open or close the mouth Yes 4.3 No 95.7 percentage distribution following also not proved statis- tically significant, yielding global values of 22.9% of patients with open bite or dental crowding (each one), 14.3% with wear on tooth surface or sharp spacing be- tween teeth, 11.4% with crossbite bite or tooth fracture, 5.7% with sharp anomaly or overbite/deep overbite. The significant parameters for oral health conditions and masticatory performance between groups were eva- luated according to the Table 1. Those obtained from prior correlation with all variables investigated. 4. DISCUSSION The higher frequency of females associated with obesity was also highlighted in the studies of Lima and Sampaio [12] and Marscicano [13]; those with percentages higher than 74% and 72%, respectively. A systematic literature review conducted by Berghofer et al. [14] corroborated the works consulted when finding higher prevalence of obesity in women. Promoting changing conditions to healthy habits for nutrition and physical exercise among children and ado- lescents is no simple task. We agree with Vignolo et al. [15], when they mention the value of a multidisciplinary team and family participation in programs aimed at weight loss and gain in life quality. It sho uld seek to un- derstand the individual and environmental factors that may be determinant of these changes, which requires time. To the aforementioned authors, five years of fol- low-up, in the present study a maximum of two years. The satisfaction with activities in the program for weight reduction, where access organization and educa- tional content are key elements, were not measured. However, organizational content, according to Kitscha et al. [16], included the nutritional re-education, physical activity, necessary interventions (medication and psy- chotherapy), guidelines for participants and their parents or guardians (taking into account the family history of obesity). From a psychological standpoint, there is a need for special attention to obese individuals, particularly chil- dren and adolescents, due to common problems to ac- ceptance in the school (with bulling cases) or family en- vironments and self-esteem, with low possibility of de- veloping leadership attitudes, reduced cycle of friend- ships and prone to more aggressive behaviors directed at their self-image or identity [17]. Oliveira et al. [18] demonstrated association between family history of obesity and a high BMI, especially with maternal obesity; a fact confirmed in this study (p < 0.05 in both overw eight and obesity). The associated comorbidities are in agreement with the study of Franca and Alves [19]. These authors sug- gested early prevention of obesity and cardiovascular diseases as a priority in public health programs. The relationship between changes in nutrition world- wide with increased overweight and obesity on the oral health status has been highlighted [20]. However, infor- mation gaps exist regarding the functional performance of the stomatognathic system, particularly the orofacial motricity, making it difficult to compare the data ob- tained in this study with other studies in the literature. Regarding the presence of deleterious oral habits, this was confirmed for 67.1% of the sample being shown in Figure 3. It is noteworthy that most of the observed hab- its is directed to the performance of the mastication and beyond the significant emotional factor, there may be a compensatory way. History of nervous bulimia existed for 4.3% of chil- dren and adolescents. For Peterson et al. [21], this disor- Copyright © 2013 SciRes. OPEN ACCESS  M. Í. G. Janoca et al. / Open Journal of Stomatology 3 (2013) 59-64 63 der would be directly related to high levels of stress and depression in patients with eating disorders and would need to be computed so odd to conduct th e treatment and control of these individuals when losing weight. Chewing has implications for activation of histamine neurons (HA), those responsible for the increased lipoly- sis in adipose tissues and the feeling of fullness or satiety [22]. However, little is