A. CASTRO-LARA ET AL.
past research has shown that, in Chile, these depression risk and
treatment access gaps between women and men are greater than
in European countries. Nevertheless, it is probable that, in addi-
tion to the aforementioned points, this difference is explained
by the barriers men face to access treatment, due to the health
centers’ hours of operation.
The study sample is clinically complex, with depressive epi-
sodes accompanied by suicide risk, comorbid anxiety disorders,
significant associated disability, and a previous history of de-
pression. Upon comparison to the 2011 study by Alvarado et al.,
which evaluated the national depression program in urban pri-
mary care clinics (Alvarado & Rojas, 2011), the sample from
this study, treated in rural community hospitals, had a higher
percentage of severe depression, a finding which should be
taken into account when designing methodologies to optimize
depression treatment for this particular population.
It is likely that in more rural zones, where these community
hospitals are located, patients face obstacles to access special-
ized treatment, given that two known treatment barriers are
distance and cost considerations (Luo & Wang, 2003; Men-
donza-Sassi & Béria, 2001; Rosenberg, 1998).
Only 24.4% of patients in the sample did not present suicide
risk. A study carried out by Escobar and Rojas found that 2.6%
of the 2008-2009 discharges from a rural hospital were patients
with suicidal behavior, approximately 70% of whom were
women. In addition, close to 60% of the patients had a history
of psychiatric disorders, and of those, 26.5% had a previous
depressive episode. Strikingly, only 24.48% of the patients
hospitalized in the rural community hospitals were evaluated by
a specialized mental health professional (Escobar & Rojas,
2010). The high rate of attempted suicide in Chile has been
previously described (Moyano Díaz & Barría, 2006; Tomas
Baader et al., 2011). Sociopolitical explanations attribute this
phenomenon to economic indicators of increasing inequality,
job insecurity, interpersonal distrust, and weakening social
