S. B. HE, X. G. ZHU
Copyright © 2013 SciRes. ENG
369
2) Clinical manifestation
Among twelve cases, there are six patients presenting
irregular or continuous fever of unknown origin between
38.5˚C to 40.2˚C lasting for ten to forty-one days. All
twelve cases have the symptoms of nausea, vomiting,
epigastric gas pains, but only six cases have intense bel-
lyache. The physical sign of per itonitis could be detected
in seven patients, and haemic ascites is punctured out
from abdominal cavity.
Pneumatics in enteric cavity is displayed in abdo minal
X-ray plains of all the cases, besides small amounts of
gas-fluid level without obviously distended ansa intersti-
nalis can be seen in only three cases.
3) Results
All cases have to be received emergency exploratory
laparotomy. The whole mesostenium which is diffusingly
dotted with bleeding points of unequal size are thickened
and congested extensively. Among them, two cases are
taken to emergency exploratory laparotomy without ob-
vious improvement after conservative treatment in twen-
ty-four hours. Nine cases underwent partial resection of
the small intes tine du e to small int estine, while three cases
underwent open-close operation because of full length
small intestine and part of colon necrosis simultaneously
with a great quantity of haemic ascites. Five cases died
after operation in which three cases are widespread
thrombosis and two cases are liver function failure after
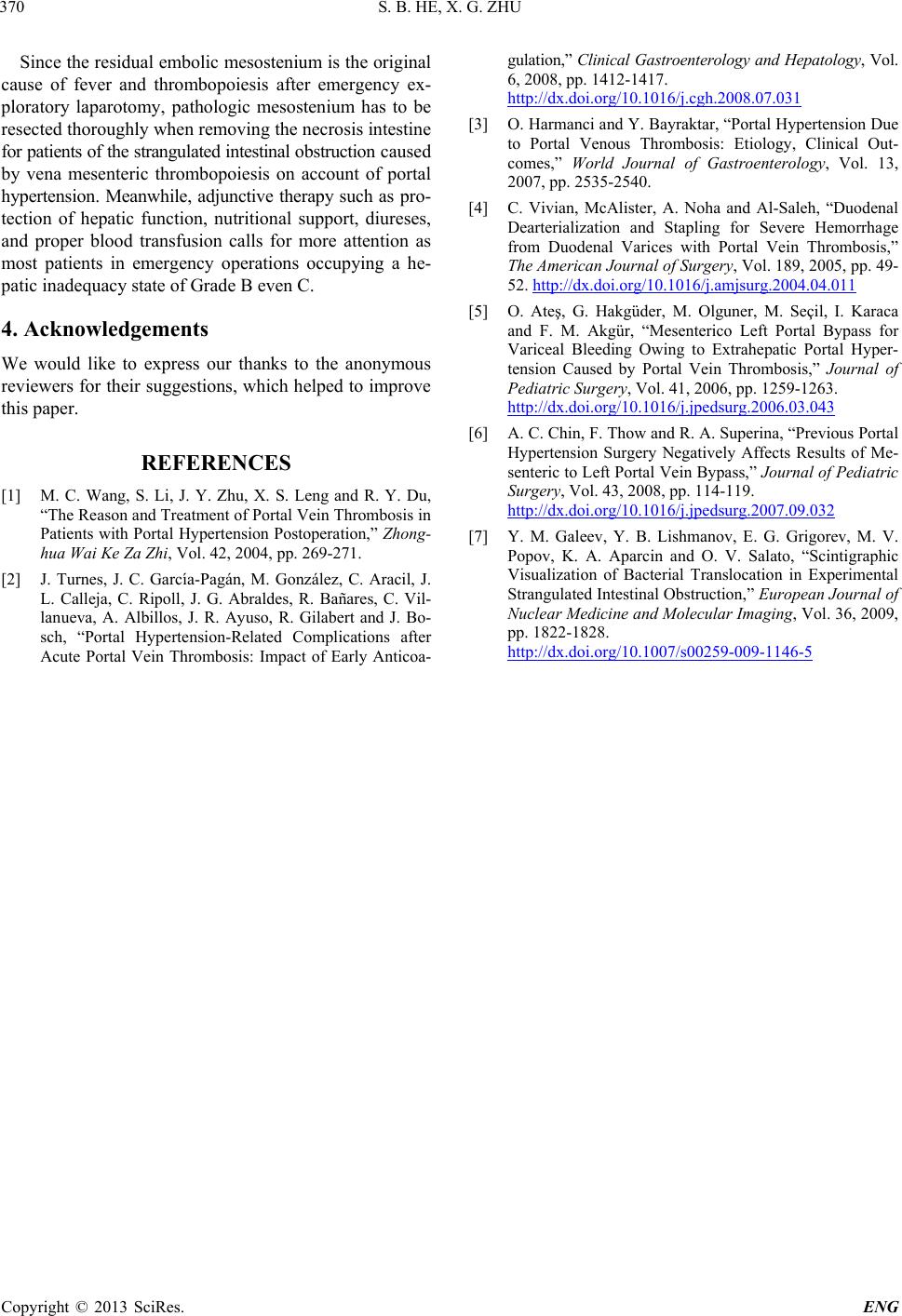
partial resection of the small intestine. Also we can get
the immunohistochemistry result of the patients after
