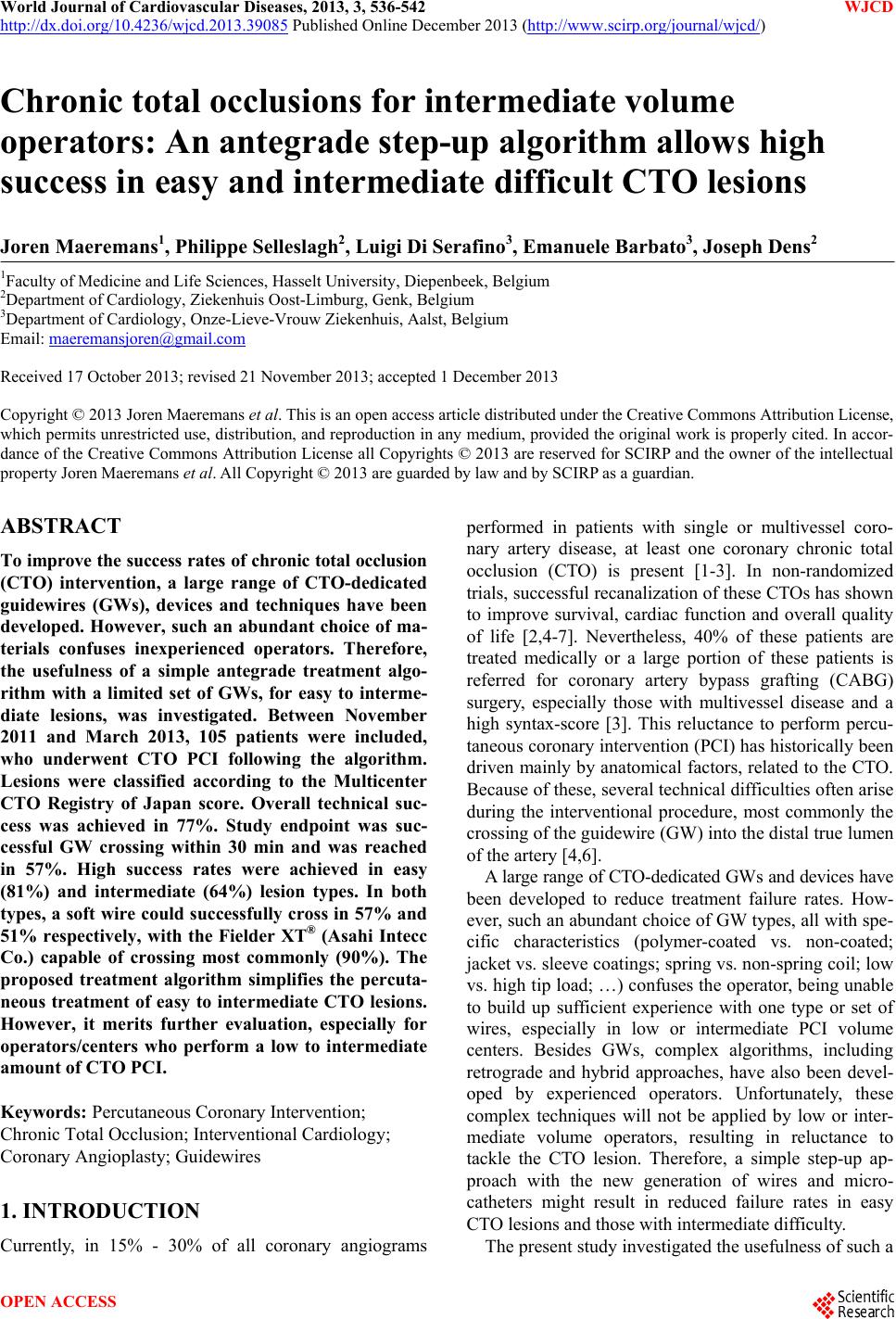
 World Journal of Cardiovascular Diseases, 2013, 3, 536-542 WJCD http://dx.doi.org/10.4236/wjcd.2013.39085 Published Online December 2013 (http://www.scirp.org/journal/wjcd/) Chronic total occlusions for intermediate volume operators: An antegrade step-up algorithm allows high success in easy and intermediate difficult CTO lesions Joren Maeremans1, Philippe Selleslagh2, Luigi Di Serafino3, Emanuele Barbato3, Joseph Dens2 1Faculty of Medicine and Life Sciences, Hasselt University, Diepenbeek, Belgium 2Department of Cardiology, Ziekenhuis Oost-Limburg, Genk, Belgium 3Department of Cardiology, Onze-Lieve-Vrouw Ziekenhuis, Aalst, Belgium Email: maeremansjoren@gmail.com Received 17 October 2013; revised 21 November 2013; accepted 1 December 2013 Copyright © 2013 Joren Maeremans et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In accor- dance of the Creative Commons Attribution License all Copyrights © 2013 are reserved for SCIRP and the owner of the intellectual property Joren Maeremans et al. All Copyright © 2013 are guarded by law and by SCIRP as a guardian. ABSTRACT To improve the success rates of chronic total occlusion (CTO) intervention, a large range of CTO-dedicated guidewires (GWs), devices and techniques have been developed. However, such an abundant choice of ma- terials confuses inexperienced operators. Therefore, the usefulness of a simple antegrade treatment algo- rithm with a limited set of GWs, for easy to interme- diate lesions, was investigated. Between November 2011 and March 2013, 105 patients were included, who underwent CTO PCI following the algorithm. Lesions were classified according to the Multicenter CTO Registry of Japan score. Overall technical suc- cess was achieved in 77%. Study endpoint was suc- cessful GW crossing within 30 min and was reached in 57%. High success rates were achieved in easy (81%) and intermediate (64%) lesion types. In both types, a soft wire could successfully cross in 57% and 51% respectively, with the Fielder XT® (Asahi Intecc Co.) capable of crossing most commonly (90%). The proposed treatment algorithm simplifies the percuta- neous treatment of easy to intermediate CTO lesions. However, it merits further evaluation, especially for operators/centers who perform a low to intermediate amount of CTO PCI. Keywords: Percutaneous Coronary Intervention; Chronic Total Occlusion; Interventional Cardiology; Coronary Angioplasty; Guidewires 1. INTRODUCTION Currently, in 15% - 30% of all coronary angiograms performed in patients with single or multivessel coro- nary artery disease, at least one coronary chronic total occlusion (CTO) is present [1-3]. In non-randomized trials, successful recanalization of these CTOs has shown to improve survival, cardiac function and overall quality of life [2,4-7]. Nevertheless, 40% of these patients are treated medically or a large portion of these patients is referred for coronary artery bypass grafting (CABG) surgery, especially those with multivessel disease and a high syntax-score [3]. This reluctance to perform percu- taneous coronary intervention (PCI) has historically been driven mainly by anatomical factors, related to the CTO. Because of these, several technical difficulties often arise during the interventional procedure, most commonly the crossing of the guidewire (GW) into the distal true lumen of the artery [4,6]. A large