Health
Vol.5 No.9(2013), Article ID:36318,5 pages DOI:10.4236/health.2013.59186
Assessment of the knowledge, attitude and practice of rural women of northeast Nigeria on risk factors associated with cancer of the Cervix
![]()
Department of Community Medicine, College of Medical Sciences, University of Maiduguri, Maiduguri, Nigeria; *Corresponding Author: atunjeba@yahoo.com
Copyright © 2013 Babatunji A. Omotara et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 23 May 2013; revised 24 June 2013; accepted 25 July 2013
Keywords: Risk factors; cervical cancer; rural women; north-eastern Nigeria
ABSTRACT
Cervical cancer is the leading cancer-related cause of death among women in Nigeria. An estimated 70,700 new cases occur each year, representing one quarter of all female cancers in sub Saharan Africa. The magnitude of the problem has been under recognised and under prioritised compared with the competing health priorities of infectious diseases such as HIV/ AIDS, tuberculosis and malaria. Studies in the United States and Nigeria have indicated that the disease has the highest incidence among the lowest socio-economic groups especially residing in rural areas. The peak age for the disease has been shown to be within 35 - 45 years age group. Knowledge of the risk factors of the disease is deemed important in its early detection and prevention. The objective of this study was to assess the knowledge, attitude and practice of rural women with cancer of the cervix. A cross sectional descriptive study was conducted among 1600 rural women aged 15 - 55 years (randomly selected from 28 villages) who were interviewed using a structured questionnaire between April and June, 2010. The majority (82.2%) were married before the age of 20 years and 19.3% before 15 years, 40% in polygamous union, 22.6% have had 2 or more sexual partners, 71.3% were primi and grand multiparous, 7.5% have had previous treatment for STIs and 10.1% were on various types of contraceptive. 454 (28.4%) have heard of Ca cervix, 358 (22.4%) knew the location of the cervix. 2.3% had Pap smear test of which 72.6% were within 2 years. The majority (89.9%) will avail themselves for screening.
1. INTRODUCTION
Cervical cancer is the most common cancer and the leading cancer-related cause of death among women in sub Saharan Africa. An estimated 70,700 new cases occur each year, representing one quarter of all female cancers in sub Saharan Africa. The magnitude of the problem has been under recognized and under prioritized compared with the competing health priorities of infectious diseases such as HIV/AIDS, tuberculosis and malaria. Studies in the United States and Nigeria have indicated that the disease has the highest incidence among the lowest socio-economic groups [1].
Munoz and Bosch [2] reported that cervical cancer accounts for 15 percent of all cancers in women worldwide; about 2.5 million women suffer from cervical cancer, over 80 percent of all cases occur in developing countries where cancer of the cervix is the most common cancer among women. Annual deaths from cervical cancer worldwide are approximately 270,000 with nearly 85% of those deaths from resource poor nations [3].
High mortality of the disease recorded in most developing countries has been attributed mostly to late presentation consequent to poor level of awareness.
Cervical cancer incidence is low in young women but increases with age. The peak age of the incidence in some countries has been shown to be in the 50 - 59 year age group. However, Babatunde [4] reported that in Nigeria, the peak incidence has been found to be fifteen years earlier, that is, in the 35 - 45 year age group.
Cancer of the cervix aetiology is not well known. However, early sexual exposure, multiple sexual partners, multiparity, sexually transmitted diseases, cigarette smoking and use of combined oral contraceptives (barrier contraceptive is protective) play important roles in the development of cervical cancer.
Studies have identified the total number of sexual partners and age at first sexual intercourse as the two main risk factors irrespective of marital status. This is probably because of the high chances of infection with human Papilloma virus (HPV), most especially the high risk subtypes 16 and 18 [5]. Significant epidemiological observations related to cancer of the cervix have shown that it is rare in virgins and Nuns compared to married women and women who are sexually active [6].
In northern Nigeria, it is the commonest cancer while in southern Nigeria it is second to breast cancer.
