B. AJILCHI ET AL.
Open Access 849
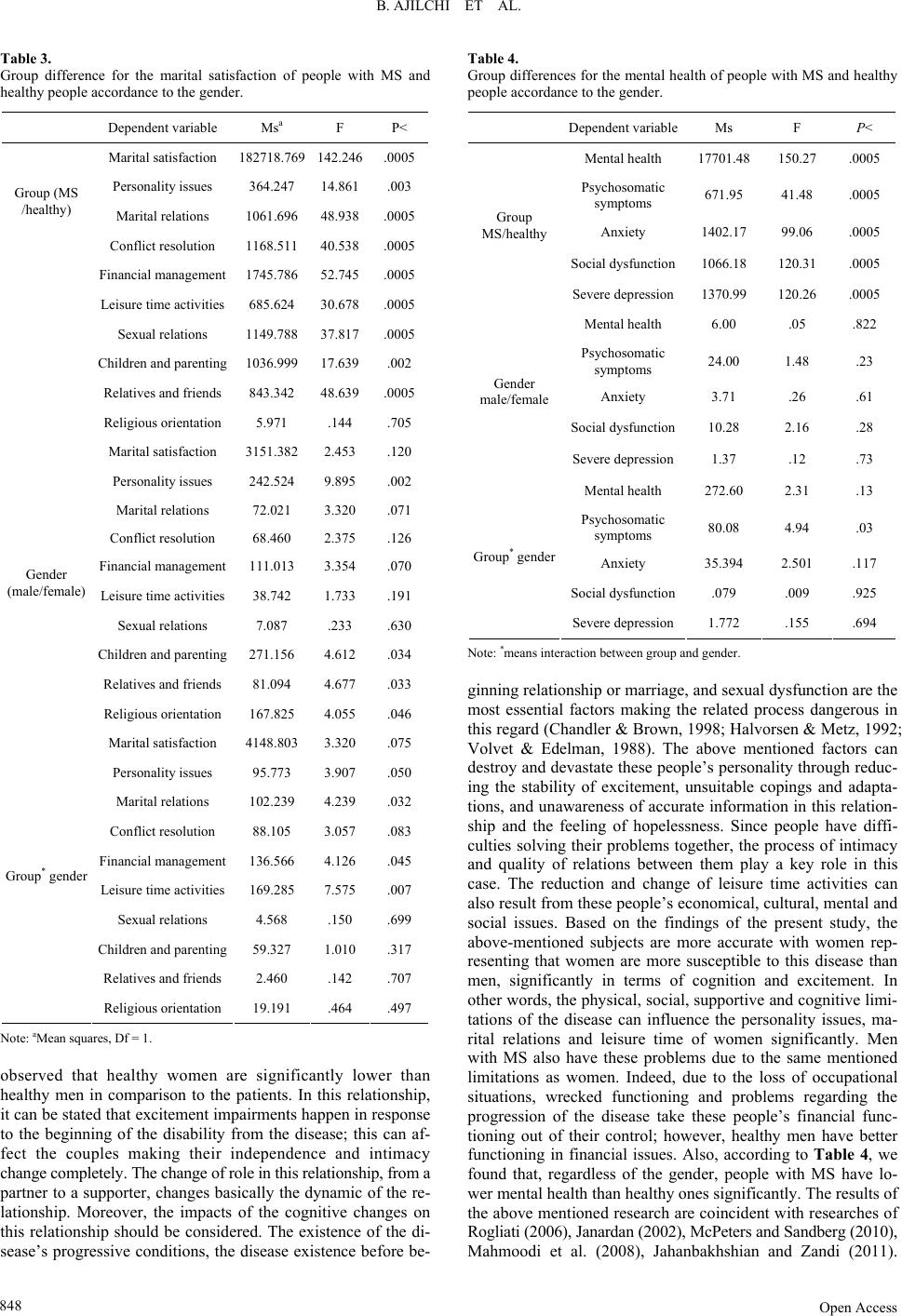
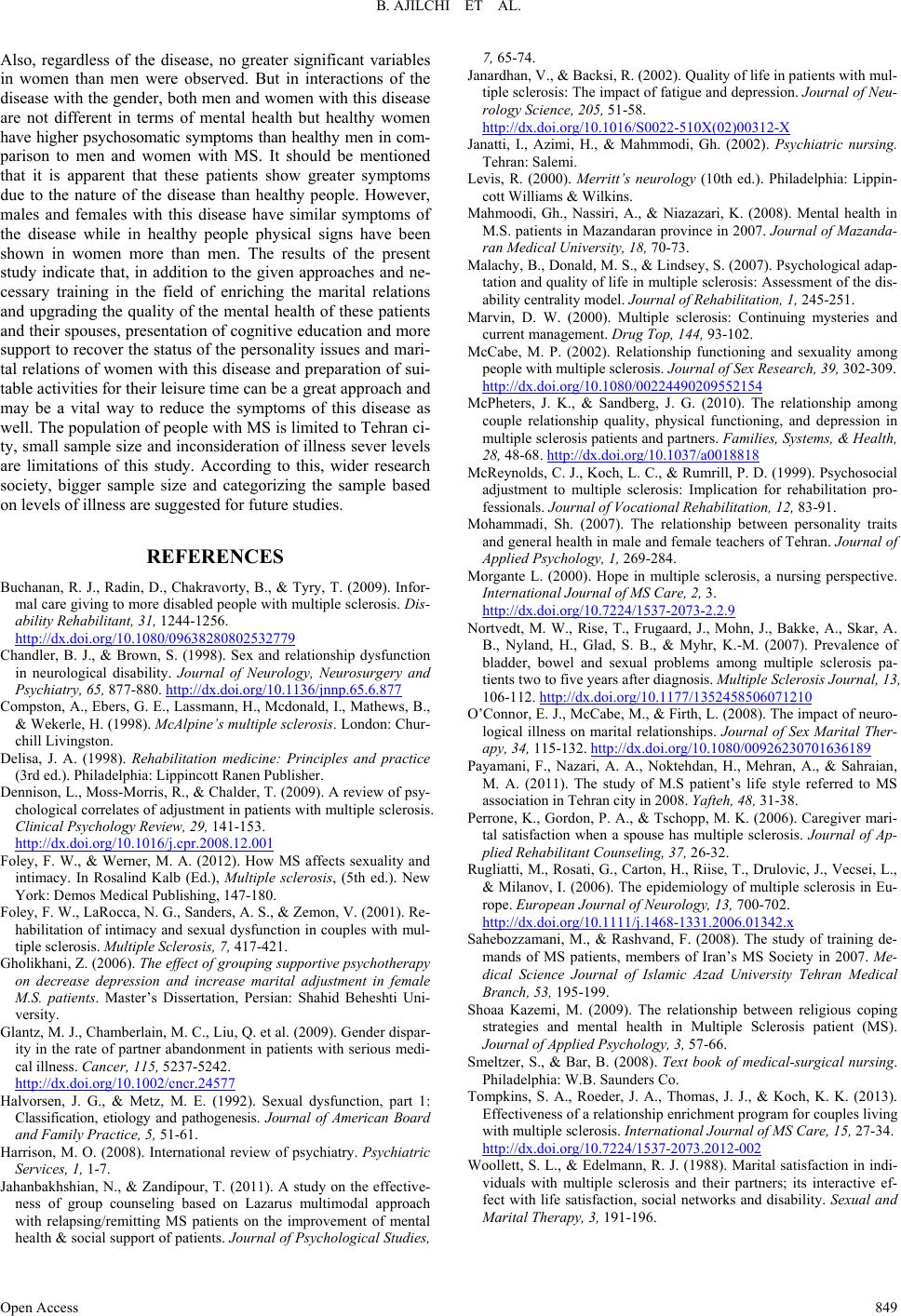
Also, regardless of the disease, no greater significant variables
in women than men were observed. But in interactions of the
disease with the gender, both men and women with this disease
are not different in terms of mental health but healthy women
have higher psychosomatic symptoms than healthy men in com-
parison to men and women with MS. It should be mentioned
that it is apparent that these patients show greater symptoms
due to the nature of the disease than healthy people. However,
males and females with this disease have similar symptoms of
the disease while in healthy people physical signs have been
shown in women more than men. The results of the present
study indicate that, in addition to the given approaches and ne-
cessary training in the field of enriching the marital relations
and upgrading the quality of the mental health of these patients
and their spouses, presentation of cognitive education and more
support to recover the status of the personality issues and mari-
tal relations of women with this disease and preparation of sui-
table activities for their leisure time can be a great approach and
may be a vital way to reduce the symptoms of this disease as
well. The population of people with MS is limited to Tehran ci-
ty, small sample size and inconsideration of illness sever levels
are limitations of this study. According to this, wider research
society, bigger sample size and categorizing the sample based
on levels of illness are suggested for future studies.