networks (Moyano Díaz & Barría, 2006).
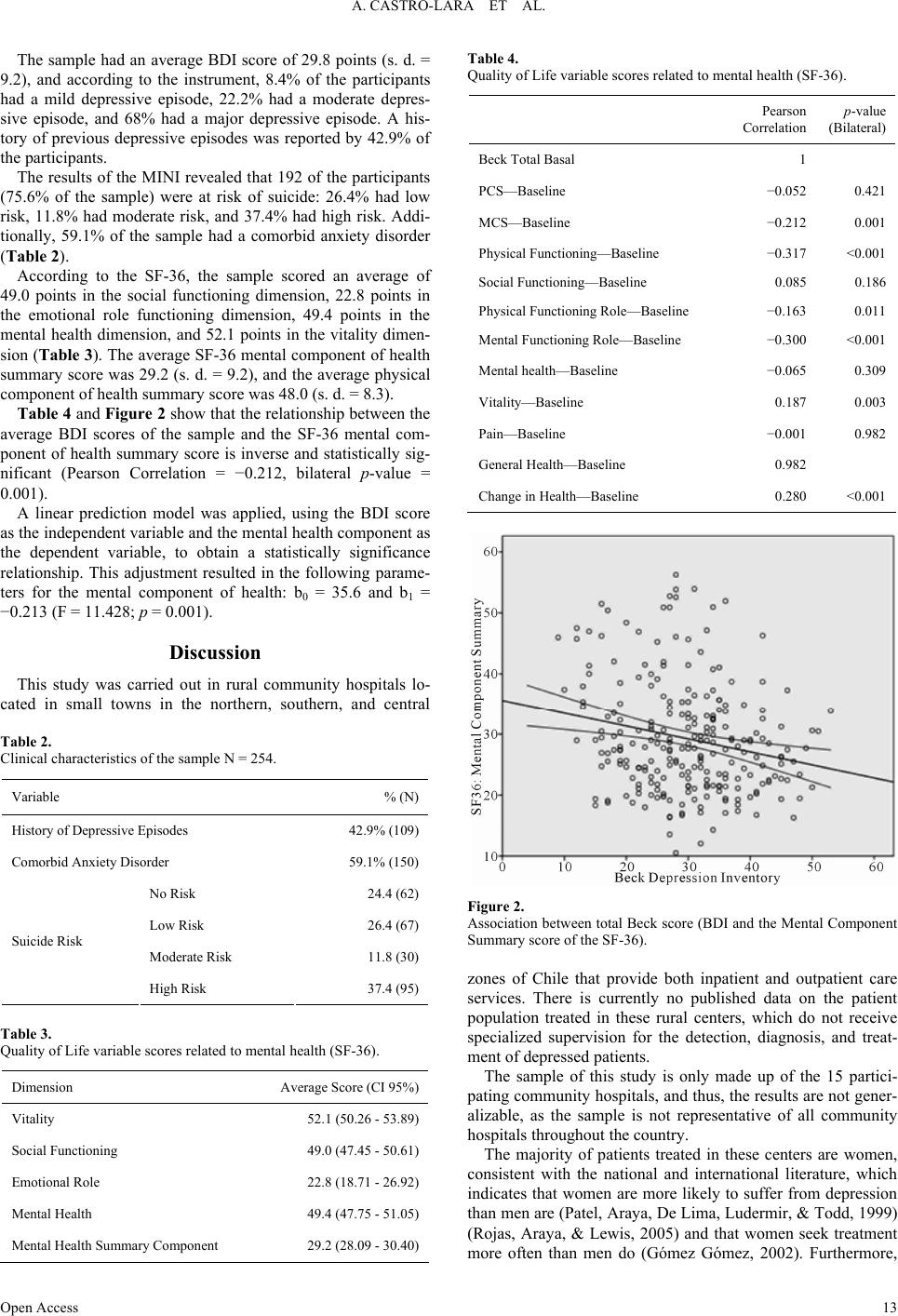
This study found a correlation between the intensity of de-
pressive symptoms, according to the BDI, and the SF-36 qual-
ity of life components. The sample’s SF-36 scores revealed
significant degrees of disability, and as the participants’ sever-
ity of symptoms increased, they had worse quality of life. It is
noteworthy that the majority of previous studies that have
shown this correlation between depressive symptomatology and
the SF-36 were carried out in urban populations (Friedman,
Conwell, & Delavan, 2007).
These results indicate that primary care teams in these rural
health centers, with little mental health skills training, are treat-
ing clinically complex patients, necessitating collaboration and
networking with specialized professionals. There has yet to be
sufficient research into what treatment alternative is most effec-
tive and what barriers exist to achieve collaboration with spe-
cialized secondary care teams and to ensure successful referral
of complex cases. Collaborative initiatives between primary
care and mental health professionals have shown positive re-
sults in terms of reduced referral time, treatment duration,
number of visits, and costs associated with treatment (Gilbody,
Bower, Fletcher, Richards, & Sutton, 2006; Van Orden, Hoff-
man, Haffmans, Spinhoven, & Hoencamp, 2009). Similar ini-
tiatives, which have also incorporated telemedicine, have pro-
duced good results in terms of improved mental health status,
quality of life, and user satisfaction (Fortney et al., 2007).
REFERENCES
Alvarado, R., & Rojas, G. (2011). The national programme for the
diagnosis and treatment of depression in primary care: An evaluation
necessary. Revista Médica de Chile, 139, 592-599.
http://dx.doi.org/10.4067/S0034-98872011000500005
Alvarado, R., Vega, J., Sanhueza, G., & Muñoz, M. G. (2005). Program
Evaluation for the detection, diagnosis and comprehensive treatment
of depression in primary care in Chile. Revista Panamericana de
Salud Pública, 18, 278-286.