The good news is that cervical cancer is largely, a potentially preventable disease if detected early. In the developed world, the incidence of the disease has decreased over the years due to the availability of well-organized cervical cancer screening programmes. Screening allows for the detection of the curable premalignant lesions. Therefore, creating and increasing awareness about the disease among women at risk will lead to desired increase in the response to screening with consequent early detection of the disease.
The objective of this study was to assess the knowledge, attitude and practice of rural women with cancer of the cervix.
2. METHODOLOGY
The study was carried out in 4 local government areas (LGAs) of north-eastern area of Nigeria; Konduga, Bama, Gwoza and Madagali over a period of eight weeks (April to June, 2010) to assess the knowledge, attitude and practice of rural women aged 15 - 55 years regarding risk factors of cancer of the cervix. A cross sectional descriptive study involving 1600 rural women aged 15 - 55 years randomly selected from 28 village units was carried out using a structured validated questionnaire by four groups of final year medical students during their eight week community based medical posting [7]. In each LGA a total of 400 questionnaires were administered to eligible from an average of seven village units from each.
A multi-stage sampling method was used to select respondents from each LGA, each having an average of four districts. In the first stage, one district was chosen randomly for the study. In the second stage, two village units were chosen from each district. And in the third stage, of the village units selected, two wards were selected from which households were selected using systematic sampling. In each household an eligible female was interviewed. However, in households where there were more than one eligible female, balloting was used to select the respondent. A total of 56 wards were selected from which the 1600 respondents were obtained.
The questionnaire comprised of four sections which sought information on the demographic background of the respondent, knowledge on ca cervix and position of the cervix in the body, attitude towards risk factors associated with ca cervix; and knowledge and practice of Pap smear test. The data was analyzed statistically using Epi Info software version 3.4.1.
3. RESULTS
Table 1 shows that the majority of the respondents are in the age group 15 to 34 (79.8%) while 85% are married. The majority (44%) are housewives while the rest are farmers, students, traders or work for the government (civil servants). Slightly over one quarter have no education, about 20% have Quranic education and the rest (56.5%) have some level of western education.
Table 2 shows that only 22.4% are aware of the location of the cervix on their body, while 28.4% have heard of Ca cervix of which 43.6% know that it is preventable and only 38.8% know of the screening for the disease.
Table 3 shows that majority of the respondents were married between the ages of 10 and 19 years (82.2%) majority of which was monogamy (51.5%) only 39.7% were in polygamous marriage. The majority (93.6%) had sexual relationship with more than one male after the first sexual exposure. The majority 82.3% were in their first marriage. The majority 39.2% were grand multiparous. Only 7.5% have had previous treatment for STIs while 89.9% do not use any form of contraceptives.
Table 4 shows that only 36 or 2.3% have heard of Pap smear all of whom had had it over a range of time between 1 month and 5 years. However, the majority 1439 (89.9%) will avail themselves the opportunity of screening if available.
4. DISCUSSION
Only 28.4% of our respondents have heard of cancer of the cervix which is in consonance with results of other studies from most sub-Saharan nations [8-10]. However, Asuzu et al. [11] reported a much higher level of awareness 79.1% among female staff of a tertiary institution in southwest Nigeria, while Al-Meer et al. [12] reported an awareness rate of 85.2% among women attending primary health care in Qatar.