REFERENCES
Buchanan, R. J., Radin, D., Chakravorty, B., & Tyry, T. (2009). Infor-
mal care giving to more disabled people with multiple sclerosis. Dis-
ability Rehabilitan t, 31, 1244-1256.
http://dx.doi.org/10.1080/09638280802532779
Chandler, B. J., & Brown, S. (1998). Sex and relationship dysfunction
in neurological disability. Journal of Neurology, Neurosurgery and
Psychiatry, 65, 877- 880. http://dx.doi.org/10.1136/jnnp.65.6.877
Compston, A., Ebers, G. E., Lassmann, H., Mcdonald, I., Mathews, B.,
& Wekerle, H. (1998). McAlpine’s multiple sclerosis. London: Chur-
chill Livingston.
Delisa, J. A. (1998). Rehabilitation medicine: Principles and practice
(3rd ed.). Philadelphia: L ippincott Ranen Publisher.
Dennison, L., Moss-Morris, R., & Chalder, T. (2009). A review of psy-
chological correlates of adjustment in patients with multiple sclerosis.
Clinical Psychology Re vi e w , 29, 141-153.
http://dx.doi.org/10.1016/j.cpr.2008.12.001
Foley, F. W., & Werner, M. A. (2012). How MS affects sexuality and
intimacy. In Rosalind Kalb (Ed.), Multiple sclerosis, (5th ed.). New
York: Demos Medical Publishing, 147-180.
Foley, F. W., LaRocca, N. G., Sanders, A. S., & Zemon, V. (2001). Re-
habilitation of intimacy and sexual dysfunction in couples with mul-
tiple sclerosis. Multiple Sclerosis, 7, 417-421.
Gholikhani, Z. (2006). The effect of grouping supportive psychotherapy
on decrease depression and increase marital adjustment in female
M.S. patients. Master’s Dissertation, Persian: Shahid Beheshti Uni-
versity.
Glantz, M. J., Chamberlain, M. C., Liu, Q. et al. (2009). Gender dispar-
ity in the rate of partner abandonment in patients with serious medi-
cal illness. Cancer, 115, 5237-5242.
http://dx.doi.org/10.1002/cncr.24577
Halvorsen, J. G., & Metz, M. E. (1992). Sexual dysfunction, part 1:
Classification, etiology and pathogenesis. Journal of American Board
and Family Practice, 5, 51-61.
Harrison, M. O. (2008). International review of psychiatry. Psychiatric
Services, 1, 1-7.
Jahanbakhshian, N., & Zandipour, T. (2011). A study on the effective-
ness of group counseling based on Lazarus multimodal approach
with relapsing/remitting MS patients on the improvement of mental
health & social support of patients. Journal of Psychological Studies,
7, 65-74.
Janardhan, V., & Backsi, R. (2002). Quality of life in patients with mul-
tiple sclerosis: The impact of fatigue and depression. Journal of Neu-
rology Science, 205, 51-58.
http://dx.doi.org/10.1016/S0022-510X(02)00312-X
Janatti, I., Azimi, H., & Mahmmodi, Gh. (2002). Psychiatric nursing.
Tehran: Salemi.
Levis, R. (2000). Merritt’s neurology (10th ed.). Philadelphia: Lippin-
cott Williams & Wilkins.
Mahmoodi, Gh., Nassiri, A., & Niazazari, K. (2008). Mental health in
M.S. patients in Mazandaran province in 2007. Journal of Mazanda-
ran Medical University, 18, 70-73.