range of CTO-dedicated GWs and devices have been developed to reduce treatment failure rates. How- ever, such an abundant choice of GW types, all with spe- cific characteristics (polymer-coated vs. non-coated; jacket vs. sleeve coatings; spring vs. non-spring coil; low vs. high tip load; …) confuses the operator, being unable to build up sufficient experience with one type or set of wires, especially in low or intermediate PCI volume centers. Besides GWs, complex algorithms, including retrograde and hybrid approaches, have also been devel- oped by experienced operators. Unfortunately, these complex techniques will not be applied by low or inter- mediate volume operators, resulting in reluctance to tackle the CTO lesion. Therefore, a simple step-up ap- proach with the new generation of wires and micro- catheters might result in reduced failure rates in easy CTO lesions and those with intermediate difficulty. The present study investigated the usefulness of such a OPEN ACCESS 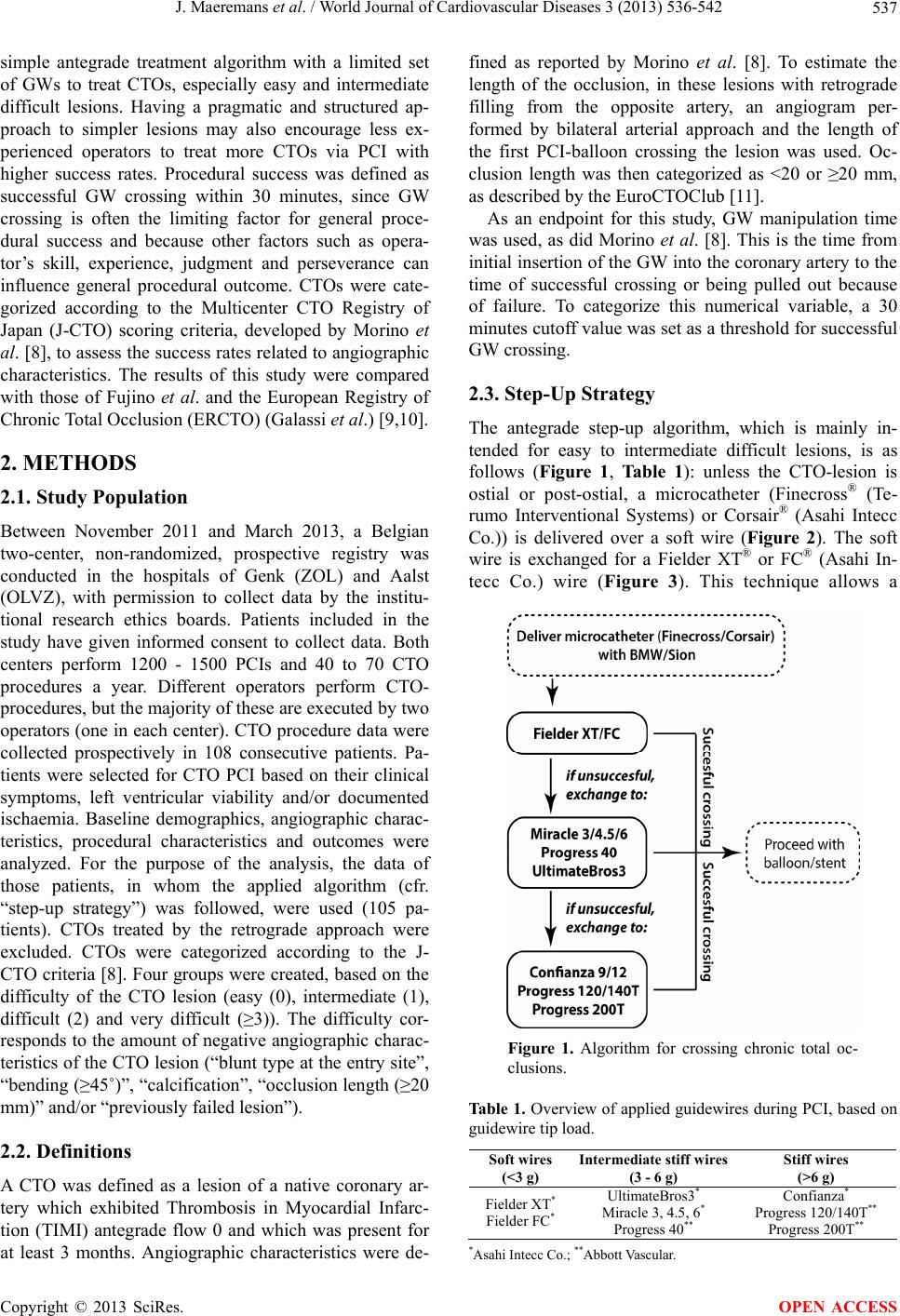 J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 537 simple antegrade treatment algorithm with a limited set of GWs to treat CTOs, especially easy and intermediate difficult lesions. Having a pragmatic and structured ap- proach to simpler lesions may also encourage less ex- perienced operators to treat more CTOs via PCI with higher success rates. Procedural success was defined as successful GW crossing within 30 minutes, since GW crossing is often the limiting factor for general proce- dural success and because other factors such as opera- tor’s skill, experience, judgment and perseverance can influence general procedural outcome. CTOs were cate- gorized according to the Multicenter CTO Registry of Japan (J-CTO) scoring criteria, developed by Morino et al. [8], to assess the success rates related to angiographic characteristics. The results of this study were compared with those of Fujino et al. and the European Registry of Chronic Total Occlusion (ERCTO) (Galassi et al.) [9,10]. 2. METHODS 2.1. Study Population Between November 2011 and March 2013, a Belgian two-center, non-randomized, prospective registry was conducted in the hospitals of Genk (ZOL) and Aalst (OLVZ), with permission to collect data by the institu- tional research ethics boards. Patients included in the study have given informed consent to collect data. Both centers perform 1200 - 1500 PCIs and 40 to 70 CTO procedures a year. Different operators perform CTO- procedures, but the majority of these are executed by two operators (one in each center). CTO procedure data were collected prospectively in 108 consecutive patients. Pa- tients were selected for CTO PCI based on their clinical symptoms, left ventricular viability and/or documented ischaemia. Baseline demographics, angiographic charac- teristics, procedural characteristics and outcomes were analyzed. For the purpose of the analysis, the data of those patients, in whom the applied algorithm (cfr. “step-up strategy”) was followed, were used (105 pa- tients). CTOs treated by the retrograde approach were excluded. CTOs were categorized according to the J- CTO criteria [8]. Four groups were created, based on the difficulty of the CTO lesion (easy (0), intermediate (1), difficult (2) and very difficult (≥3)). The difficulty cor- responds to the amount of negative angiographic charac- teristics of the CTO lesion (“blunt type at the entry site”, “bending (≥45˚)”, “calcification”, “occlusion length (≥20 mm)” and/or “previously failed lesion”). 