Certain risk factors such as early onset of sexual intercourse, multiple sexual partners and frequent STIs are known to be highly associated with the disease. The result of this study shows that majority (82.2%) of the respondents got married before the age of 20 years of which 19.3% were below 15 years. This is due largely to the traditional/religious practices in the community of study. It is believed that a young girl should be married off at the commencement of puberty. Even though the study communities are largely Muslim, monogyny was mostly reported in the study and majority of the respon-
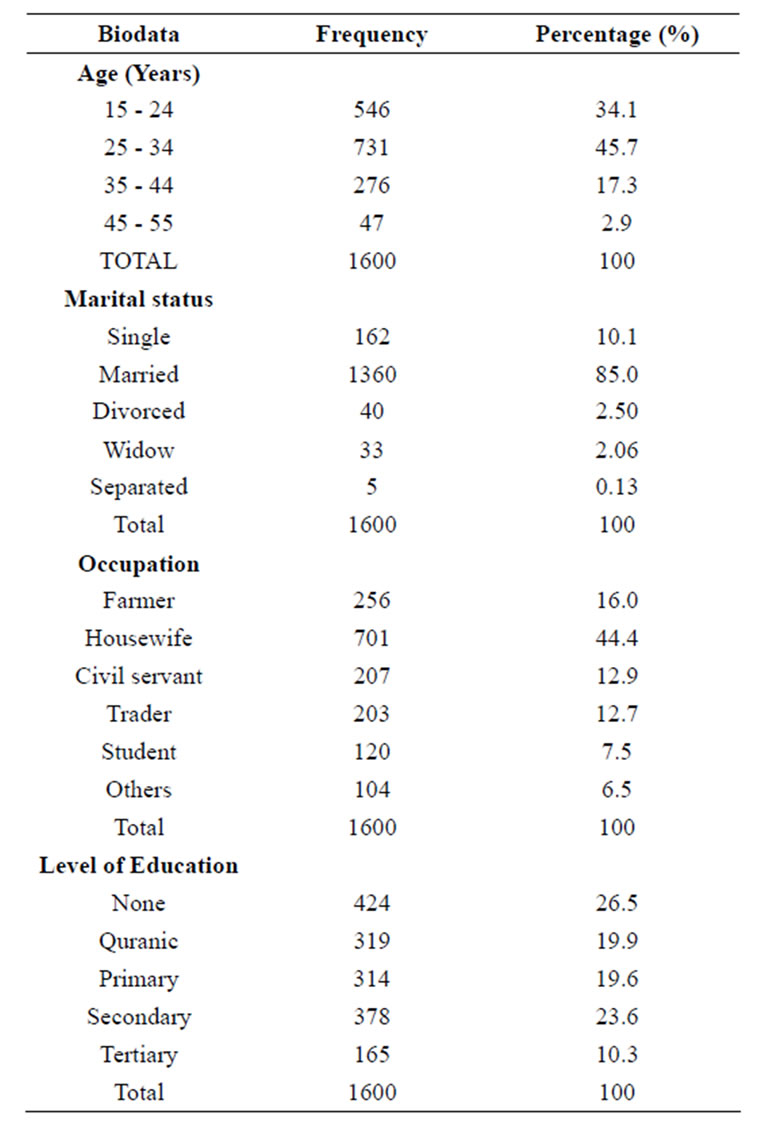
Table 1. Demographic characteristics of respondents.
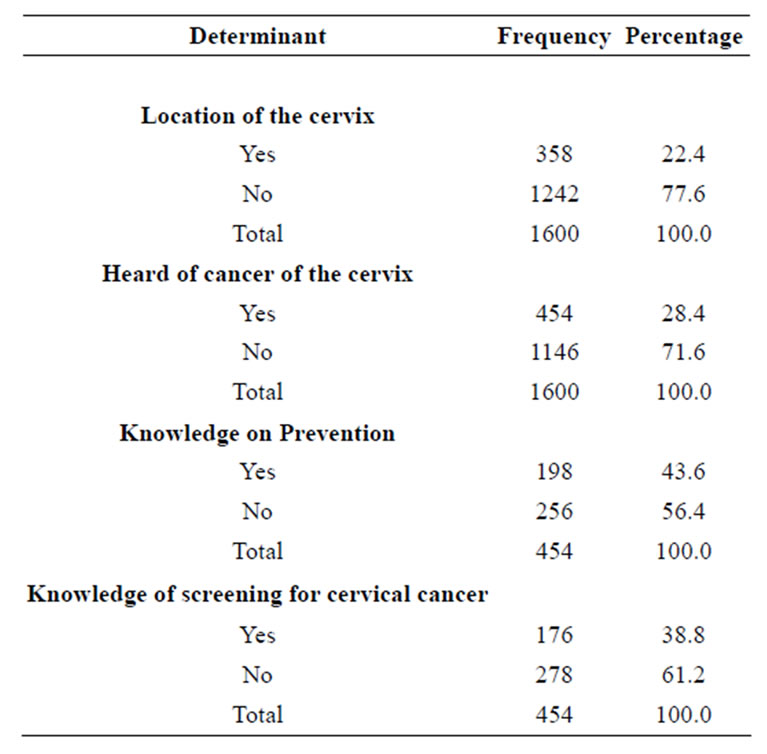
Table 2. Level of awareness of cervical cancer and screening among women of reproductive age group in north-eastern Nigeria.
