Partial Nephrectomy for Renal Cell Carcinoma: Risk Factors for Acute Post-Operative Hemorrhage
and Impact on Subsequent Hospital Course and Complete Nephrectomy Rate.
8
An Analysis of 200 Consecutive Cases
However, a recent analysis utilizing the Surveillance,
Epidemiology ad End Results program during that same
time period showed that in the US only 35.2% of patients
with T1a (≤4 cm) renal masses received partial nephrec-
tomy between 1999 and 2006 [11]. That same study re-
vealed that only 50% of tumors <2 cm were treated with
partial nephrectomy, and 48% of tumors between 2 and 4
cm were treated with partial nephrectomy [12].
There is increasing evidence that surgically induced
chronic kidney disease [13,14] following complete neph-
rectomy is associated with increased risk of cardiovascu-
lar disease including death [15,16] and metabolic adverse
consequences including anemia, acidosis, and osteoporo-
sis [17,18] and associated significant adverse health con-
sequences.
The reason for underutilization of partial nephrectomy
compared to radical nephrectomy for management of the
T1a (<4 cm) and select T1b 4 - 7 cm) renal mass is un-
clear, and is beyond the scope of the current investigation.
Investigators have suggested that the explanation may be
multifactorial, including physician and patient factors,
and that the decision making requires complex multi
perspective reasoning [19]. It is generally recognized that
partial nephrectomy is a complex procedure requiring
surgical expertise, a dedicated operating room team and
advanced surgical technology, and that partial nephrec-
tomy is associated with increased surgical risk both in-
tra-operative and post-operative, the most devastating
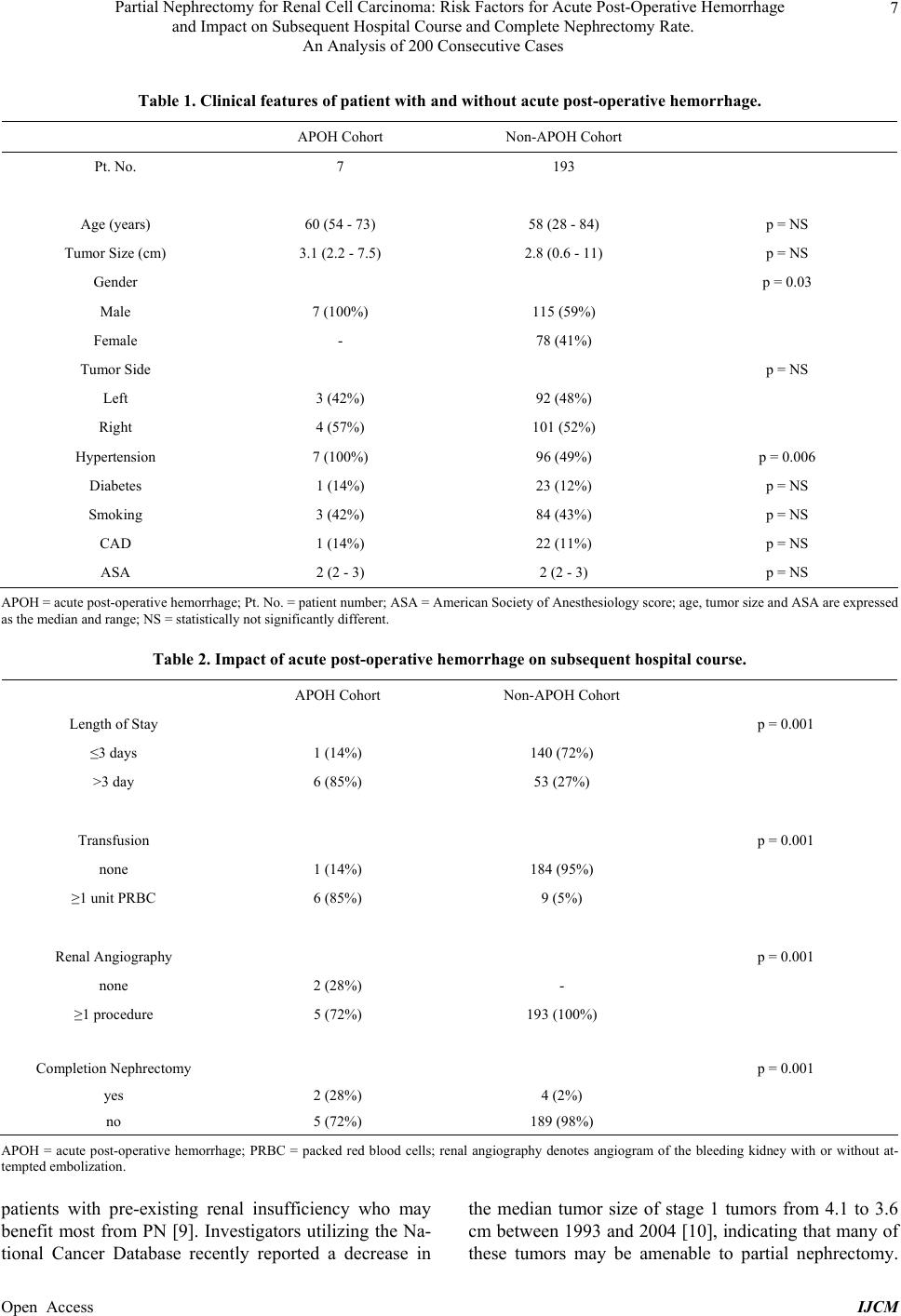
being post-operative hemorrhage. The present study
sought to identify risk factors for APOH after partial
nephrectomy. Though a rare event, APOH increased the
hospital length of stay, the transfusion rate, the need for
ancillary procedures and most importantly, the complete
nephrectomy rate which was 29% in the APOH cohort
compared to 2% in the non-APOH group. Furthermore,
we sought to identify risk factors associated with APOH.
