K. N’Guessan et al. / Journal of Tuberculosis Researc h 1 (2013) 40-43 41
Previous work has shown that there is a good correla-
tion between the results obtained with the QBC ParaLens
and those results obtained with classical fluorescent mi-
croscopy [5]. In some cases, the performance of LED
FM is better than conventional fluorescent microscopy
methods [5,6].
This study was designed to evaluate the QBC Para
Lens LED fluorescent microscopy attachment and the
QBC F.A.S.T. AFB staining system for the detection of
AFB in pathological specimens of suspected TB patients
in Abidjan, Côte d’Ivo ire in 20 10.
2. METHODS
2.1. Sample Collection
Patient samples were collected at the CHU Services of
Cocody, Centre Antituberculeux de Treichville and Ad-
jamé. Samples were collected from 50 patients with
symptoms suggestive of tuberculosis. The 50 samples
included 31 spontaneous sputum samples, 16 gastric as-
pirates sample, 1 bronchial aspiration sample, and 2
pleural liquid samples Table 1. Samples were then tran s-
ported at 4˚C to the Tubercu losis Laboratory at the Insti-
tute Pasteur of Cote d’Ivoire. The samples were exam-
ined for non-conformance per internal quality control
procedures and accepted for use in the study.
2.2. Direct Examination
Direct examination without concentration was per-
formed on each of the samples. Two smears were pre-
pared according to internal protocols. The first smear
was made on a common use microscope slide. The sec-
ond smear was made on a QBC F.A.S.T. SureFo cus slide.
Both smears were air-dried and fixed using flame. The
first smear was stained according to accepted procedures
with a 0.5% Carbol Fuschsin solution prepared in the
laboratory. The second smear was stained using the QBC
F.A.S.T. AFB Stain kit according to the manufacturer’s
instructions for use.
Direct examination was conducted using an Olympus
CX21 microscope. To facilitate fluorescent examination,
the QBC ParaLens fluorescent microscope attachment
with 60× objective was mounted to the nosepiece of the
same microscope.
Ziehl-Neelsen (ZN) stained smears were reviewed us-
ing a 100× objective under oil. QBC F.A.S.T. AFB fluo-
rescent stained smears were reviewed using the QBC
ParaLens with 60× objective under oil. Two technicians
conducted blinded microscope examination according to
accepted procedures for both the ZN and QBC F.A.S.T.
AFB examination techniques. Discordant results were
reviewed by a third, more experienced technician. Direct
examination results were quantified using the WHO
scale [7].
2.3. Culture
Each of the samples was also cultured according to
accepted procedures. Samples were decontaminated us-
ing a 2% N-Acetyl-L-Cysteine (NALC) solution and
incubating for 15 minutes. After incubation, the samples
were centrifuged at 3000 × g for 20 minutes. The super-
natant was removed and the pellet re-suspended in a
phosphate suspension buffer (pH 7). The solution was
homogenized by aspiration. Each sample was used to
inoculate three cultures of Lowenstein-Jensen (LJ) media.
The inoculants were incubated at 37˚C for eight weeks.
After incubation, all positive LJ cultures were tested us-
ing an Immunochromatographic (SD BioLine) test for
detection of antigen MPT 64. Data was collected and
analyzed using Epi-Info 6.04 (CDC, Atlanta, GA, USA).
3. RESULTS
Direct examination of ZN stained specimens resulted
in 40%; 95% C.I. [0.26 - 0.54] % (20 of 5 0 samples) posi-
tive incidence rate. When LED fluorescent microscopy
was used to examine the specimens stained with the
QBC F.A.S.T. AFB stain, a 42%; 95% C.I. [0.28 - 0.56]%
(21 of 50 samples) positive incident rate was seen (Table
2).
Of the samples examined, positive results were ob-
served using ZN stain in 16 spontaneous sputum sam-
ples, 3 gastric aspirates and 1 liquid bronchial aspiration.
LED fluorescent microscopy with QBC F.A.S.T. AFB
stain resulted in positive samples being observed in 17
spontaneous sputum samples, 3 gastric aspirates and 1
liquid bronchial aspiration. The MPT 64 antigen detec-
tion method identified 18 positive cases and 1 strongly
suggestive suspected case.