operation (Figure 2).
3. Discussion
The venous thrombosis is concerned with lesion of vas-
Figure 2. Immunohistochemistry of mesentery vein throm-
bosis.
cular endothelial cell, adhering and assembling of plate-
lets, low serum antithrombase, and alteration of haemo-
dynamics [2,3]. Posthepatitic cirrhosis is a kind of hepat-
ic sinusoid cirrhosis, which has augmented resistance of
blood flow returning to liver resulting in hypertension in
vena mesenteric and torpidity of blood flow. Meanwhile
a bulk of fatty acid, amino acids and carbohydrate ab-
sorbed in small intestine are accumulated in mesostenium
which increase the viscosity. Chronic portal hypertension
plus ischemic and hypoxia of endothelial cells of vena
mesenteric could damage endothelial cells unavoidably.
The function of single platelet won’t be weakened, in-
stead, adhering and assembling of platelets will augment
due to the necessity of compensation in spite of the in-
creasing demolition of platelet leading by splenomegaly
and hypersplenism. In addition, patients of hepatic cirr-
hosis with low level of hepatic protein synthesis are in
the hypercoagulable state owing to the dysfunction of
antiprothrombin [4]. In a word, mesostenium in portal
system is prone to thrombopoiesis influenced by all the
factors mentioned above.
The disor der of hemorheology been secondary to throm-
bopoiesis in vena mesenteric which leads to completely
interruption of venous blood flow will result in the simi-
lar circumstance in the arterial mesenteric, and strangu-
lated intestinal obstruction will emerge ultimately [5,6].
