Neuroscience & Medicine, 2013, 4, 267-270
Published Online December 2013 (http://www.scirp.org/journal/nm)
http://dx.doi.org/10.4236/nm.2013.44038
Open Access NM
267
Benign Fibrous Histiocytoma of the Neurocranium
Chrisovalantis A. Tsimiklis*, Tom Morris
Neurosurgical Department, Royal Adelaide Hospital (RAH), North Terrace, Adelaide, Australian
Email: *ctsimiklis29@gmail.com, dr.t ommorris@gmail.com
Received October 8th, 2013; revised November 5th, 2013; accepted December 3rd, 2013
Copyright © 2013 Chrisovalantis A. Tsimiklis, Tom Morris. This is an open access article distributed under the Creative Commons
Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
ABSTRACT
Presented is a case of benign fibrous histiocytoma (BFH) involving the calvarium of a 25 years old lady who noticed a
depression in her occiput associated with localised pain. Imaging revealed a tumour eroding through the inn er and outer
skull tables, closely associated with major underlying dural sinuses. She underwent complete macroscopic resection of
the tumour and reconstru ction of a titanium mesh craniop lasty. Histology favoured a benign process with a diagnosis of
BFH of the calvarium given. At 1 year follow-up, the patient is asymptomatic and has not developed recurrence of the
tumour.
Keywords: Benign Fibrous Histiocytoma; Skull Tumour; Neurocranium
1. Introduction
BFH is most often encountered as a soft-tissue neoplasm
involving the skin, and although less common, BFH in-
volving other sites including the bony skeleton is seen.
Involvement of the skull is particularly rare with only
one other case of BFH involving the neurocranium re-
ported in the literature [1]. Here we report a case of a
symptomatic BFH involving the occipital bone and dis-
cuss the role for minimising the degree of resection in
these benign ca ses.
2. Case Report
Presentation and examination. A bump was first noted
by this 25 years old lady on her occiput 18 months prior
to presentation. It was steadily increasing over this period
and she had associated pain at the site but was otherwise
neurologically intact. There were no overlying changes
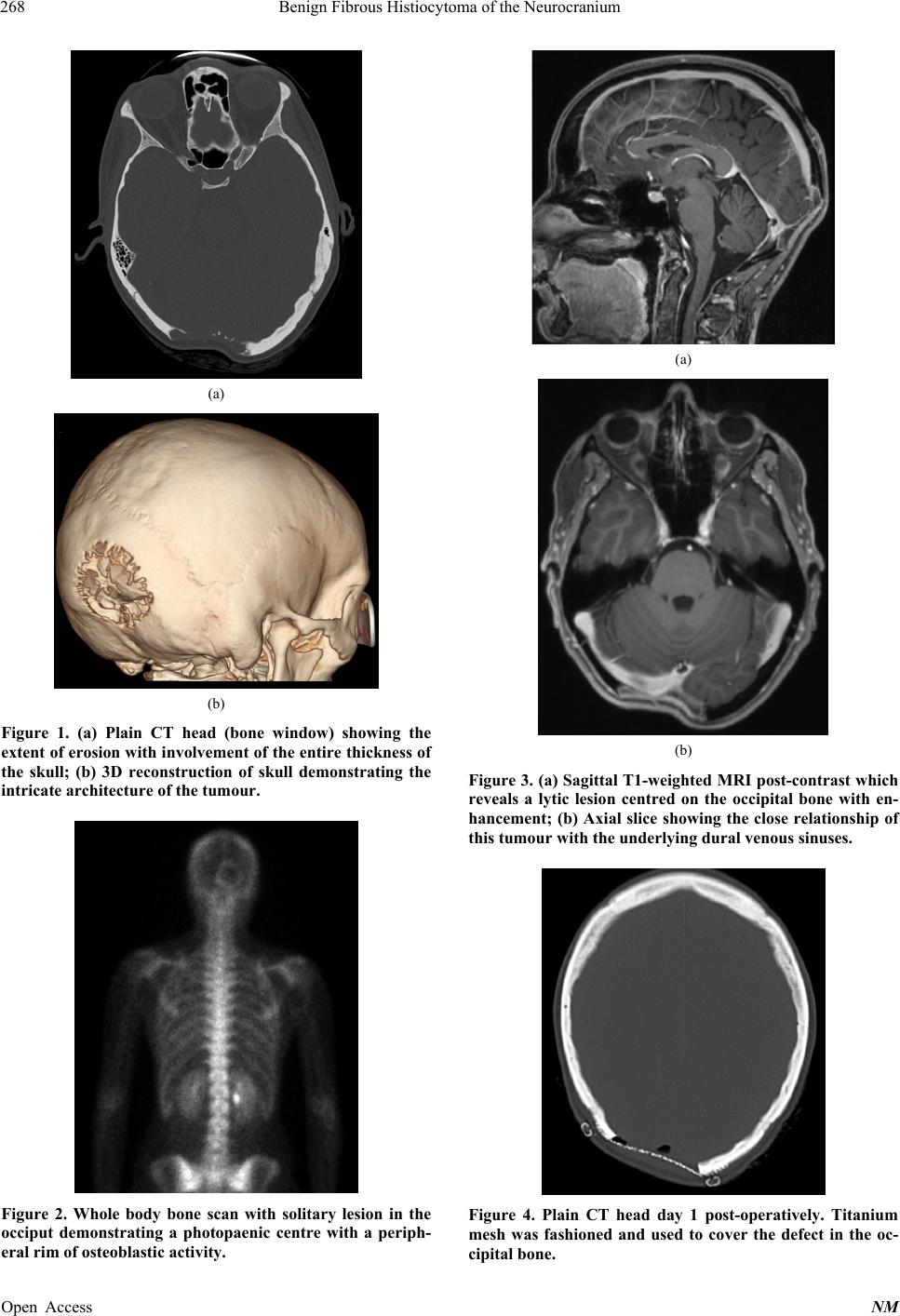
to the scalp tissue itself. A CT head revealed an expansile
lytic process to the right of the midline invo lving the oc-
cipital bone, measuring 40 × 45 mm, and resulting in loss