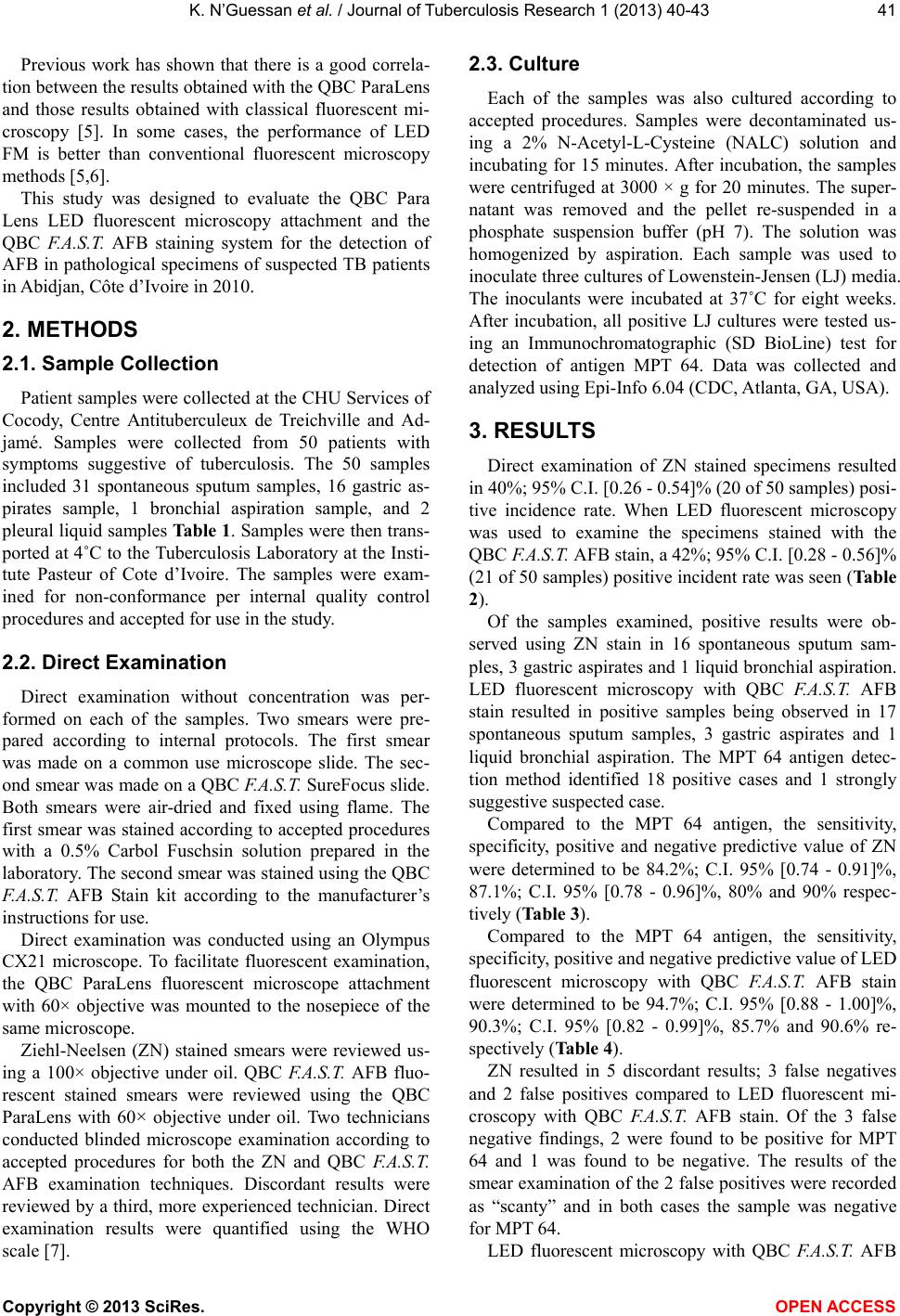
Compared to the MPT 64 antigen, the sensitivity,
specificity, positive and negative predictive value of ZN
were determined to be 84.2%; C.I. 95% [0.74 - 0.91]%,
87.1%; C.I. 95% [0.78 - 0.96]%, 80% and 90% respec-
tively (Table 3).
Compared to the MPT 64 antigen, the sensitivity,
specificity, positive and negative predictive value of LED
fluorescent microscopy with QBC F.A.S.T. AFB stain
were determined to be 94.7%; C.I. 95% [0.88 - 1.00]%,
90.3%; C.I. 95% [0.82 - 0.99]%, 85.7% and 90.6% re-
spectively (Table 4).
ZN resulted in 5 discordant results; 3 false negatives
and 2 false positives compared to LED fluorescent mi-
croscopy with QBC F.A.S.T. AFB stain. Of the 3 false
negative findings, 2 were found to be positive for MPT
64 and 1 was found to be negative. The results of the
smear examination of the 2 false positives were recorded
as “scanty” and in both cases the sample was negative
for MPT 64.
LED fluorescent microscopy with QBC F.A.S.T. AFB
Copyright © 2013 SciRes. OPEN A CCESS