Malachy, B., Donald, M. S., & Lindsey, S. (2007). Psychological adap-
tation and quality of life in multiple sclerosis: Assessment of the dis-
ability centrality model. Journal of Rehabilitation, 1, 245-251.
Marvin, D. W. (2000). Multiple sclerosis: Continuing mysteries and
current management. Drug Top, 144, 93-102.
McCabe, M. P. (2002). Relationship functioning and sexuality among
people with multiple sclerosis. Journal of Sex Research, 39, 302-309.
http://dx.doi.org/10.1080/00224490209552154
McPheters, J. K., & Sandberg, J. G. (2010). The relationship among
couple relationship quality, physical functioning, and depression in
multiple sclerosis patients and partners. Families, Systems, & Health,
28, 48-68. http://dx.doi.org/10.1037/a0018818
McReynolds, C. J., Koch, L. C., & Rumrill, P. D. (1999). Psychosocial
adjustment to multiple sclerosis: Implication for rehabilitation pro-
fessionals. Journal of Voca tional Rehabilitation, 12, 83-91.
Mohammadi, Sh. (2007). The relationship between personality traits
and general health in male and female teachers of Tehran. Journal of
Applied Psychology, 1, 269-284.
Morgante L. (2000). Hope in multiple sclerosis, a nursing perspective.
International Journal of MS Car e, 2, 3.
http://dx.doi.org/10.7224/1537-2073-2.2.9
Nortvedt, M. W., Rise, T., Frugaard, J., Mohn, J., Bakke, A., Skar, A.
B., Nyland, H., Glad, S. B., & Myhr, K.-M. (2007). Prevalence of
bladder, bowel and sexual problems among multiple sclerosis pa-
tients two to five years after diagnosis. Multiple Sclerosis Journal, 13,
106-112. http://dx.doi.org/10.1177/1352458506071210
O’Connor, E. J., McCabe, M., & Firth, L. (2008). The impact of neuro-
logical illness on marital relationships. Journal of Sex Marital Ther-
apy, 34, 115-132. http://dx.doi.org/10.1080/00926230701636189
Payamani, F., Nazari, A. A., Noktehdan, H., Mehran, A., & Sahraian,
M. A. (2011). The study of M.S patient’s life style referred to MS
association in Tehran city in 2008. Yafteh, 48, 31-38.
Perrone, K., Gordon, P. A., & Tschopp, M. K. (2006). Caregiver mari-
tal satisfaction when a spouse has multiple sclerosis. Journal of Ap-
plied Rehabilitant Counsel ing, 37, 26-32.
Rugliatti, M., Rosati, G., Carton, H., Riise, T., Drulovic, J., Vecsei, L.,
& Milanov, I. (2006). The epidemiology of multiple sclerosis in Eu-
rope. European Journal of Neurology, 13, 700-702.
http://dx.doi.org/10.1111/j.1468-1331.2006.01342.x
Sahebozzamani, M., & Rashvand, F. (2008). The study of training de-
mands of MS patients, members of Iran’s MS Society in 2007. Me-
dical Science Journal of Islamic Azad University Tehran Medical
Branch, 53, 195-199.
Shoaa Kazemi, M. (2009). The relationship between religious coping
strategies and mental health in Multiple Sclerosis patient (MS).
Journal of Applied Psychology, 3, 57-66.
Smeltzer, S., & Bar, B. (2008). Text book of medical-surgical nursing.
Philadelphia: W.B. Saund e rs Co.
Tompkins, S. A., Roeder, J. A., Thomas, J. J., & Koch, K. K. (2013).
Effectiveness of a relationship enrichment program for couples living
with multiple sclerosis. Interna tional Journal of MS Care, 15, 27-34.
http://dx.doi.org/10.7224/1537-2073.2012-002
Woollett, S. L., & Edelmann, R. J. (1988). Marital satisfaction in indi-
viduals with multiple sclerosis and their partners; its interactive ef-
fect with life satisfaction, social networks and disability. Sexual and
Marital Therapy, 3, 191-196.