International Journal of Clinical Medicine
Vol.3 No.3(2012), Article ID:19384,6 pages DOI:10.4236/ijcm.2012.33036
Study of Cardiac Manifestations in Patients with HIV Infection and Their Correlation with CD4 Count in Indian Population
![]()
1Postgraduate Department of Medicine, SCB Medical College and Hospital, Cuttack, India; 2Postgraduate Department of Medicine and Nodal Officer, Anti Retroviral Therapy (ART) Centre, SCB Medical College and Hospital, Cuttack, India.
Email: *drsidhartha.cuttack@gmail.com
Received January 10th, 2012; revised February 20th, 2012; accepted March 11th, 2012
Keywords: HIV; AIDS; PLHA; CD4 count; echocardiographic findings
ABSTRACT
Introduction: With advances in the management of patients living with HIV and AIDS (PLHA), not only survival has increased but manifestations of late stage HIV infection are encountered more often including cardiovascular complications. Aims and Objectives: To determine the prevalence and characteristics of cardiac manifestations in patients with HIV infection and to evaluate their correlation with CD4 count. Materials and Method: 70 consecutive patients with HIV infection admitted to Post Graduate Department of Medicine from the period of July 2010 to August 2011 were studied. All cases of PLHA diagnosed after positive ELISA test for HIV infection were included, whereas those with congenital heart disease, rheumatic heart disease, hypertension, Ischemic heart disease were excluded from the study. CD4 count and 2D echocardiography along with routine investigations were done for all patients. Result: Male to female ratio was 2:1. Echocardiographic abnormalities were seen in 58% of patients. Reduced ejection fraction (below 50%) and fractional shortening below 30% were the most common cardiac abnormality (48.7%) followed by pericardial effusion (17.4%), pulmonary artery hypertension (11.4%), dilated cardiomyopathy (8.5%), diastolic dysfunction (8.5%) and regional wall motion abnormality (1.4%) respectively. Significant statistical positive correlation was observed between low CD4 count and echocardiographic abnormalities (p < 0.0001). Pericardial effusion was seen more in patients with CD4 count below 200 (p < 0.001). Maximum number of echocardiographic abnormalities was seen in WHO clinical stage IV. Conclusions: Cardiac manifestations are frequent PLHA in our population but do not have detectable clinical manifestation. Echocardiographic abnormalities have a strong correlation with low CD4 count and occur more in advanced stage of the disease.
1. Introduction
HIV infection has become a global pandemic with more than 33.3 million people infected throughout the world by the end of 2009 [1]. India is estimated to have 5.1 million infected individuals [2].
Acquired immunodeficiency syndrome (AIDS) is characterized by an acquired, profound, irreversible, immune suppression that predisposes the patient to multiple opportunistic infections, malignant neoplasms and a progressive dysfunction of multiple organ systems [3]. With the availability of a large armamentarium of anti-retroviral drugs and recent advances in the diagnosis, treatment and monitoring of persons living with HIV and AIDS (PLHA), there has been visible improved survival of such patients [4]. Due to the longer survival of PLHA, the manifestations of late stage HIV infection are now being met with more commonly than before, which includes HIV related cardiac diseases [4] .
Although not fully recognized in the early days of HIV epidemic, cardiac involvement has been reported with increasing frequency in recent years [5]. The prevalence of cardiac involvement in AIDS patients have been reported to range between 28% and 73% [5]. The cardiac diseases in HIV infections include pericardial effusion, left ventricular dysfunction myocarditis, dilated cardiomyopathy, endocarditis, pulmonary hypertension, malignant neoplasm, coronary artery disease and drug related cardiotoxicity [6].
Echocardiography is very helpful in detecting cardiac dysfunction at an early stage, much before overt clinical manifestations develop [7]. The most common sign of cardiac involvement is impairment of LV fractional shortening. This could be explained by reduction of cardiac contractility [6]. Early recognition and prompt treatment are important to prevent significant morbidity from cardiac involvement [8].
2. Materials and Methods
Seventy consecutive patients with HIV infection admitted to the Post Graduate Department of Medicine at S.C.B Medical College and Hospital were studied. All patients diagnosed to have HIV infection/AIDS after ELISA test being positive were included in the study. Patients suffering from 1) congenital heart disease; 2) rheumatic heart disease; 3) hypertension and 4) ischaemic heart disease were excluded from the study. As the subjects under study were patients hospitalized to this tertiary care centre, consent was taken at the point of hospitalistion for conducting the required investigations as detailed below.