2.2. Definitions A CTO was defined as a lesion of a native coronary ar- tery which exhibited Thrombosis in Myocardial Infarc- tion (TIMI) antegrade flow 0 and which was present for at least 3 months. Angiographic characteristics were de- fined as reported by Morino et al. [8]. To estimate the length of the occlusion, in these lesions with retrograde filling from the opposite artery, an angiogram per- formed by bilateral arterial approach and the length of the first PCI-balloon crossing the lesion was used. Oc- clusion length was then categorized as <20 or ≥20 mm, as described by the EuroCTOClub [11]. As an endpoint for this study, GW manipulation time was used, as did Morino et al. [8]. This is the time from initial insertion of the GW into the coronary artery to the time of successful crossing or being pulled out because of failure. To categorize this numerical variable, a 30 minutes cutoff value was set as a threshold for successful GW crossing. 2.3. Step-Up Strategy The antegrade step-up algorithm, which is mainly in- tended for easy to intermediate difficult lesions, is as follows (Figure 1, Table 1): unless the CTO-lesion is ostial or post-ostial, a microcatheter (Finecross® (Te- rumo Interventional Systems) or Corsair® (Asahi Intecc Co.)) is delivered over a soft wire (Figure 2). The soft wire is exchanged for a Fielder XT® or FC® (Asahi In- tecc Co.) wire (Figure 3). This technique allows a Figure 1. Algorithm for crossing chronic total oc- clusions. Table 1. Overview of applied guidewires during PCI, based on guidewire tip load. Soft wires (<3 g) Intermediate stiff wires (3 - 6 g) Stiff wires (>6 g) Fielder XT* Fielder FC* UltimateBros3* Miracle 3, 4.5, 6* Progress 40** Confianza* Progress 120/140T** Progress 200T** *Asahi Intecc Co.; **Abbott Vascular. Copyright © 2013 SciRes. OPEN ACCESS 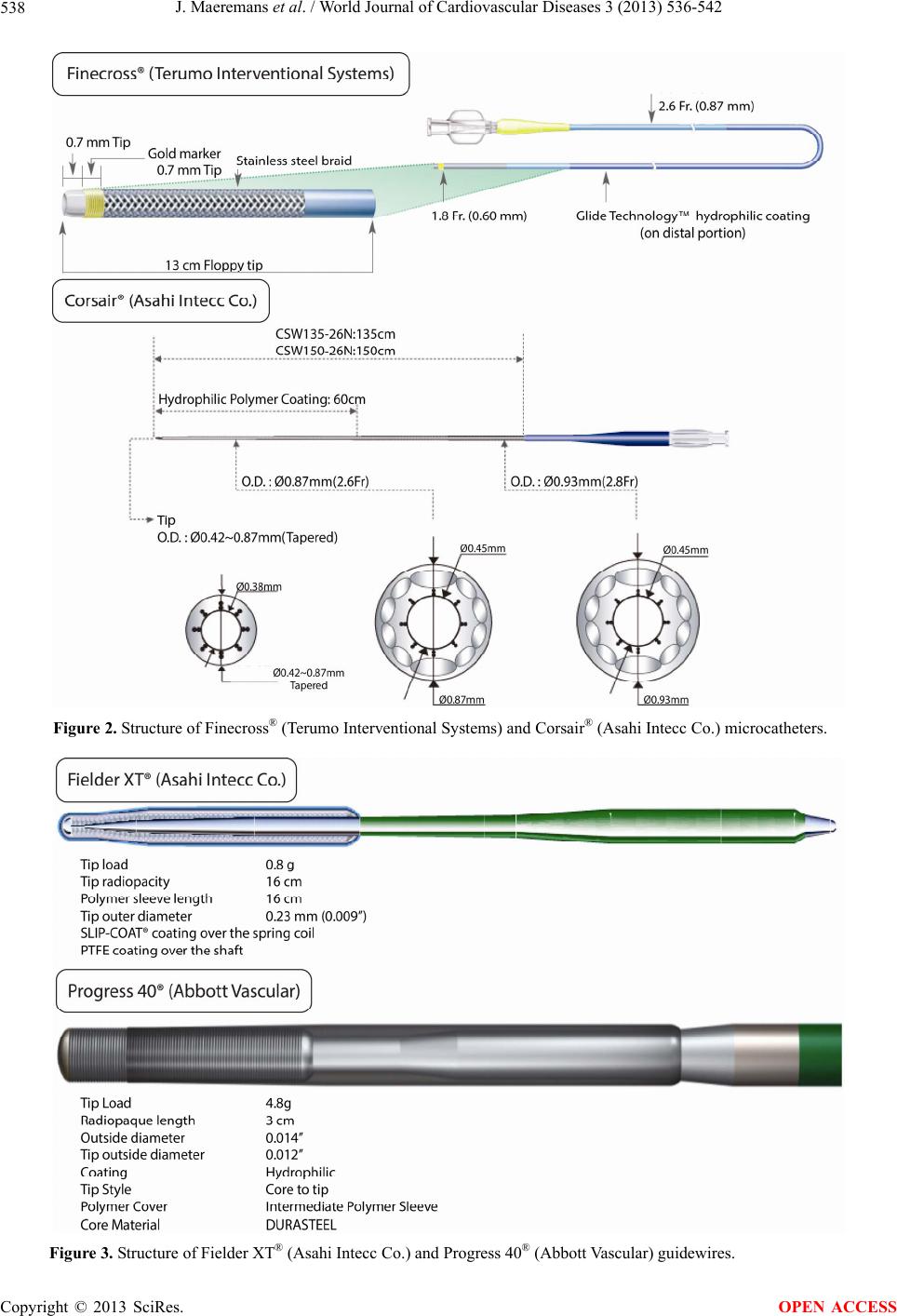 J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 Copyright © 2013 SciRes. 538 Figure 2. Structure of Finecross® (Terumo Interventional Systems) and Corsair® (Asahi Intecc Co.) microcatheters. Figure 3. Structure of Fielder XT® (Asahi Intecc Co.) and Progress 40® (Abbott Vascular) guidewires. OPEN ACCESS  J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 539 specific shape of the tip of the dedicated CTO wire. Fielder XT® and FC® are defined as soft wires, based on the low tip load of these wires. Upon failure, a GW ex- change to an intermediate stiff wire was made. Follow- ing the algorithm, this second wire is a Miracle® 3/4.5/6 (Asahi Intecc Co.) or Progress 40® (Abbott Vascular). During the registry, the UltimateBros3® (Asahi Intecc Co.) became available which replaced the Miracle® as the wire of preference. If unsuccessful, exchange to- wards even more stiff wires was performed, with the Confianza® (Pro) (Asahi Intecc Co.), Progress® 120, 140T and 200T (Abbott Vascular) as preferred wires. In both centers the wire of preference to start with was the Fielder XT® wire. 2.4. Guidewires The Fielder XT® is a soft and tapered GW with a tip load and diameter of respectively 0.8g and 0.009" (Figure 3). The outer diameter is 0.014". It has a stainless steel spring coil core, with a hydrophilic polymer sleeve coat- ing at the distal end of the wire which provides lubricity and trackability