Vol.1, No.3, 37-39 (2013) Journal of Tubercul osis Resear ch
http://dx.doi.org/10.4236/jtr.2013.13007
Appendicular tuberculosis presenting as
enterocutaneous fistula over thigh—A rare case
report with review of literature
Vaibhav Pandey*, Ajay Narayan Gangopadhyay, Shiv Prasad Sharma, Vijayndar Kumar
Department of Pa e d ia t r ic Surgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India;
*Corresponding Author: sunny.imsbhu@gmail.com
Received 23 July 2013; revised 11 September 2013; accepted 24 September 2013
Copyright © 2013 Vaibhav Pandey et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Abdominal tuberculosis is a significant cause of
morbidity and mort ality in children in developing
countries. Primary involvement of appendix is
very rare. Presentation is usually non specific
and diagnosis is made in most cases on histo-
pathlogical examination following appendicec-
tomy. This to our knowledge is the first case of
appendicular tuberculosis presenting primarily
as spontaneous enterocutaneous fistula over
front of right thigh. Barium meal follow-through
was diagnostic. Appendicectomy was perform-
ed followed by anti-tubercular treatment which
was curative.
Keyw ords: Tubercular Appendicitis; Abdominal
Tuberculosis; Enterocutaneous Fistula
1. INTRODUCTION
Abdominal tuberculosis continues to be a significant
cause of morbidity and mortality in children in develop-
ing countries. Ileocaecal region is most common site of
involvement and accoun ts for 75% of the gastrointestinal
tuberculosis; primary involvement of appendix is very
rare and accounts for only 0.6% to 2.9% [1]. Here we
report a case of primary appendicular tuberculosis in a
child presented with enterocutaneous fistula in front up-
per part of right thigh.
2. CASE REPORT
A 4-year-old female child presented with pain com-
plaints of pain and swelling over front of right thigh as-
sociated with high grade fever. A diagnosis of a suppura-
tive abscess was made and incision and drainage was