All patients were assessed clinically by detailed history taking and general physical examination. Specific investigations were undertaken to establish diagnosis of HIV infection and screened for opportunistic infections. CD4 count was done for all patients using flowcytometry using a BD FACS Count system. The CD4 count was done using kits supplied by the National AIDS Control Organisation of India (NACO) to anti Retroviral Therapy (ART) Centre, Cuttack. Staging of the disease was done according to revised WHO clinical staging of the disease [9].
All patients were evaluated using M Mode and Two dimensional transthoracic echocardiography and colour flow doppler examination using Philips Sonos (MCMD02AA) in the Postgraduate Department of Cardiology of this institution. Each two dimensional study consist of parasternal long and short axis, and apical two and four chamber views. The conventions of American Society of Echocardiography were followed in obtaining left atrial dimensions, left ventricular end systolic and end diastolic dimensions, right ventricular end diastolic dimensions and left ventricular fractional shortening (FS) [7]. Left ventricular volumes were measured and ejection fraction (EF) was calculated. The presence of pericardial effusion, any valve regurgitation and any regional wall motion abnormalities was looked for.
Statistical analysis of data was done using SPSS 16 software.
3. Observations
Seventy consecutive patients with HIV infection who were hospitalized to inpatients of the department of Medicine were studied. There was a gender predominance with male is to female ratio being 2:1. The age of the patients studied ranged between 15 and 70 years, with a mean age of 38.87 (±8.71) years in males and 33.38 (±7.73) years in females respectively. Majority of the patients, 71% males and 67% females were young and were in the age group of 26 to 40 years. Sexual mode of transmission was the most common, out of which hetero-sexual accounted for 91.4% and homosexual 2.8% of cases. The other modes were blood transfusion (2.8%), IV drug abuse (1.4%) and vertical transmission (1.4%) respectively. The clinical features of the patients under study with relevance to cardiovascular system were fever (74.3%), cough (30%), breathlessness (28.6%), pedal edema (18.6%), chest pain (18.6%) and palpitation (10%). CD4 count was less than 50/micrL in 28.6%, 32.9% of cases had CD4 count between 50 to 200/microL while 25.7% had CD4 Count >350/micrL. The maximum number of patients studied were in clinical stage 4 (40%) followed by Clinical stage 3 (35.7%), Clinical stage 2 (14.3%) and only 10% of cases were in Stage 1respectively.
As shown in Table 1, echocardiographic abnormalities were seen in 55.7% of cases. Reduced EF (<50%) was seen in 22.8% and reduction in FS (<30%) in 48.6% of cases. Pericardial effusions was seen in 17.4% while pulmonary artery hypertension was noted in 11.4% of cases. Dilated cardiomyopathy and diastolic dysfunction was found in 8.5% of cases. One case had regional wall motion abnormality (RWMA) involving the anterior wall.
As presented in Table 2, maximum number of echocardiographic findings were seen in patients with CD4 count less than 200. Out of the total 16 patients with reduced EF, 9 patient had CD4 count less than 50. Similarly reduction in FS, 14 patients out of total 34 had CD4 count less than 50. 5 out 6 cases of dilated cardiomyopathy had CD4 count less than 50. Maximum number of cases with pericardial effusions, diastolic dysfunction and pulmonary artery hypertension had CD4 count less than 50. The lone case with RWMA also had CD4 count less than 50.

Table 1. 2D echocardiographic findings of the cases studied.
Table 3 shows association of 2D echocardiographic findings with revised WHO clinical staging. Maximum number of echocardiographic findings was seen in patients in clinical stage 4. Out of the total 16 patients with reduced EF, 11 patients were in stage 4, similarly in those with reduced FS, 22 out of total 34 were in stage 4. All the 6 cases of dilated cardiomyopathy were in stage 4. Maximum number of cases with pericardial effusions, diastolic dysfunction and pulmonary arterial hypertension were also in stage 4. The lone case of coronary artery disease was also in Stage 4.
Mean CD4 counts was found to be 100 ± 110 in patients with echocardiographic abnormalities, whereas it was 337.6 ± 207.4 in patients without echocardiographic abnormalities (p < 0.0001). There was no statistically significant correlation of cardiac manifestations with hemoglobulin values or total leukocyte count.
Pericardial effusions was seen in 12 patients. Most of the patients had mild effusions (12.8%). Mean CD4 count with pericardial effusion was 72 + 103.03 (n = 12) and mean CD4 count without pericardial effusion was 237.3 + 211.5. p < 0.0001.