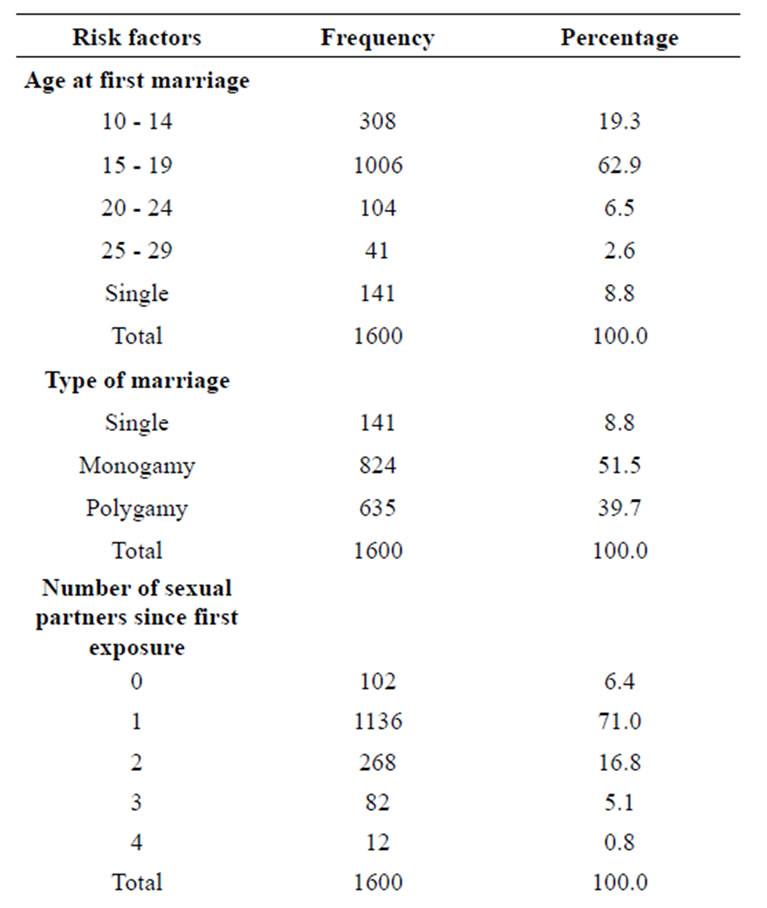

Table 3. Distribution of risk factors for cervical cancer amongst respondents in north-eastern Nigeria.