for tortuous vessels. A PTFE-coating covers the shaft of the wire. The Fielder FC® has similar characteristics as the Fielder XT® but is not tapered and its polymer sleeve is a bit longer. The Miracle® 3/4.5/6 and UltimateBros3® GWs are both intermediate stiff GWs with tip loads between 3 and 6 g. The core wire and distal coil are designed to resist great force. The higher tip load increases driving force against tight lesions. The UltimateBros3® has a longer hydrophilic polymer coat- ing which maintains high maneuverability, allowing im- proved wire manipulation in tight lesions. The Confi- anza® GW has a tapered tip diameter of 0.009" and a non-hydrophilic coating. In combination with its heavy tip load, highly resistant lesions can be penetrated. The Progress®-family is a family of CTO wires coated with a lubricious, hydrophilic sleeve coating (Figure 3). As a core, these wires have DURASTEEL® and both the outer and tip diameter is 0.014”. This family has different tip loads resulting in a range of tip stiffness. 2.5. Statistical Analysis Univariate analyses were performed to assess the rela- tionship between the patients’ baseline and angiogra- phic characteristics and successful GW crossing within 30 minutes. Numerical values were expressed as mean ± standard deviation, while categorical variables were ex- pressed as percentage of total. Normality was assessed using the Shapiro-Wilk statistic. Comparisons between groups were performed using Fisher’s exact test for categorical variables and the independent Student’s t-test for continuous variables, with the level of significance set at p ≤ 0.05. Data on procedural characteristics and procedural success rates were also calculated for the dif- ferent J-CTO difficulty groups. In addition, a subdivision was made according to the applied treatment algorithm. All statistical analyses were carried out using SPSS Sta- tistics version 20 (IBM SPSS Inc.). 3. RESULTS 3.1. Study Population, Overall Results and Procedural Characteristics The algorithm was followed in 105 out of 108 patients (97.2%). In 81 of these patients, general success was achieved (77.1%) (Table 2). Lesions were categorized into difficulty risk groups (easy, intermediate, difficult and very difficult), according to the J-CTO scoring model [8]. In this way, respectively 21, 42, 28 and 14 patients were assigned to each group. In 83.8% of all lesions, a microcatheter was used. Overall success was achieved in 90.5%, 81%, 82.1% and 35.7% of each group respectively. For each risk group, procedural cha- racteristics were evaluated (Table 2). This includes the number of wires used, procedure times, fluoroscopy times, contrast use and radiation doses. An increase in these values is seen in accordance with lesion difficulty. The values in the very difficult group do not differ signi- ficantly from the difficult, due to abortion of the proce- dure by the operator, if it seemed futile to continue. Ne- vertheless, these values are relatively low and clearly within safety margins for contrast use and radiation ex- posure. The primary endpoint of this study was successful GW crossing within 30 minutes. The baseline characteristics as well as angiographic characteristics and procedural outcomes of the study population, classified according to this primary endpoint, are reported in Table 3. No sig- nificant differences were present between the two groups