of both the inner and outer tables of the skull (Figures
1(a) and (b)). A bone scan showed a solitary photo-
paenic occipital bone lesion with a peripheral rim of os-
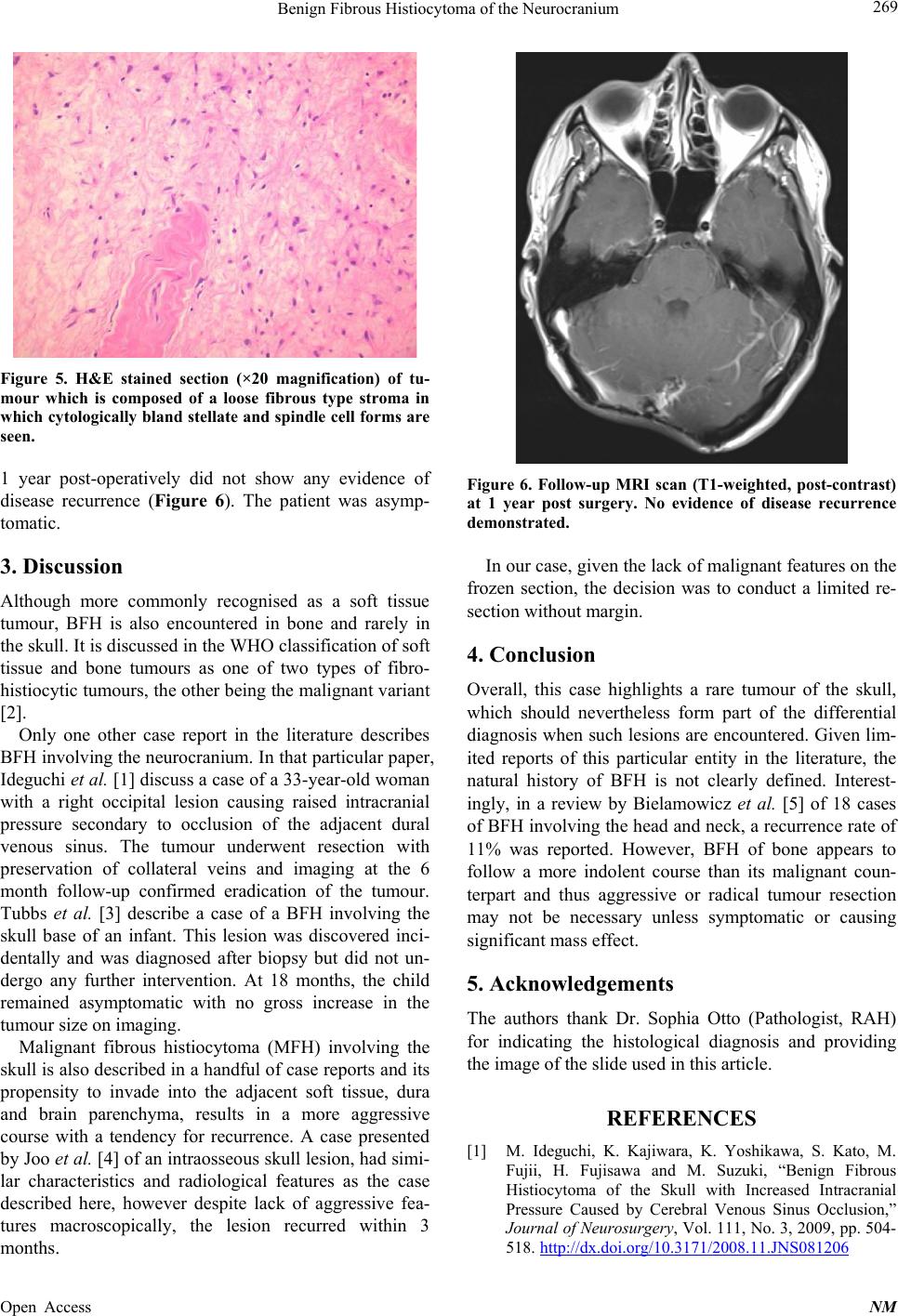
teoblastic activity (Figure 2). On MRI there was a lytic
process following CSF signal with peripheral enhance-
ment (Figures 3(a) and (b)). There was no invasion into
brain parenchyma but it was closely associated with ma-
jor underlying dural sinuses. The main differential diag-
nosis was of an eosiniphilic granuloma.
Operation and Postoperative Course. The patient un-
derwent craniotomy and resection of the tumour. The
macroscopic finding intra-operatively was of a pale rub-
bery mass eroding through the entire thickness of the
occipital bone. Frozen section did not provide a clear
diagnosis but there were no necrotic features or obvious
mitoses. The bone edges were drilled back to normal
appearing skull. The mass was carefully dissected off the
underlying torcula and dura. Gross total resection was
achieved. Titanium mesh was fashioned to cover the
bony defect followed by primary wound closure (Figure
4). Her post-operative course was uneventful.