4. Discussion
Seventy consecutive patients with HIV infection hospitalized to the inpatients ward of the department of Medicine were included in the current study. Majority of the patients, 71% males and 67% females, belonged to the young age group of 26 to 40 years. It was in concordance with NACO annual report 2009 - 2010 [10]. The NACO report has shown that most PLHA in India were young adults. Men were more affected than females by a ratio of 2:1. 45 patients (64.3%) were males and 25 patients (35.7%) were females. The gender difference was also at par with NACO report, where 39% of the total HIV patients in India were females, 3.5% were children and the rest 57.5% were males [10]. Sexual contact was the most common mode of transmission (94%) with heterosexuality being the cause for 92%. The homosexual route of transmission was 2.8% while infected blood transfusion was responsible for 2.8% of cases in our study. Globally, sexual contact is the commonest mode of transmission [6]. In the west, 75% of newly affected males are due to homosexuality, 14% consequent to heterosexual contact, 8% due to injection drug use and a meager 3% due to other modes of transmission [6]. The socio-cultural picture in India is different from the West and therefore homosexual mode of transmission was less in this study as compared to the West [6]. However, our data is comparable with NACO annual report 2009-2010 [10] where

Table 2. Association of 2D echocardiographic findings with CD4 count.
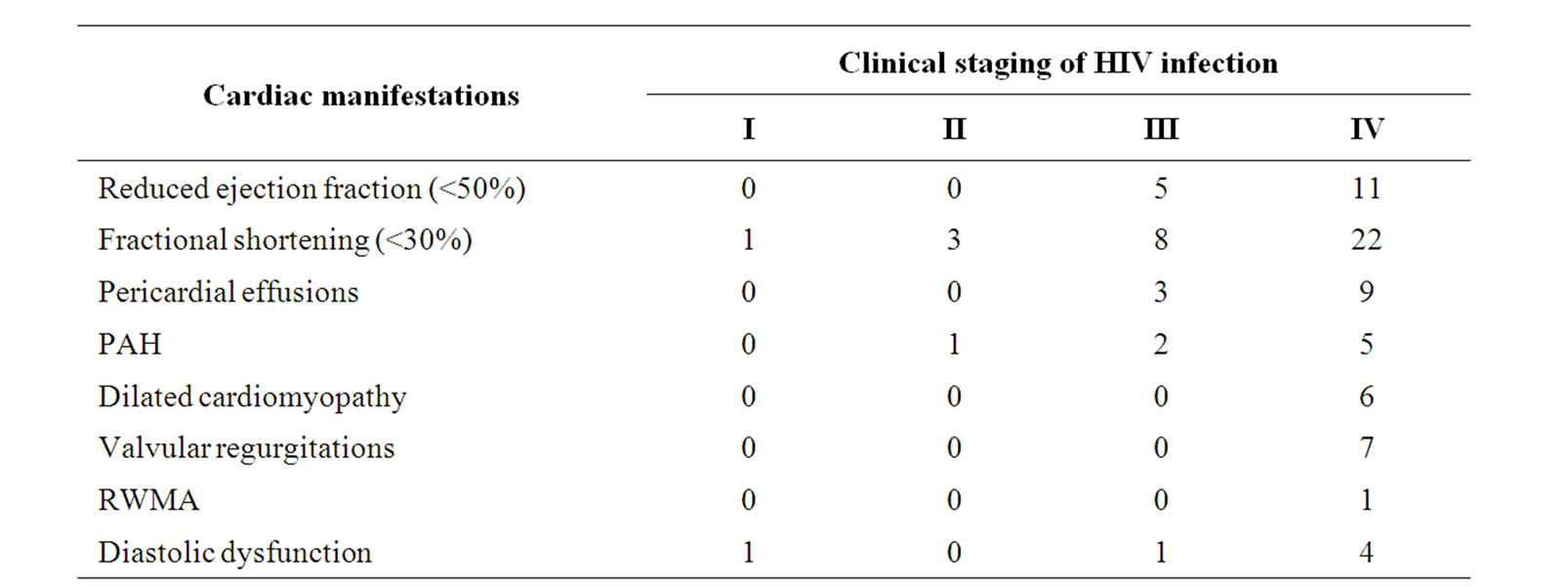
Table 3. Association of 2D echocardiographic findings with clinical staging according to who.
heterosexual route of transmission was 87%. This confirms that there is a visible difference in the type of sexual contact responsible for causing HIV infection in different population.