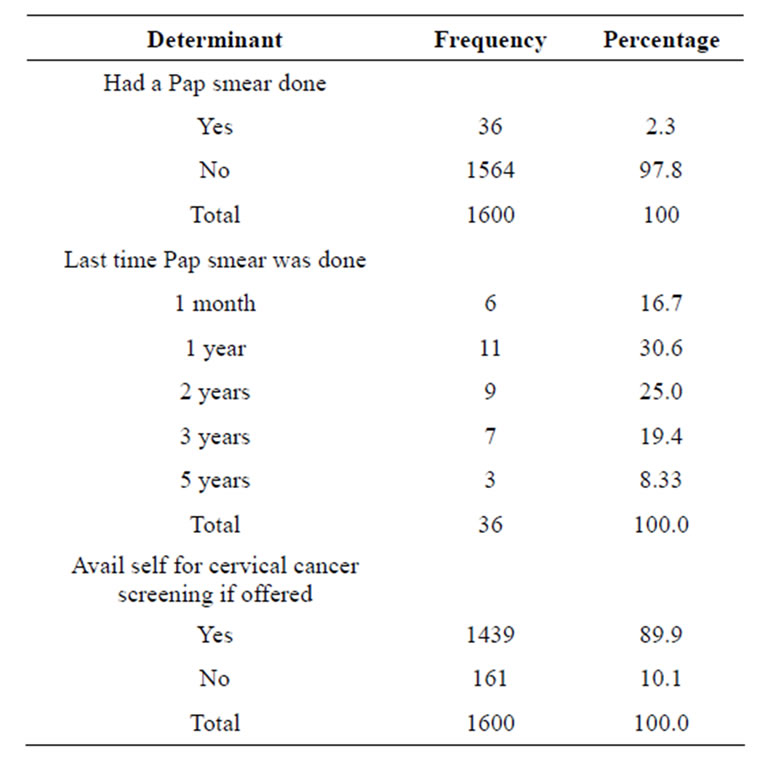
Table 4. Practice of respondents to cervical cancer screening in north-eastern Nigeria.
dents were in their first marriage. Because of early marriage most respondents are grand multiparous. The majority of the respondents (89.9%) are not on any form of contraceptive. This was largely due to religious and cultural beliefs which forbid the use of any form of contraception. Contraceptive use has been identified as one of the risk factors for cancer of the cervix therefore, this is one instance where cultural/religious practice is deemed to be advantageous. Prevalence of STIs reported in this study is low (7.5%) which may be as a result of the strong religious and cultural beliefs. Only 6.4% have had no other sexual partners while the majority have had at least one or more of which 71% have had only one additional sexual partner. This is significantly higher than what was reported among female secondary school teachers in southwest Nigeria (21.4%) and among women visiting primary care in Qatar (6.8%) [12,13]. Knowledge of risk factors is important to women at risk to enable them seek help early. Hoque et al. [14] reported that only 6% knew all and 65% knew any one of the risk factors of cervical cancer among women in a rural community in South Africa.
In our study only 22.4% knew where the cervix is located on their body. Also knowledge of the screening for the disease was correspondingly low as well as their knowledge on whether it can be prevented 43.6% and 38.8%, respectively. Only 2.3% have heard of Pap smear test and had one done on them. In rural South Africa 18% of women were reported to have ever had Pap smear test done [14]. In Qatar less than half (44%) believed that the disease can be detected with the Pap smear before symptoms appear [12].
Perhaps the most encouraging of the result of our study is that majority (89.9%) are willing to avail themselves with the opportunity to be screened.
Evidence suggests that HPV vaccines prevent HPV infection. Gadasil is a quadrivalent vaccine which is approved for girls and women of age 9 - 26 years for the prevention of cervical cancer (and also genital warts and anal cancer caused by HPV 6, 11, 16, and 18 in the United States. Unfortunately this vaccine is not yet available in Nigeria.
5. CONCLUSIONS
The awareness of cervical cancer and knowledge of its risk factors are very low among women of reproductive age group in northeast Nigeria with high prevalence of the risk factors. The practice towards prevention is also low due to the poor knowledge/ awareness of the disease, however, the majority of the respondents are willing to undergo the screening test if available. Successful implementation of screening and primary care depend on awareness and willingness on the part of women at risk. The fact that most of the women in our study are willing to undergo screening is considered important as other studies in other part of Nigeria, South Africa and Zambia reported that most women were not aware of HPV and did not believe that it could be prevented [8-10].
It is recommended that community based education which is religious and culture specific should be instituted as suggested by Olusola et al. [15]. In addition facilities for screening should be made available at the primary health care centres with trained health personnel.