So that such knowledge may allow preemptive risk re-
duction. At our institution all hypertensive males are
treated under the care of a cardiologist to maximize hy-
pertension management for at least 1 month prior to par-
tial nephrectomy. In addition, we have instituted a
peri-operative protocol to maintain normotensive status
throughout the intra-operative and post-operative period.
Whereas in the past all patients received PRN supple-
mental meds for hypertension, now our protocol admin-
isters that medication (usually beta-blockade) as standing
order with hold parameter (i.e. Systolic BP < 100 mmHg
or HR < 60 bpm). We attempt to maintain a mean arterial
pressure of 70 - 80. Since the institution of this protocol
in October 2011 we have not experienced an APOH.
During this period, our patient criteria, volume, surgical
technique and post-operative pathway [20] remain con-
stant.
5. Conclusion
In the present analysis, APOH was associated with ex-
tended hospitalization, the increased transfusion require-
ment and the need for more ancillary procedures. APOH
patients were at significantly increased risk of renal loss.
Male gender and hypertension were associated with in-
creased risk for APOH. We have incorporated this in-
formation into an APOH risk reduction program at our
institution.
REFERENCES
[1] S. C. Campbell, A. C. Novick, A. Belldegrun, et al.,
“Guidelines for Management of the Clinical T1 Renal
Mass,” Journal of Urology, Vol. 182, No. 4, 2009, pp.
1271-1279. http://dx.doi.org/10.1016/j.juro.2009.07.004
[2] M. C. Smaldone, B. Egleston, R. G. Uzzo and A. Kutikov,
“Does Partialnephrectomy Result in a Durable Overall
Survival Benefit in the Medicare Population?” Journal of
Urology, Vol. 188, No. 6, 2012, pp. 2089-2094.
http://dx.doi.org/10.1016/j.juro.2012.07.099
[3] S. P. Kim, R. H. Thompson, S. A. Boorjian, et al., “Com-
parative Effectiveness for Survival and Renal Function of
Partial and Radical Nephrectomy for Localized Renal
Tumor: A Systematic Review and Meta-Analysis,” Jour-
nal of Urology, Vol. 188, No. 1, 2012, pp. 51-57.
http://dx.doi.org/10.1016/j.juro.2012.03.006
[4] A. Kutilov and R. G. Uzzo, “The R.E.N.A.L. Nephro-
tomy Score: A Comprehensive Standardized System for
Quantitating Renal Tumor Score, Location and DEPTH,”
Journal of Urology, Vol. 182, No. 3, 2009, pp. 844-853.
http://dx.doi.org/10.1016/j.juro.2009.05.035
[5] J. L. Fleiss, “Statistical Methods for Rates and Propor-
tions,” 2nd Edition, John Wiley & Sons, 1981.
[6] American Cancer Society Cancer Facts and Figures, “At-
lanta,” American Cancer Society.
http://seer.cancer.gov/
[7] W. H. Chow, S. S. Devesa, J. L. Warren and J. F. Frau-
meni, “Rising Incidence of Renal Cell Carcinoma in the
United States,” JAMA, Vol. 281, No. 17, 1999, pp. 1628-
1631. http://dx.doi.org/10.1001/jama.281.17.1628
[8] P. Russo, “Renal Cell Carcinoma Presentation, Staging
and Surgical Treatment,” Seminars in Oncology, Vol. 27,
No. 2, 2000, pp. 160-166.
[9] J. M. Woldrich, K. Palazzi, S. P. Stroup, et al., “Trends in
the Surgical Management of Localized Renal Masses:
Thermal Ablation, Partial and Radical Nephrectomy in
the USA, 1999-2008,” BJU International, Vol. 111, No. 8,
2012, pp. 1261-1268.
http://dx.doi.org/10.1111/j.1464-410X.2012.11497.x
[10] C. J. Kane, K. Mallin, J. Ritchey, et al., “Renal Cell Can-
cer Stage Migration: Analysis of the National Cancer
Data Base,” Cancer, Vol. 113, No. 1, 2008, pp. 78-83.
Open Access IJCM