Clinical features such as fever 74.3%, cough 30%, breathlessness 28.6% respectively was similar to as reported in other studies from India [11]. However, most of the symptoms were non specific and could be attributable to secondary pulmonary infections [11]. CD4 count was less than 50/micrL in 28.6% of cases while 32.9% of cases had CD4 count in between 50 - 200/microL. Thus most of the cases studied had CD4 count less than 200/microL and categorized under WHO revised clinical stage 4 (40%) and clinical stage 3 (35.7%) respectively. The reason behind low CD4 count is that, the patients studied were hospitalized case as they had presented in advanced stage of the disease.
Echocardiographic abnormalities are summarized in Table 1. The study showed that echocardiographic abnormalities was common in HIV infected patients. Echocardiographic abnormalities were seen in 55.7% of cases in the present study while it was 42.3% in studies done by other workers from India [8]. Commonest manifestation found was reduction in FS. This was consistent with studies done in Europe by Corrallo et al. [5] as well as from India by Aggarwal et al. [8].
Reduction in EF was seen in 22.8% of cases in the present study. Reduction in ejection fraction without global hypokinesia or chamber enlargement but without any symptom, probably represented a mild form of cardiac disease that will progress to a clinically evident form of dilated cardiomyopathy [5]. Dilated cardiomyopathy was seen in 8.5% of the cases whereas studies published by Moreno et al [12] and Hakim et al. [13] had detected 6% and 5% respectively. Pulmonary artery hypertension was noted in 8 cases (11.4%) which was higher than normal population and comparable to studies done by Pellicelli AM et al. [14] and Mehta et al. [15] who also found higher incidence of pulmonary artery hypertension in HIV patients than normal population.
Diastolic dysfunction was seen in 8.5% of cases, consistent with the study done by Hakim et al. [13].An increased incidence of myocardial infarction in patients with HIV infection has recently been identified as per Mary et al. [16] and Klein et al. [17] .Both the studies related it to the long term use of protease inhibitors. One patient in this study with CD4 count of 27 and on anti retro-viral therapy for three years had RWMA in apical and anterior wall. The marked absence of endocardial involvement in this study may be related to the low prevalence of intravenous drug abusers [18]. The incidence of valvular regurgitations observed in the present study was similar to that noted as in general population suggests that it was a chance finding [18].
Pericardial effusion was seen in 17.4% of cases which is at par with Indian studies done by Aggarwal et al. (11.5%) and studies done at United States by Himelman et al. [8,19]. The pericardial effusion detected was often small in amount and without any hemodynamic significance. Pericardial effusion in HIV patients may be marker of end stage HIV infection because it is associated with low CD4 count. Table 3 depicts the association of echocardiographic abnormalities with WHO revised clinical staging. Most of the echocardiographic abnormalities were seen in WHO clinical stage 4 which at par with studies done by Khunnawat et al. [20] and Lipshultz SE et al. [21], who have shown that cardiac manifestations occur late in the course of the disease.
Previous studies have shown that HIV related cardiac manifestations are often seen in a state of severe immunosuppression with low CD4 Count (CD4 < 200/microL) [18,22,23]. This study (Table 2) showed that patients with CD4 count less than 200/microL had a high prevalence of echocardiographic abnormalities than those with CD4 count more than 200/microL. As illustrated in figures 1(a) and (b), CD4 count had a significant positive correlation with reduction in EF and FS (p < 0.001 and p < 0.002, respectively). Various studies agree that the most important factor in development of cardiac abnormalities is the level of immunosuppression and there is tight correlation between CD4 count and echocardiographic abnormalities, which is also demonstrated in the present study [8,22,24]. As shown in Table 4, statistically significant correlation was seen between echocardiographic abnormalities and CD4 count (p < 0.0001).

Table 4. mean pattern of study parameters with cardiac dysfunction and their correlation.
 (a)
(a) (a)
(a)
Figure 1. (a) and (b) depicts that CD4 count/microL has significant correlation with Ejection Fraction (p < 0.001) and Fractional Shortening (p value < 0.002).
5. Conclusion
HIV infection in India is more consequent to heterosexual contact than other modes of transmission identified in western population. The results of the study indicate that cardiovascular abnormalities in HIV infected patients are common and can occur without any clinical manifestation. The most common cardiac manifestations being reduction in EF, FS, pericardial effusions, dilated cardiomyopathy and diastolic dysfunction. They are associated with low CD4 count and occur in advanced stage of the disease, especially in Stage 4. Echocardiography is a useful technique for the early recognition and treatment of cardiac dysfunction in such patients. Further clinicopathological studies are required to clarify the role of HIV virus and opportunistic infections in the pathogenesis of cardiac pathology found in HIV infected patients.
REFERENCES
- UNAIDS and WHO, “AIDS Epidemic Update,” Joint United Nations Programme on HIV/AIDS and World Health Organization, Geneva, 2009.
