M. RASKE, D. HULSE 301
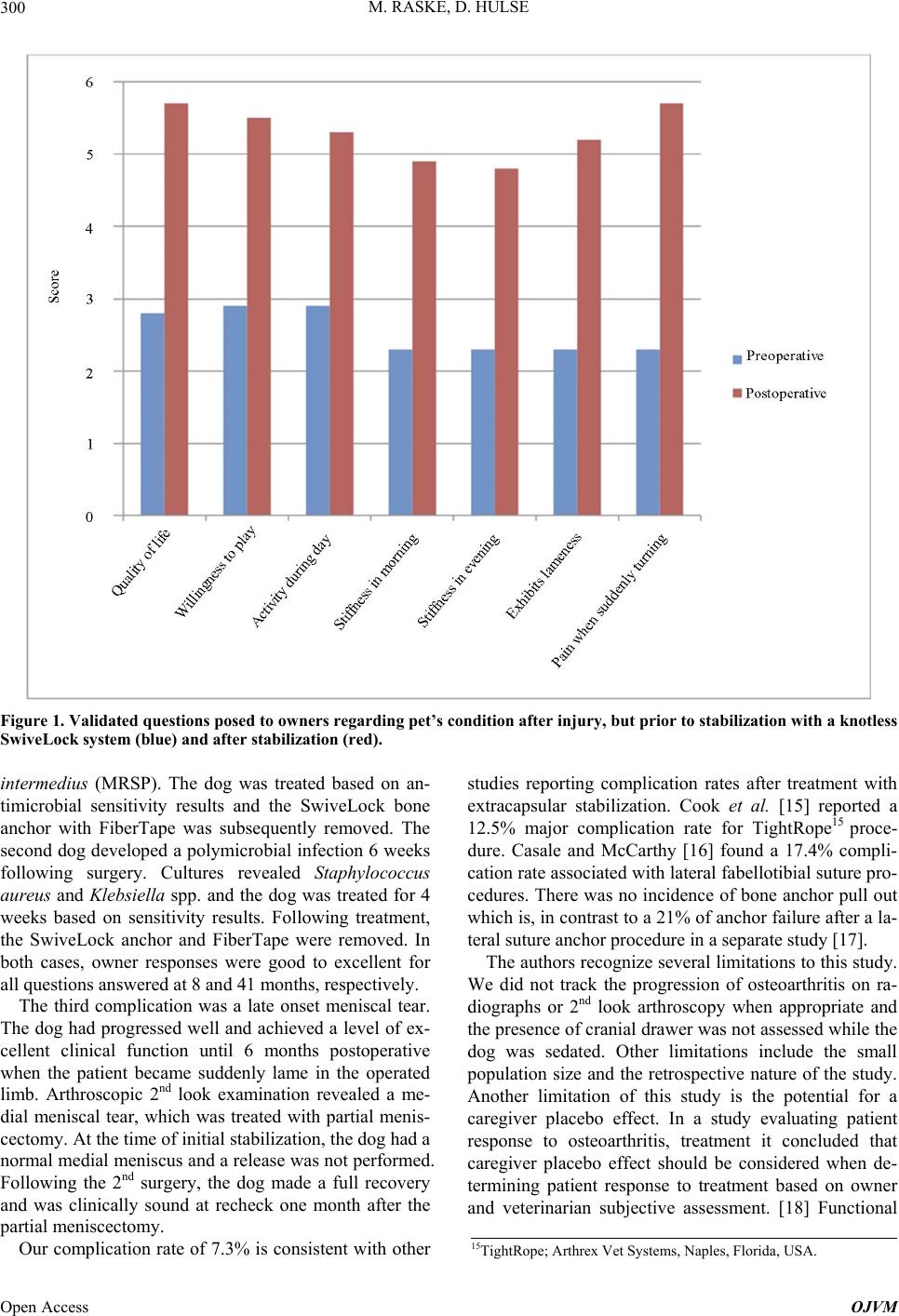
outcome was based on a subjective, client answered ques-
tionnaire. The questionnaire has been found to be repea-
table and valid for assessing lameness in dogs. [6]
5. Conclusion
The knotless SwiveLock bone anchor preloaded with 2
mm FiberTape provides good to excellent long-term cli-
nical function outcomes and a low complication rate in
dogs treated for CCL deficient stifles.
6. Acknowledgements
We would like to thank Dr. Abigail D. Mariano for as-
sistance with statistical analysis.
REFERENCES
[1] D. L. Piermattei, F. L. Gretchen and C. E. DeCamp, “The
Stifle Joint,” In: D. L. Piermattei, F. L. Gretchen and C. E.
DeCamp, Eds., Brinker, Piermattei, and Flo’s Handbook
of Small Animal Orthopedics and Fracture Repair, Else-
vier Inc., St. Louis, 2006, pp. 562-632.
[2] J. L. Cook, “Extracapsular Stabilization,” In: P. Muir, Ed.,
Advances in the Canine Cranial Cruciate Ligament, Wi-
ley-Blackwell, Hoboken, 2010, pp. 163-167.
[3] S. E. Kim, A. Pozzi, M. P. Kowaleski, et al., “Tibial Os-
teotomies for Cranial Cruciate Ligament Insufficiency in
Dogs,” Veterinary Surgery, Vol. 37, No. 2, 2008, pp. 111-
125. http://dx.doi.org/10.1111/j.1532-950X.2007.00361.x
[4] H. S. Mullen and D. T. Matthiesen, “Complications of
Transposition of the Fibular Head for Stabilization of the
Cranial Cruciate-Deficient Stifle in Dogs: 80 Cases (1982-
1986),” Journal of the American Animal Hospital Asso-
ciation, Vol. 195, No. 9, 1989, pp. 1267-1271.