It is different from acute volvulus with the interruption of
blood flow both in arterial and vena mesenteric simulta-
neously causing the typically manifestation such as in-
tense abdominal pain, nausea and vomiting. The symp-
tom of intense abdominal pain occurs only in seven cases
in this group, and all the others have non-specificity ma-
nifestations such as abdominal discomfort, nausea and
vomiting. Furthermore, two cases attempted to adopt con-
servative treatment before exploratory laparotomy. Thus,
the clinical manifestation of strangulated intestinal ob-
struction caused by vena mesenteric thrombopoiesis on
account of portal hypertension is so insidious that it is
difficult t o ha ve t imely and accura te diagnosis. C ontinuous
fever and general toxic symptoms with leucocytes count
of more than 20 × 109 per liter would emerge attachin g to
vena mesenteric thrombopoiesis. What’s more, ascites
even jaundice and alimentary tract hemorrhage could be
detected if infective pylephlebitis occurs in addition to
the aggravation of infective symptoms. Accordingly, it is
necessary to take ultrasound or CT scan for patients of
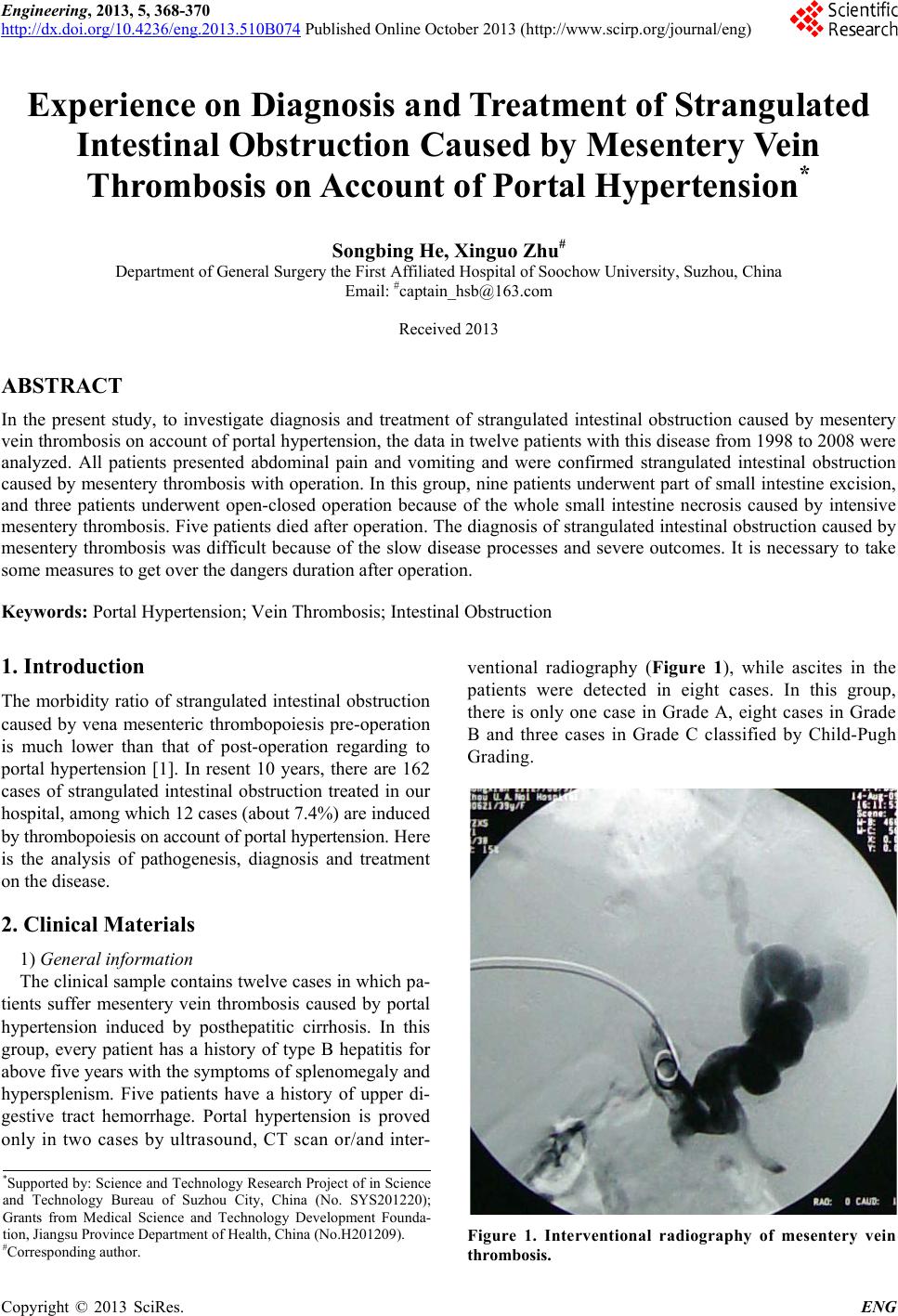
portal hypertension with the symptoms of continuous fev-
er, abdominal pain, abdominal distention, nausea and vo-
miting. Thrombopoiesis in vena mesenteric, thickened me-
sostenium, and haemic ascites can be considered as suf-
ficient indications of emergency exploratory laparotomy
[7]. Actually there are three cases in this group dying
from extensive thrombopoiesis owing to delayed diagno-
sis.