for baseline characteristics except for age (62.9 ± 10.9 vs. 67.4 ± 9.5, p = 0.03). Concerning angiographic charac- teristics, the failure rate to cross within 30 minutes was clearly higher if the shape of the entry site was blunt (10.0% vs. 40.0%, p = 0.000) and when calcifications were present (28.3% vs. 57.8%, p = 0.003). Other an- giographic characteristics were not significantly different, although this might be due to the sample size. 3.2. Successful Guidewire Crossing and Step-Up Algorithm In 57% of all patients, the primary endpoint of suc- cessful GW crossing within 30 minutes was achieved (Table 4). According to the model of Morino et al. [8], the primary endpoint was achieved in 17 (81%), 27 (64%), 13 (46%) and 3 (21%) cases respectively. In total, 43% of 94 CTO lesions could be crossed within 30 minutes by using only soft wires. In 95% of Copyright © 2013 SciRes. OPEN ACCESS 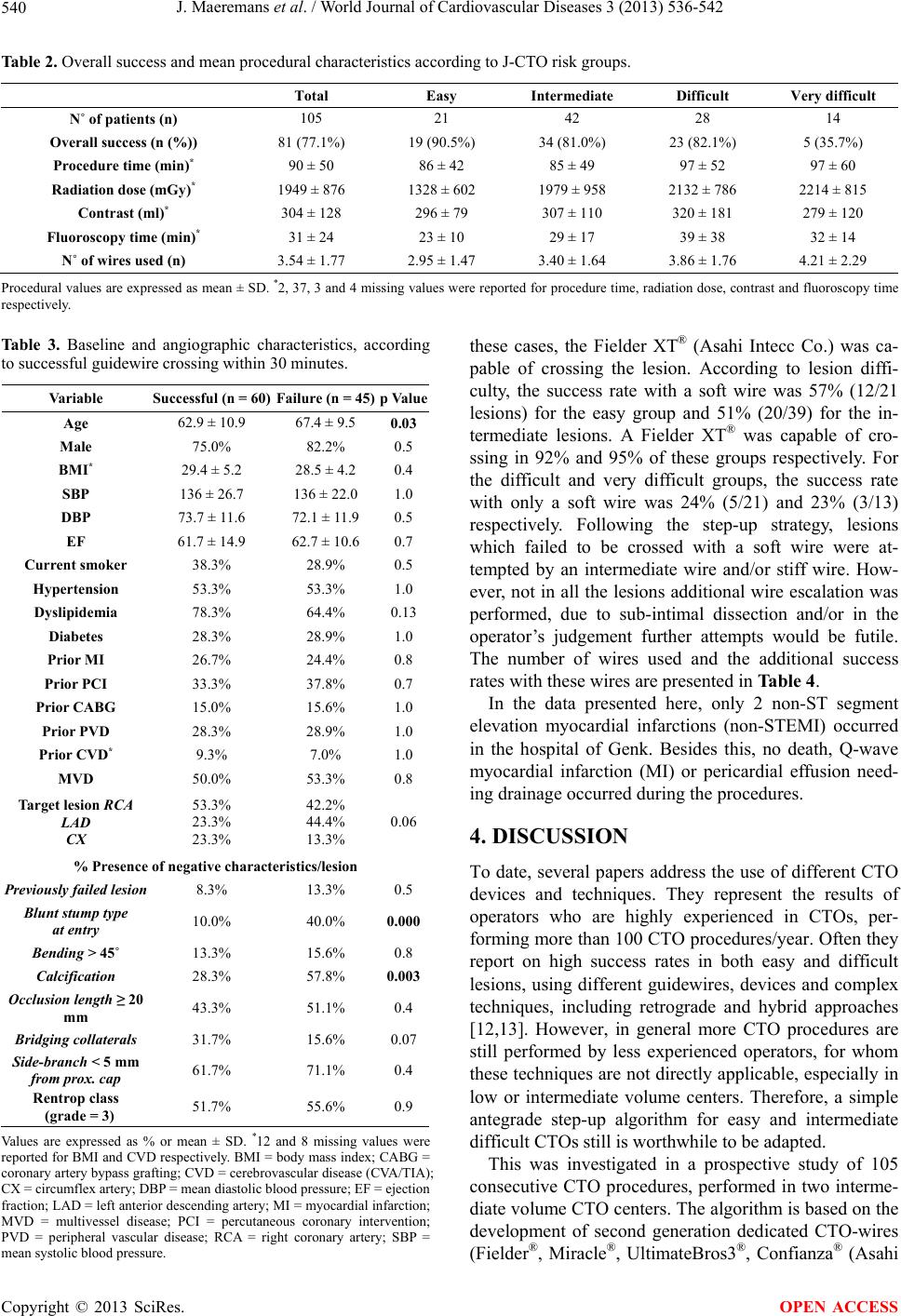 J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 540 Table 2. Overall success and mean procedural characteristics according to J-CTO risk groups. Total Easy Intermediate Difficult Very difficult N˚ of patients (n) 105 21 42 28 14 Overall success (n (%)) 81 (77.1%) 19 (90.5%) 34 (81.0%) 23 (82.1%) 5 (35.7%) Procedure time (min)* 90 ± 50 86 ± 42 85 ± 49 97 ± 52 97 ± 60 Radiation dose (mGy)* 1949 ± 876 1328 ± 602 1979 ± 958 2132 ± 786 2214 ± 815 Contrast (ml)* 304 ± 128 296 ± 79 307 ± 110 320 ± 181 279 ± 120 Fluoroscopy time (min)* 31 ± 24 23 ± 10 29 ± 17 39 ± 38 32 ± 14 N˚ of wires used (n) 3.54 ± 1.77 2.95 ± 1.47 3.40 ± 1.64 3.86 ± 1.76 4.21 ± 2.29 Procedural values are expressed as mean ± SD. *2, 37, 3 and 4 missing values were reported for procedure time, radiation dose, contrast and fluoroscopy time respectively. Table 3. Baseline and angiographic characteristics, according to successful guidewire crossing within 30 minutes. Variable Successful (n = 60) Failure (n = 45)p Value Age 62.9 ± 10.9 67.4 ± 9.5 0.03 Male 75.0% 82.2% 0.5 BMI* 29.4 ± 5.2 28.5 ± 4.2 0.4 SBP 136 ± 26.7 136 ± 22.0 1.0 DBP 73.7 ± 11.6 72.1 ± 11.9 0.5 EF 61.7 ± 14.9 62.7 ± 10.6 0.7 Current smoker 38.3% 28.9% 0.5 Hypertension 53.3% 53.3% 1.0 Dyslipidemia 78.3% 64.4% 0.13 Diabetes 28.3% 28.9% 1.0 Prior MI 26.7% 24.4% 0.8 Prior PCI 33.3% 37.8% 0.7 Prior CABG 15.0% 15.6% 1.0 Prior PVD 28.3% 28.9% 1.0 Prior CVD* 9.3% 7.0% 1.0 MVD 50.0% 53.3% 0.8 Target lesion RCA LAD CX 53.3% 23.3% 23.3% 42.2% 44.4% 13.3% 0.06 % Presence of negative characteristics/lesion Previously failed lesion 8.3% 13.3% 0.5 Blunt stump type at entry 10.0% 40.0% 0.000 Bending > 45˚ 13.3% 15.6% 0.8 Calcification 28.3% 57.8% 0.003 Occlusion length ≥ 20 mm 43.3% 51.1% 0.4 Bridging collaterals 31.7% 15.6% 0.07 Side-branch < 5 mm from prox. cap 61.7% 71.1% 0.4 Rentrop class (grade = 3) 51.7% 55.6% 0.9 Values are expressed as % or mean ± SD. *12 and 8 missing values were reported for BMI and CVD respectively. BMI = body mass index; CABG = coronary artery bypass grafting; CVD = cerebrovascular disease (CVA/TIA); CX = circumflex artery; DBP = mean diastolic blood pressure; EF = ejection fraction; LAD = left anterior descending artery; MI = myocardial infarction; MVD = multivessel disease; PCI = percutaneous coronary intervention; PVD = peripheral vascular disease; RCA = right coronary artery; SBP = mean systolic blood pressure. these cases, the Fielder XT® (Asahi Intecc Co.) was ca- pable of crossing