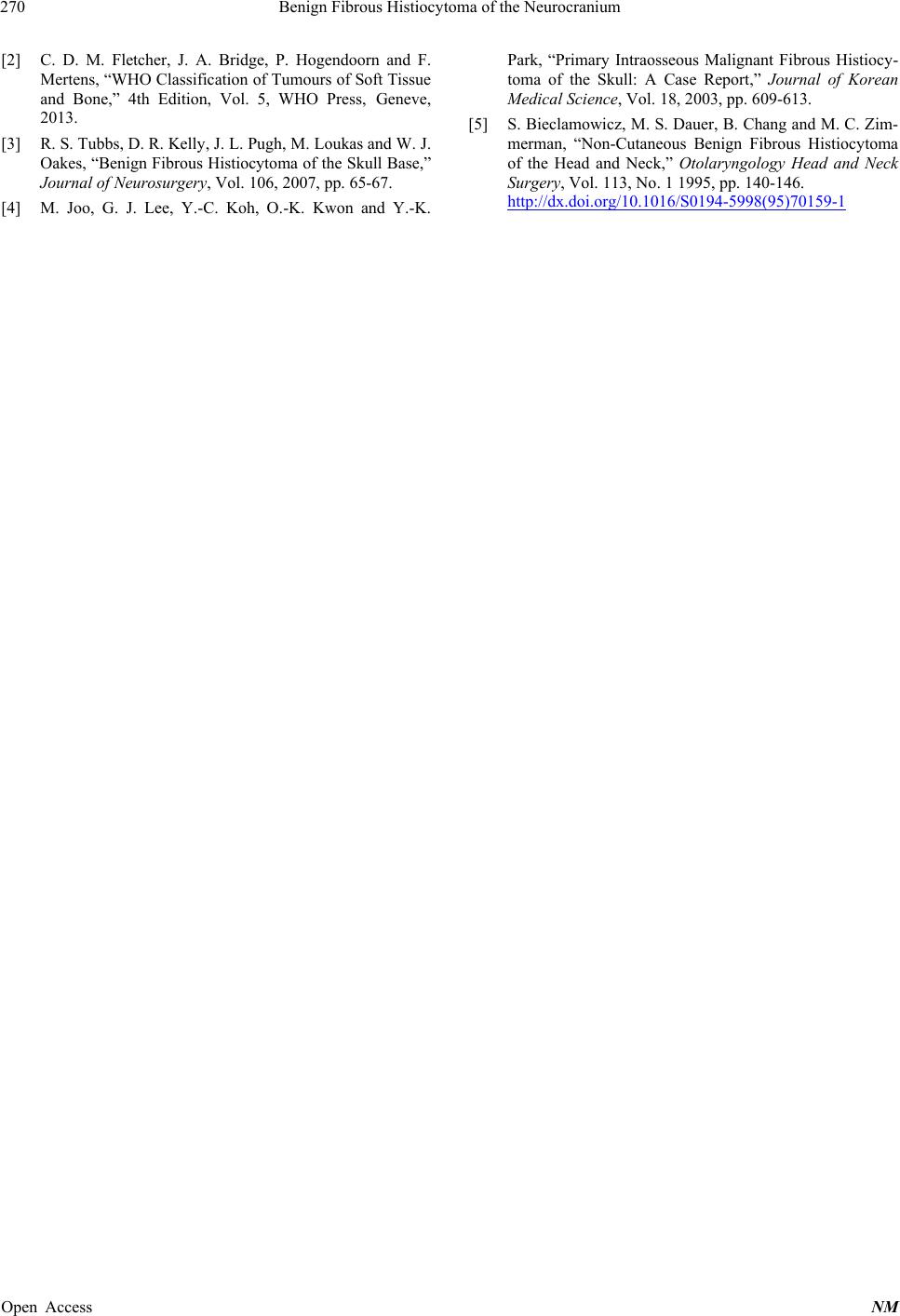
On histological examination, the tissue revealed spin-
dle cell proliferation, with fibromyxoid appearance
(Figure 5). Some of the spindle cells showed a level of
nuclear hyperchromasia, but mitoses were not readily
identified, and there was no evidence of necrosis. Im-
munohistochemistry revealed positive immunostaining
for SMA, but negativity for S100, CD34, AE1/3, GFAP,
EMA and desmin. An expert opinion was sought and it
was felt that the most likely diagnosis was that of b enign
fibrous histiocytoma of the calv arium.
No further adjuvant treatment was necessary. An MRI
*Corresponding a uthor.