[5] D. Hulse, W. Hyman, B. Beale, et al., “Determination of
Isometric Points for Placement of a Lateral Suture in
Treatment of the Cranial Cruciate Ligament Deficient
Stifle,” Veterinary and Comparative Orthopaedics and
Traumatology, Vol. 23, No. 3, 2010, pp. 163-167.
[6] D. Hulse, B. Saunders, B. Beale, et al., “Extra-Articular
Stabilization of the Cranial Cruciate Deficient Stifle with
Anchor Systems,” Tierärztliche Praxis Kleintiere, Vol.
39, No. 5, 2011, pp. 363-367.
[7] J. T. Hudson, M. R. Slater, L. Taylor, et al., “Assessing
Repeat Ability and Validity of a Visual Analogue Scale
Questionnaire for Use in Assessing Pain and Lameness in
Dogs,” American Journal of Veterinary Research, Vol.
65, No. 12, 2004, pp. 1634-1643.
http://dx.doi.org/10.2460/ajvr.2004.65.1634
[8] C. J. Choate, A. Pozzi, D. D. Lewis, et al., “Mechanical
Comparison of Lateral Circumfabellar Suture, Tightrope
ccl, and Swivelock Bone Anchor for Extracapsular Stabi-
lization of the Cranial Cruciate Ligament-Deficient Stifle
in Dogs,” Proceed 32nd Annual Conference of the Vet-
erinary Orthopedic Society, Snowmass, 2005, pp. 9-10.
[9] S. Eugster, P. Schawalder, F. Gaschen, et al., “A Pro-
spective Study of Postoperative Surgical Site Infections in
Dogs and Cats,” Veterinary Surgery, Vol. 33, No. 5, 2004,
pp. 542-550.
http://dx.doi.org/10.1111/j.1532-950X.2004.04076.x
[10] T. N. Frey, M. G. Hoelzler, T. D. Scavelli, et al., “Risk
Factors for Surgical Site Infection-Inflammation in Dogs
Undergoing Surgery for Rupture of the Cranial Cruciate
Ligament: 902 Cases (2005-2006),” Journal of the Ame-
rican Veterinary Medical Association, Vol. 236, No. 1,
2010, pp. 88-94.
http://dx.doi.org/10.2460/javma.236.1.88
[11] P. B. Vasseur, J. Levy, E. Dowd, et al., “Surgical Wound
Infection Rates in Dogs and Cats Data from a Teaching
Hospital,” Veterinary Surgery, Vol. 17, No. 2, 1988, pp.
60-64.
http://dx.doi.org/10.1111/j.1532-950X.1988.tb00278.x
[12] L. J. Owen, J. A. Gines, T. G. Knowles, et al., “Efficacy
of Adhesive Incise Drapes in Preventing Bacterial Con-
tamination of Clean Canine Surgical Wounds,” Veterina-
ry Surgery, Vol. 38, No. 6, 2009, pp. 732-737.
http://dx.doi.org/10.1111/j.1532-950X.2009.00537.x
[13] N. D. Rose, D. Goerke, R. B. Evans, et al., “Mechanical
Testing of Orthopedic Suture Material Used for Extra-
Articular Stabilization of Canine Cruciate-Ligament Defi-
cient Stifles,” Veterinary Surgery, Vol. 41, No. 2, 2012,
pp. 266-272.
[14] M. L. Dulisch, “Suture Reaction Following Extra-Ar-
ticular Stifle Stabilization in the Dog—Part I: A Retro-
spective Study of 161 Stifles,” Journal of the American
Veterinary Medical Association, Vol. 17, 1981, pp. 569-
571.
[15] J. L. Cook, J. K. Luther, J. Beetem, et al., “Clinical
Comparison of a Novel Extracapsular Stabilization Pro-
cedure and Tibial Plateau Leveling Osteotomy for Treat-
ment of Cranial Cruciate Ligament Deficiency in Dogs,”
Veterinary Surgery, Vol. 39, No. 3, 2010, pp. 315-323.
http://dx.doi.org/10.1111/j.1532-950X.2010.00658.x
[16] S. A. Casale and R. J. McCarthy, “Complications Associ-
ated with Lateral Fabellotibial Suture Surgery for Cranial
Cruciate Ligament Injury in Dogs: 363 Cases (1997-
2005),” Journal of the American Veterinary Medical As-
sociation, Vol. 234, No. 2, 2009, pp. 229-235.
[17] L. Guenego, A. Zahara, A. Madelenat, et al., “Cranial Cru-
ciate Ligament Rupture in Large and Giant Dogs. A ret-
rospective Evaluation of a Modified Lateral Extracapsular
Stabilization,” Veterinary and Comparative Orthopaedics
and Traumatology, Vol. 20, No. 1, 2007, pp. 43-50.
[18] M. G. Conzemius and R. B. Evans, “Caregiver Placebo
Effect for Dogs with Lameness from Osteoarthritis,” Jour-
nal of the American Veterinary Medical Association, Vol.
241, No. 10, 2012, pp. 1314-1319.
http://dx.doi.org/10.2460/javma.241.10.1314
Open Access OJVM