the lesion. According to lesion diffi- culty, the success rate with a soft wire was 57% (12/21 lesions) for the easy group and 51% (20/39) for the in- termediate lesions. A Fielder XT® was capable of cro- ssing in 92% and 95% of these groups respectively. For the difficult and very difficult groups, the success rate with only a soft wire was 24% (5/21) and 23% (3/13) respectively. Following the step-up strategy, lesions which failed to be crossed with a soft wire were at- tempted by an intermediate wire and/or stiff wire. How- ever, not in all the lesions additional wire escalation was performed, due to sub-intimal dissection and/or in the operator’s judgement further attempts would be futile. The number of wires used and the additional success rates with these wires are presented in Table 4. In the data presented here, only 2 non-ST segment elevation myocardial infarctions (non-STEMI) occurred in the hospital of Genk. Besides this, no death, Q-wave myocardial infarction (MI) or pericardial effusion need- ing drainage occurred during the procedures. 4. DISCUSSION To date, several papers address the use of different CTO devices and techniques. They represent the results of operators who are highly experienced in CTOs, per- forming more than 100 CTO procedures/year. Often they report on high success rates in both easy and difficult lesions, using different guidewires, devices and complex techniques, including retrograde and hybrid approaches [12,13]. However, in general more CTO procedures are still performed by less experienced operators, for whom these techniques are not directly applicable, especially in low or intermediate volume centers. Therefore, a simple antegrade step-up algorithm for easy and intermediate difficult CTOs still is worthwhile to be adapted. This was investigated in a prospective study of 105 consecutive CTO procedures, performed in two interme- diate volume CTO centers. The algorithm is based on the development of second generation dedicated CTO-wires (Fielder®, Miracle®, UltimateBros3®, Confianza® (Asahi Copyright © 2013 SciRes. OPEN ACCESS  J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 541 Table 4. Successful guidewire crossing within 30 minutes, according to J-CTO difficulty groups and applied step-up strategy. Total Easy Intermediate Difficult Very difficult N˚ of patients (n) 105 21 42 28 14 Successful crossing ≤ 30 minutes 57% (60/105) 81% (17/21) 64% (27/42) 46% (13/28) 21% (3/14) Success with soft wires 43% (40/94ε) 57% (12/21) 51% (20/39*) 24% (5/21Δ) 23% (3/13γ) Additional success with intermediate wires 37% (15/41) 60% (3/5) 54% (7/13) 33% (5/15) 0% (0/8) Additional success with stiff wires 19% (5/27) 66% (2/3) 0% (0/7) 17% (3/10) 0% (0/7) *3/42 lesions were treated immediately with an intermediate stiff wire; Δ7/28 lesions were treated immediately with an intermediate stiff wire; γ1/14 lesions was treated with immediately with a stiff wire; εIn total 11 lesions were not treated with a soft wire. Intecc Co.) and the Progress®-family (Abbott Vascular)), allowing operators to get familiar with a limited set of wires. With the use of this set of dedicated CTO-wires and the routine use of a microcatheter, this algorithm should simplify procedures. In this study, GW manipulation time was used as the endpoint for success [8]. This was done because suc- cessful GW crossing is most often the limiting factor for