surveyed on the influence of mas- tication in the process of weight reduction. Apolinário, Moraes and Motta [23] in the study involving the masti- catory evaluation of 30 patients on the diet, reported that the guidelines on chewing are made in most of guidelines with emphasis on the speed and number of chewing cy- cles. They added that there is adaptation of the mastica- tory process, despite the unilateral mastication having been much noted. In this study, besides one preferred side, there was a preferred food consistency and speed masticatory unfavorable to the process; however, with no significant differences between overweight/obese group and that one without this conditio n. When reporting to oral conditions themselves, Bail- leul-Forestier et al., [24] identified a higher DMFT in obese patients (mean 6.9) compared to those non-obese (4.3); superior results to those found in this study. The inadequate food habits associated with frequency of food intake and low self-esteem (which includes care with personal hygiene) can be considered a risk factor for periodontal diseases by favoring the formation and calci- fication of the dent al bi o fi lm. Genco et al., [25] found significant association be- tween BMI and periodontal disease in obese individuals. These authors mentioned insulin resistance as a mediator of this relationship, without highlighting the occlusal aspects. The malocclusions observed in this study also possessed no significant association with BMI of volun- teers. The clinical implications of this study point to a different approach for the planning of Dental Caries Pre- ventive Programs in children and adolescents obese or overweight. A Different Approach for the Planning of Dental Car- ies Preventive Programs. 5. CONCLUSION Based on the results, a longer treatment with medication was directly associated with oral conditions in children and adolescents overweight or obese, particularly with the higher DMFT rates, presence of visible biofilm and higher frequency of halitosis. REFERENCES [1] Silva, J.B., Silva, F.G., Medeiros, H.J., Roncalli, A.G. and Knackfuss, M.I. (2009) Estado nutricional de lós Estudiantes de la región semiárida Del noreste de Brasil. Revista de Salud Publica (Bogota), 11, 62-71. http://dx.doi.org/10.1590/S0124-00642009000100007 [2] El Taguri, A., Dabbas-Tyan, M., Goulet, O. and Ricour, C. (2009) The use of body mass index for measurement of fat mass in children is highly dependant on abdominal fat. WHO, Eastern Mediterranean Health Journal, 15, 563-573. [3] Arora. A., Scott, J. A., Bhole, S., Do, L., Schwarz, E. and Blinkhorn, A.S. (2011) Early childhood feeding practices and dental caries in preschool children: A multi-centre birth cohort study. BMC Public Health, 11, 28. http://dx.doi.org/10.1186/1471-2458-11-28 [4] Silva-Sanigorski, A.M., Waters, E., Calache, H., Smith, M., Gold, L., Gussy, M., Scott, A., Lacy, K. and Virgo- Milton, M. (2011) Splash!: A prospective birth cohort study of the impact of environmental social and family- level influences on child oral health and obesity related risk factors and outcomes. BMC Public Health, 11, 505.http://dx.doi.org/10.1186/1471-2458-11-505 [5] Monteiro, P., Victora, C. and Barros, F. (2004) Fatores de risco sociais, familiares e comportamentais para obesi- dade em adolescentes. Revista Panamericana de Salud Publica, 16, 250-258. http://dx.doi.org/10.1590/S1020-49892004001000004 [6] Oliveira, C. L., Mello, M.T., Cintra, I.S. a nd Mauro, F.M. (2004) Obesidade e síndrome metabólica na infância e adolescência. Revista de Nut rição, 17, 237-245. http://dx.doi.org/10.1590/S1415-52732004000200010 [7] Batista Filho, M., Souza, A.I., Miglioli, T.C. and Santos, M.C. (2008) Anemia e obesidade: Um paradoxo da transição nutricional brasileira. Cadernos de Saúde Púb- lica, 24, S247-S257. http://dx.doi.org/10.1590/S0102-311X2008001400010 [8] Touger-Decker, R. and Mobley, C.C. (American Dietetic Association) (2007) Position of the American dietetic as- sociation. Oral. Journal of the American Dietetic Asso- ciation, 107, 1418-1428. http://dx.doi.org/10.1016/j.jada.2007.06.003 [9] Östberg, A.L., Bengtsson, C., Lissner, L. and Hakeberg, M. (2012) Oral health and obesity indicators. BMC Oral Health, 12, 50. http://dx.doi.org/10.1186/1472-6831-12-50 [10] Genaro, K.F., Berretin-Félix, G., Rehder, M.I.B.C. and Marchesan, I.Q. (2009) Avaliação miofuncional orofacial —Protocolo MGBR. Revista Cefac, 237-255. [11] Oliveira, A.J.R.C., Unfer, B., Costa, I.C.C., Arcieri, R.M., Guimarães, L.O.C. and Saliba, N.A. (1998) Levantamen- tos epidemiológicos em saúde bucal: análise da meto- dologia proposta pela Organização Mundial de Saúde. Revista Brasileira de Epidemiologia, 1, 177-189. http://dx.doi.org/10.1590/S1415-790X1998000200008 [12] Lima, L.P.D. and Sampaio, H.A.D.C. (2007) Caracteri- zação socioeconômica, antropométrica e alimentar de obesos graves. Ciências e Saúde Coletiva, 12, 1011-1020. http://dx.doi.org/10.1590/S1413-81232007000400022 [13] Marsicano, J.A. (2008) Avaliação das condições bucais de pacientes obesos e de submetidos à cirurgia bariátrica [dissertação de mestrado]. Faculdade de Odontologia da Copyright © 2013 SciRes. OPEN ACCESS  M. Í. G. Janoca et al. / Open Journal of Stomatology 3 (2013) 59-64 Copyright © 2013 SciRes. 64 OPEN ACCESS Universidade de São Paulo, Bauru. [14] Berghöfer, A., Pischon, T., Reinhold, T., Apovian, C.M., Sharma, A.M. and Willich, S.N. (2008) Obesity preva- lence from a European perspective: A systematic review. BMC Public Health, 8, 200. http://dx.doi.org/10.1186/1471-2458-8-200 [15] Vignolo, M., Rossi, F., Bardazza, G., Pistorio, A., Parodi, A., Spigno, S., Torrisi, C., Gremmo, M,. Veneselli, E. and Aicardi, G. (2008) Five-year follow-up of a cogni- tive-behavioural lifestyle multidisciplinary programme for childhood obesity outpatient treatment. Europen Journal of Clinical Nutrition, 62, 1047-1057. http://dx.doi.org/10.1038/sj.ejcn.1602819 [16] Kitscha, C.E., Brunet, K., Farmer, A. and Mager, D.R. (2009) Reasons for non-return to a pediatric weight ma- nagement program. Canadian Journal of Diet Practices and Research, 70, 89-94. http://dx.doi.org/10.3148/70.2.2009.89 [17] Zeller, M.H., Reiter-Purtill, J. and Ramey, C. (2008) Ne- gative peer perceptions of obese children in the classroom environment. Obesity, 16, 755-762. http://dx.doi.org/10.1038/oby.2008.4 [18] Oliveira, L.P.M., Assis, A.M.O., Silva, M.C.M., Santana, M.L.P., Santos, N.A., Pinheiro, S.M.C., Barreto, M.L. and Souza, C.O. (2009) Fatores associados a excesso de peso e concentração de gordura abdominal em adultos na cidade de Salvador, Cadernos de Saúde Publica, Bahia, 25, 570-582. http://dx.doi.org/10.1590/S0102-311X2009000300012 [19] Franca, E. and Alves, J.G.B. (2006) Dislipidemia entre crianças e adolescentes de Pernambuco. Arquivos Bra- sileiros de Cardiologia, 87, 722-727. http://dx.doi.org/10.1590/S0066-782X2006001900007 [20] Enwonwu, C.O. (2010) Global nutrition transition chal- lenges oral health. Compendium of Continuing Education in Dentistry, 31, 98-99. [21] Peterson, C.B., Thuras, P., Ackard, D.M., Mitchell, J.E., Berg, K., Sandager, N. and Wonderlich, S.A. (2010) Per- sonality dimensions in bulimia nervosa, binge eating dis- order, and obesity. Comprehensive Psychiatry, 51, 31-36. http://dx.doi.org/10.1016/j.comppsych.2009.03.003 [22] Sakata, T., Yoshimatsu, H., Masaki, T. and Tsuda, K. (2003) Anti-obesity actions of mastication driven by his- tamine neurons in rats. Experimental Biology and Medi- cine, 228, 1106-1110. [23] Apolinário, R.M.C., Moraes, R.B. and Motta, A.R. (2008) Mastigação e dietas alimentares para a redução do peso. Revista Cefac, 10, 191-199. http://dx.doi.org/10.1590/S1516-18462008000200008 [24] Bailleul-Forestier, I., Lopes, K., Sounames, M., Azou- guy-Levy, S. and Frelut, M.L. (2007) Caries experience in a severely obese adolescent population. Journal of the International Association of Dentistry for Children, 17, 358-363. [25] Genco, R.J., Grossi, S.G. , Ho, A., Nishimura, F. and Mu- rayama, Y.A. (2005) A proposed mode linking inflamma- tion to obesity, diabetes, and periodontal infections. Jour- nal of Periodontology, 76, 2075-2084. http://dx.doi.org/10.1902/jop.2005.76.11-S.2075
|