Beck, A. T., Steer, R. A., & Carbin, M. G. (1998). Psychometric prop-
erties of the Beck Depression Inventory: Twenty-five years of eva-
luation. Clinical Ps y c hology Review, 8, 77-100.
http://dx.doi.org/10.1016/0272-7358(88)90050-5
Escobar, C., & Rojas, G. (2010). Suicidal behavior observed in hospi-
talizations Frutillar. Hospital’s revision 2008-2009. Revista de Psi-
quiatría Clínica, 48, 7-14.
Florenzano, R., Acuña, J., Fullerton, C., & Castro, C. (1998). Compara-
tive study of the frequency and features of emotional disturbances in
patients in primary care clinics. Revista Médica de Chile, 126, 397-
405.
Fortney, J., Pyne, J., Edlund, M., Williams, D., Robinson, D., Mittal, D.,
& Henderson, K. (2007). A randomized trial of telemedicine-based
collaborative care for depression. Journal of General Internal Medi-
cine, 22, 1086-1093. http://dx.doi.org/10.1007/s11606-007-0201-9
Friedman, B., Conwell, Y., & Delavan, R. L. (2007). Correlates of
late-life major depression: A comparison of urban and rural primary
care patients. The American Journal of Geriatric Psychiatry, 15, 28-
41. http://dx.doi.org/10.1097/01.JGP.0000224732.74767.ad
Gilbody, S., Bower, P., Fletcher, J., Richards, D., & Sutton, A. J.
(2006). Collaborative care for depression: A cumulative meta-analy-
sis and review of longer-term outcomes. Archives of Internal Medi-
cine, 166, 2314-2321. http://dx.doi.org/10.1001/archinte.166.21.2314
Gómez Gómez, E. (2002). Gender, equity and access to health services:
An empirical approach. Revista Panamericana de Salud Pública, 11,
327-334.
Inostroza, M. (2006). Health status survey 2004-2005 Isapres’s pop-
ulation. www. superintendenciadesalud
Kohn, R., Levav, I., de Almeida, J. M., Vicente, B., Andrade, L.,
Caraveo-Anduaga, J. J., Saraceno, B., et al. (2005). Mental disorders
in Latin America and the Caribbean: A public health priority. Revista
Panamericana de Salud Pública, 18, 229-240.
http://dx.doi.org/10.1590/S1020-49892005000900002
Luo, W., & Wang, F. (2003). Measures of spatial accessibility to health
care in a GIS environment: Synthesis and a case study in the Chicago
region. Environment and Pl anni ng B, 30, 865-884.
http://dx.doi.org/10.1068/b29120
Mendonza-Sassi, R., & Béria, J. U. (2001). Use of health services: A
systematic review of factors related. Cuadernos Médico Sociales, 81,
43-60.
Ministry of Health (2009). Clinic guide treatment of people with de-
pression. Santiago: Ministry of Health.
Ministry of Health (2012). Department of health statistics and informa-
tion. http://www.deis.cl/
Moyano Díaz, E., & Barría, R. (2006). Suicide and Gross Domestic
Product (GDP) in Chile: Towards a model predictive quality of life.
Revista Latinoamericana de Psicología, 38, 343-359.
Murray, C. J. L., & Lopez, A. D. (1997). Alternative projections of
mortality and disability by cause 1900-2020: Global burden of dis-
ease study. The Lancet, 349, 1498-1504.
http://dx.doi.org/10.1016/S0140-6736(96)07492-2
Murray, C. J. L., & Lopez, A. D. (1996). The global burden of disease.
Cambridge, MA: Harvard School of Public Health on behalf of the
World Bank.
Patel, V., Araya, R., De Lima, M., Ludermir, A., & Todd, C. (1999).
Women, poverty and common mental disorders in four restructuring
societies. Social Science & Medicine, 49, 1461-1471.
http://dx.doi.org/10.1016/S0277-9536(99)00208-7
Rojas, G., Araya, R., & Fritsch, R. (2000). Mental health, psychosocial
and primary health care. Acta Psiquiátrica y Psicológica de América
Latina, 46, 119-126.
Open Access
14