general procedural success. Consequently, the J-CTO scoring model was used to categorize the lesions accord- ing to difficulty [8]. The overall success rate with the applied algorithm was 77.1%, while it was possible to cross the lesion within 30 minutes in 57%. For each risk group, similar success rates are achieved for this primary endpoint (81%, 64%, 46% and 21% respectively), com- pared to those of Morino et al. (derivation set: 87.7%, 67.1%, 42.4%, 10% and validation set: 92.3%, 58.3%, 34.8%, 22.2% respectively) [8]. We routinely used a mi- crocatheter as back-up to increase wire tip load and sup- port. These results confirm that the technique works well in easy to intermediate type of CTO lesions and that for more difficult lesions, one needs different materials, techniques and experience to be successful. In 43% of all cases, soft wires were able to cross the lesion within 30 minutes, 95% of these lesions were crossed with the Fielder XT®. Moreover, when looking at the “easy” and “intermediate” lesions, a success rate of up to 57% and 51% was achieved, with the Fielder XT® capable of crossing in 92.5% and 95% of the cases re- spectively. This result is similar to the findings of Fujino et al. [10]. They reported a success rate of 37% for pa- tients treated only with a single soft wire (Fielder XT®/XT-R®). However, general success in all types of lesions was used as endpoint in this study. Besides this, Galassi et al. reported a slightly lower success rate (29.2% vs. 43%). 36% of these were successfully crossed with a Fielder XT®, which is clearly lower than in our study, due to different lesion selection [9]. 5. CONCLUSION From the results of this study, using a step-up algorithm, in which a pre-defined set of new generation CTO- dedicated wires is used, high success rates in easy and intermediate type of lesions can be obtained. In particular the use of a Fielder XT® as a wire of first choice simpli- fies the procedure. The additional benefit is the overall limited number of wires, fluoroscopy, contrast, proce- dure time and radiation, reducing costs and increasing safety. We therefore strongly encourage less experienced and intermediate volume operators/centers to follow a treatment algorithm, in which a select set of CTO- dedicated guidewires is used, to get familiar with. The presented algorithm can serve as a guideline for this, especially in the case of so called easy CTOs and those of intermediate difficulty. For more difficult lesions (i.e. J-CTO score of 3), which are less easy to deal with, an onward referral to an expert CTO center should be con- sidered. REFERENCES [1] Arslan, U., Balcioglu, A.S., Timurkaynak, T. and Cengel, A. (2006) The clinical outcomes of percutaneous coro- nary intervention in chronic total coronary occlusion. In- ternational Heart Journal, 47, 811-819. [2] Godino, C., Bassanelli, G., Economou, F.I., Takagi, K., Ancona, M., Galaverna, S., et al. (2013) Predictors of cardiac death in patients with coronary chronic total oc- clusion not revascularized by PCI. International Journal of Cardiology, 168, 1402-1409. http://dx.doi.org/10.1016/j.ijcard.2012.12.044 [3] Fefer, P., Knudtson, M.L., Cheema, A.N., Galbraith, P.D., Osherov, A.B., Yalonetsky, S., et al. (2012) Current per- spectives on coronary chronic total occlusions: The Ca- nadian Multicenter Chronic Total Occlusions Registry. Journal of the American College