6. ACKNOWLEDGEMENTS
The authors acknowledge the contributions of the four groups of medical students for the collection of data, the local government authorities, traditional heads and all the elderly persons who participated in the study.
REFERENCES
- Bukar, M., Mayun, A.A., Audu, B.M., Musa, A.B. and Inuwa, U. (2009) Prevalence of pre-invasive lesions of the cervix in Maiduguri, north-eastern Nigeria. Nigerian Medical Practitioner, 55, 52-55. doi:10.4314/nmp.v55i4.45431
- Munoz, N. and Bosch, F.X. (1999) Epidemiology of cervical cancer. In: Munoz, N., Bosch, F.X. and Johnson, O.M., Eds., Human Papilloma and Cervical Cancer in International Journal of Gynaecology and Obstetrics, 67, 87-94.
- Alliance for Cervical Cancer Prevention (2009) New evidence on the impact of cervical cancer screening and treatment using HPV DNA tests, visual inspection or cytology. http://.alliance-cxca.org/
- Babatunde, A. (1978) Carcinoma of the cervix in Nigeria (Ibadan experience). Nigerian Medical Practitioner, 8, 12-15.
- Nahmias, A.J., Joxy, W.E. and Oleske J.M. (1980) Epidemiology of cervical cancer in viral Infection in Humans. Planum Publishing Co., New York.
- Jacob, B., Michal, A.R. and Hahn, A. (1995) Aetiology of cervical cancer: Current concept CME review article. Obstetrics and Gynaecology Survey, 50, 146-153. doi:10.1097/00006254-199502000-00027
- Omotara, B.A., Padonu, M.K.O., Bassi, A.P. and Amodu, M.O. (1992) Community-Based Medical Education (CBME): University of Maiduguri Experience. Annals of Community-Oriented Education, 5, 41-46.
- Nnondu, O., Erinosho, L., Jamda, M. and Olaniyi, O. (2010) Knowledge and attitudes towards cervical cancer and human Papilomavirus: A Nigerian pilot study. African Journal of Reproductive Health, 14, 95-108.
- Francis, S.A., Nelson, J., Liverpool, J., Soogun, S., Mofammere, N. and Thorpe Jr., R.J. (2010) Examining attitudes and knowledge about HPV and cervical cancer risk among female clinic attendees in Johannesburg. Fourth African Vaccine, 28, 8026-8032.
- Chirwa, S., Nwanahamuntu, M., Kapambwe, S., Mkumba G., Stringer, J., Sahasrabuddher, V., Pfaendler, K. and Parham, G. (2010) Myths and misconceptions about cervical cancer among Zimbabwe women: Rapid assessment by peer educators. Global Health Promotion, 17, 47-50. doi:10.1177/1757975910363938
- Asuzu, C.C., Unegbu, J. and Akin-Odanye, E. (2011) Knowledge, attitude and behaviour of the University of Ibadan women towards cancer of the cervix and its prevention. Psychooncology. doi:10.1002/pon.2007
- Al-Meer, F.M., Aseel, M.T., Al khalaf, J., Al-Kuwari, M.G. and Imail, M.F.S., (2011) Knowledge, attitude and practices regarding cervical cancer and screening among women visiting primary health care in Qatar. Eastern Mediterranean Health Journal, 17, 855-861.
- Adekanle, D.A., Adeyemi, A.S. and Afolabi, A.F. (2011) Knowledge, attitude and cervical cancer screening among secondary school teachers in Osogbo, Southwest Nigeria. Academic Journal of Cancer Research, 4, 24-28.
- Hoque, M., Hoque, E. and Kader, S.B. (2008) Evaluation of cervical cancer screening program at a rural community of South Africa. East African Journal of Public Health, 5, 111-116.
- Olusola, A.A., Olayinka, O.O. and Olatunde, J.A. (2005) Determinants of cervical cancer knowledge and utilization of screening among Nigerian female population, Ibadan, Nigeria. Tropical Journal of Obstetrics and Gynaecology, 22, 1.