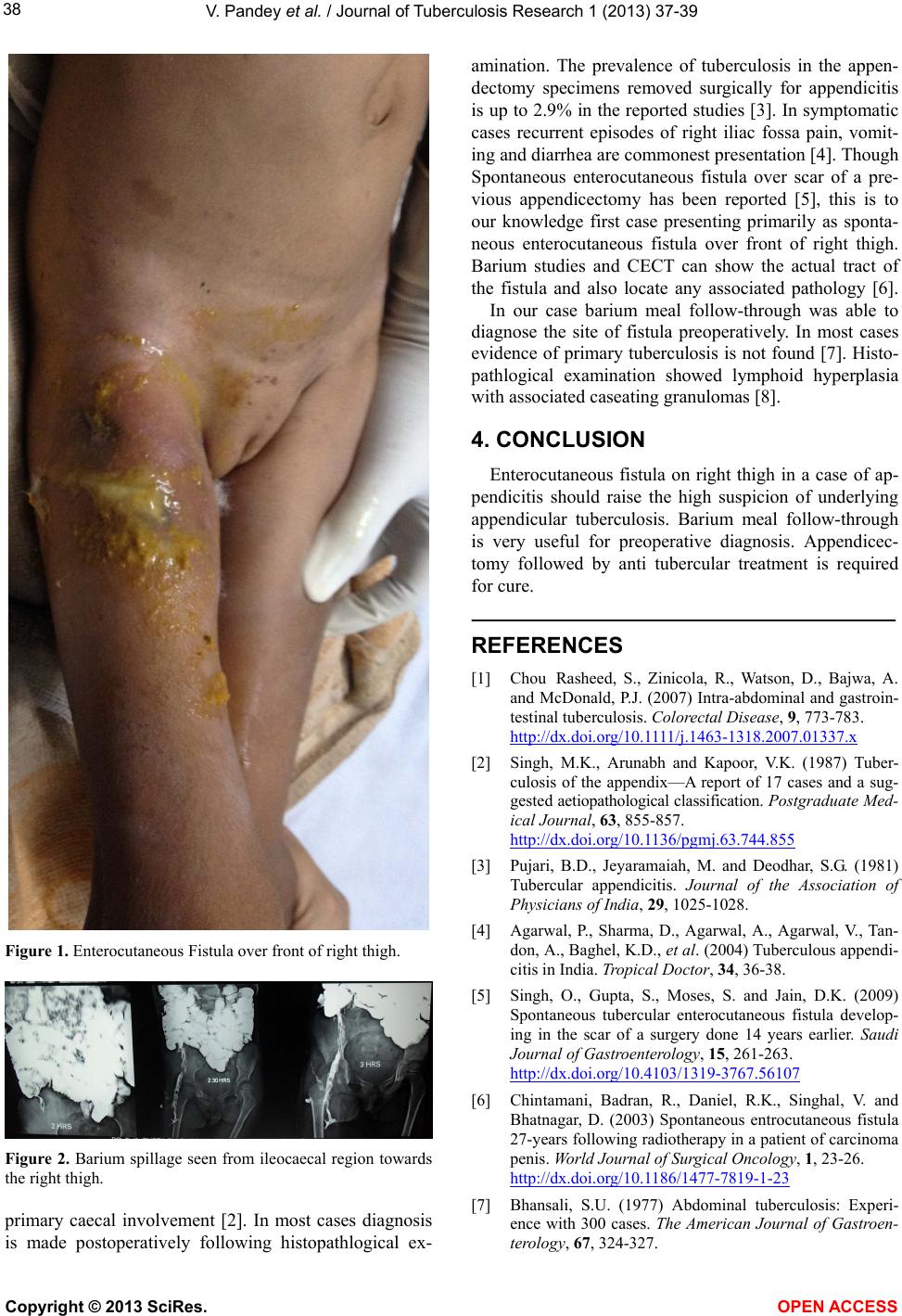
done outside, following which she developed fecal dis-
charge from the incision site (Figure 1). Patient had also
mild pain in right iliac fossa. On examination there was
guarding and mild tenderness in the right iliac fossa. Ul-
trasonogram of abdomen showed localized collection in
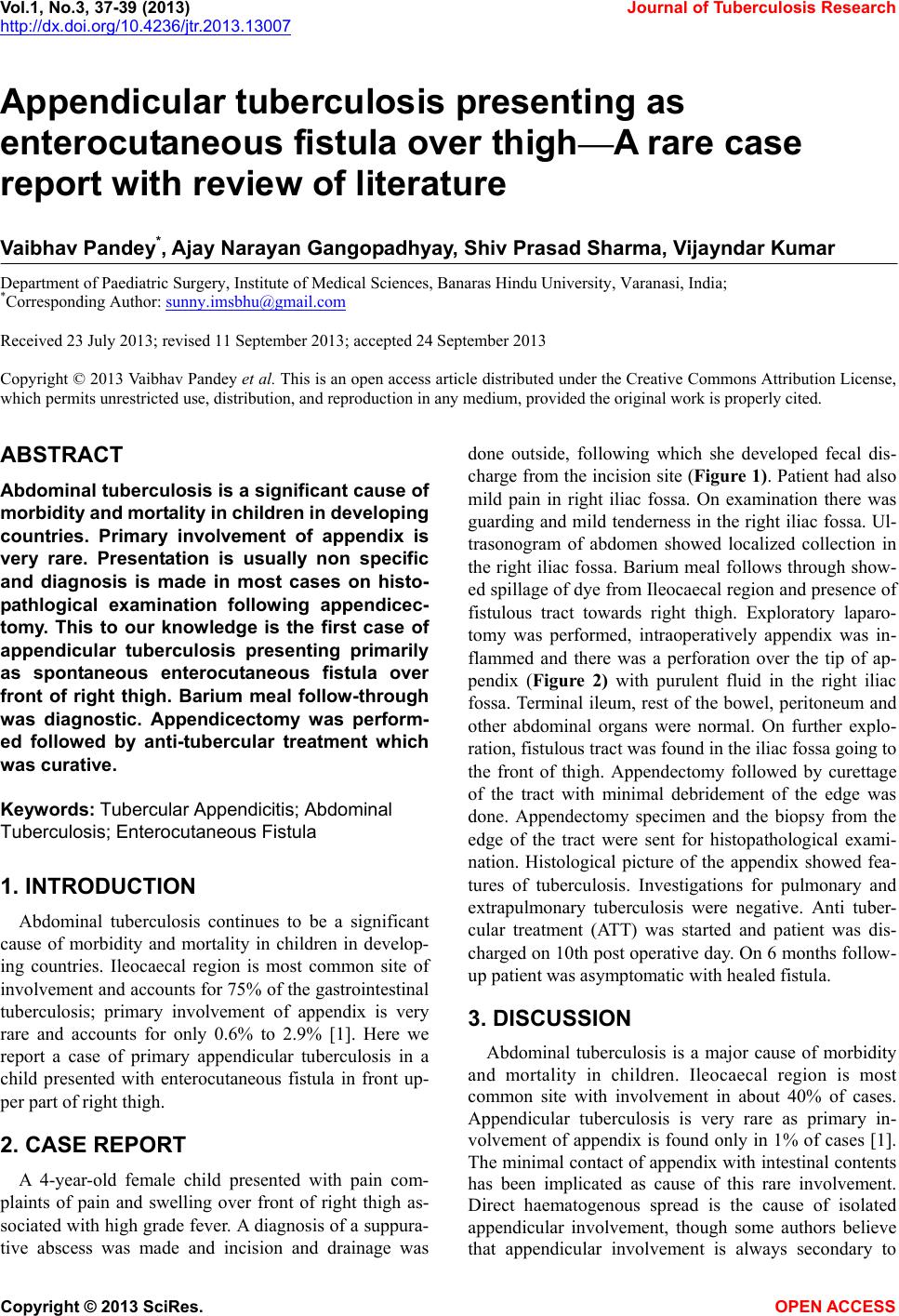
the right iliac fossa. Barium meal follows through show-
ed spillage of dye from Ileocaecal region and presence of
fistulous tract towards right thigh. Exploratory laparo-
tomy was performed, intraoperatively appendix was in-
flammed and there was a perforation over the tip of ap-
pendix (Figure 2) with purulent fluid in the right iliac
fossa. Terminal ileum, rest of the bowel, peritoneum and
other abdominal organs were normal. On further explo-
ration, fistulous tract was found in the iliac fossa going to
the front of thigh. Appendectomy followed by curettage
of the tract with minimal debridement of the edge was
done. Appendectomy specimen and the biopsy from the
edge of the tract were sent for histopathological exami-
nation. Histological picture of the appendix showed fea-
tures of tuberculosis. Investigations for pulmonary and
extrapulmonary tuberculosis were negative. Anti tuber-
cular treatment (ATT) was started and patient was dis-
charged on 10th post operative day. On 6 months fo llow-
up patient w as asymptomatic with healed fistula.
3. DISCUSSION
Abdominal tuberculosis is a major cause of morbidity
and mortality in children. Ileocaecal region is most
common site with involvement in about 40% of cases.
Appendicular tuberculosis is very rare as primary in-
volvement of appendix is found only in 1% of cases [1].
The minimal contact of appendix with intestinal contents
has been implicated as cause of this rare involvement.
Direct haematogenous spread is the cause of isolated
appendicular involvement, though some authors believe
that appendicular involvement is always secondary to
Copyright © 2013 SciRes. OPEN A CCESS