of Cardiology, 59, 991- 997. http://dx.doi.org/10.1016/j.jacc.2011.12.007 [4] Rathore, S., Katoh, O., Matsuo, H., Terashima, M., Ta- naka, N., Kinoshita, Y., et al. (2009) Retrograde percuta- neous recanalization of chronic total occlusion of the coronary arteries: Procedural outcomes and predictors of success in contemporary practice. Circulation: Cardio- vascular Interventions, 2, 124-132. http://dx.doi.org/10.1161/CIRCINTERVENTIONS.108.8 38862 [5] Borgia, F., Viceconte, N., Ali, O., Stuart-Buttle, C., Saraswathyamma, A., Parisi, R., et al. (2012) Improved cardiac survival, freedom from MACE and angina-related Copyright © 2013 SciRes. OPEN ACCESS  J. Maeremans et al. / World Journal of Cardiovascular Diseases 3 (2013) 536-542 542 quality of life after successful percutaneous recanaliza- tion of coronary artery chronic total occlusions. Interna- tional Journal of Cardiology, 161, 31-38. http://dx.doi.org/10.1016/j.ijcard.2011.04.023 [6] Suero, J.A., Marso, S.P., Jones, P.G., Laster, S.B., Huber, K.C., Giorgi, L.V., et al. (2001) Procedural outcomes and long-term survival among patients undergoing percuta- neous coronary intervention of a chronic total occlusion in native coronary arteries: A 20-year experience. Journal of the American College of Cardiology, 38, 409-414. [7] Khan, M.F., Wendel, C.S., Thai, H.M. and Movahed, M.R. (2013) Effects of percutaneous revascularization of chronic total occlusions on clinical outcomes: A meta- analysis comparing successful versus failed percutaneous intervention for chronic total occlusion. Catheterization and Cardiovascular Interventions, 82, 95-107. http://dx.doi.org/10.1002/ccd.24863 [8] Morino, Y., Abe, M., Morimoto, T., Kimura, T., Hayashi, Y., Muramatsu, T., et al. (2011) Predicting successful guidewire crossing through chronic total occlusion of na- tive coronary lesions within 30 minutes: The J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC: Cardiovascular interventions, 4, 213-221. http://dx.doi.org/10.1016/j.jcin.2010.09.024 [9] Galassi, A., Tomasello, S., Reifart, N., Werner, G., Sianos, G., Bonnier, H., et al. (2011) In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. Eurointer- vention, 7, 472-479. http://dx.doi.org/10.4244/EIJV7I4A77 [10] Fujino, A., Sakamoto, H., Fujino, M., Yamane, T., Adachi, T., Jinnai, T., et al. (2012) The procedural benefit of soft and tapered tip guidewire use as a first choice for chronic total occlusion revascularisation. Journal of the American College of Cardiology, 59, E106. http://dx.doi.org/10.1016/S0735-1097(12)60107-7 [11] Di Mario, C., Werner, G.S., Sianos, G., Galassi, A.R., Buttner, J., Dudek, D., et al. (2007) European perspective in the recanalisation of Chronic Total Occlusions (CTO): Consensus document from the EuroCTO Club. Euro- Intervention, 3, 30-43. [12] Brilakis, E.S., Grantham, J.A., Rinfret, S., Wyman, R.M., Burke, M.N., Karmpaliotis, D., et al. (2012) A percuta- neous treatment algorithm for crossing coronary chronic total occlusions. JACC: Cardiovascular Interventions, 5, 367-379. http://dx.doi.org/10.1016/j.jcin.2012.02.006 [13] Brilakis, E.S., Grantham, J.A., Thompson, C.A., DeMartini, T.J., Prasad, A., Sandhu, G.S., et al. (2012) The retro- grade approach to coronary artery chronic total occlu- sions. Catheterization and Cardiovascular Interventions, 79, 3-19. http://dx.doi.org/10.1002/ccd.23004 Copyright © 2013 SciRes. OPEN ACCESS
|