- R. Steinbrook, “HIV in India—A Downsized Epidemic,” The New England Journal of Medicine, Vol. 358, No. 2, 2008, pp. 107-109. doi:10.1056/NEJMp0708474
- P. Rerkpattanapipat and N. Woongpraparut, “Cardiac Manifestations of Acquired Immunodeficiency Syndrome,” Archives of Internal Medicine, Vol. 160 No. 5, 2000, pp. 602-608. doi:10.1001/archinte.160.5.602
- S. Kaul, M. C. Fishbein and R. J. SIEGEL, “Cardiac Manifestations of Acquired Immune Deficiency Syndrome,” American Heart Journal, Vol. 122, No. 2, 1991, pp. 535- 544. doi:10.1016/0002-8703(91)91013-D
- S. Corallo, M. R. Mutinelli, M. Moroni, et al., “Echocardiography Detects Myocardial Damage in AIDS,” European Heart Journal, Vol. 9, No. 8, 1998, pp. 887-892.
- A. S. Fauci and H. C. Lane, “Human Immunodeficiency Virus Disease: AIDS and Related Disorders,” In: A. S. Fauci, et al., Eds., Harrison’s Principles of Internal Medicine, 18th Edition, McGraw Hill Company Inc., New York/Chicago/New Delhi, 2011, pp. 1506-1587.
- D. J. Sahn, A. De Maria, J. Kissilo and A. Weyman, “Recommendations Regarding Quantitations in M—Mode Echo Cardiography,” Circulation, Vol. 58, No. 6, 1988, pp. 1072-1083.
- P. Aggarwal, A. Sharma, R. Bhardwaj and R. Rainam, “Myocardial Dysfunction in Human Immunodeficiency virus Infection: An Echocardiographic Study,” Journal of the Association of Physicians of India, Vol. 57, 2009, pp. 745-746.
- World Health Organization, “Interim Who Clinical Staging of HIV/AIDS Case Definitions for Surveillance,” 2005. http://www.who.int/hiv/pub/guidelines/clinicalstaging.pdf
- National AIDS Control Organization, “A Press Release on HIV Estimates 2009,” 2010. http://www.nacooline.org/facts
- B. Anita, et al., “Cardiac Dysfunction Associated with HIV Infection,” Journal of the Association of Physicians of India, Vol. 51, 2003, p. 1182.
- R. Moreno, J. P. Villacastin, H. Bueno, et al., “Clinical and Echocardiographic Findings in HIV Patients with Pericardial Effusion,” Cardiology, Vol. 88, No. 5, 1997, pp. 397-400. doi:10.1159/000177367
- J. G. Hakim, J. A. Matenga and S. Siziya, “Myocardial Dysfunction in HIV Infection: An Echocardiographic Study of 157 Patients in Hospital in Zimbabwe,” Heart, Vol. 76, No. 2, 1996, pp. 161-165. doi:10.1136/hrt.76.2.161
- A. M. Pellicelli, G. Barbaro, F. Palmieri, E. Girardi, C. D’Ambrosio, A. Rianda, G. Barbarini, D. Frigiotti, M. C. Borgia and N. Petrosillo, “Primary Pulmonary Hypertension in HIV Patients: A Systematic Review,” Angiology, Vol. 52, No. 1, 2001, pp. 31-41.
- N. J. Mehta, I. A. Khan, R. N. Mehta and D. A. Sepkowitz, “HIV-Related Pulmonary Hypertension: Analytic Review of 131 Cases,” Chest, Vol. 118, No. 4, 2000, pp. 1133-1141. doi:10.1378/chest.118.4.1133
- M. Mary-Krause, L. Cotter, M. Partisani, A. Simon, D. Costagliola, “Impact of Protease Inhibitor Treatment on Myocardial Infarction in HIV infected Men,” 8th Conference on Retro Virus and Opportunistic Infections, Chicago, 4-8 February 2001.
- D. Klein, L. B. Hurley, C. P. Quesenberry Jr. and S. Sidney, “Do Protease Inhibitors Increase the Risk for Coronary Heart Disease in Patients with HIV-1 Infection,” Journal of Acquired Immune Deficiency Syndromes, Vol. 30, No. 5, 2002, pp. 471-477. doi:10.1097/00126334-200208150-00002
- S. Castro, G. Migliau, A. Silvestri, et al., “Heart Involvement in AIDS: A Prospective Study during Various Stages of Diseases,” European Heart Journal, Vol. 13, 1992, pp. 1452-1459.
- R. B. Himelman, W. S. Chung, D. N. Chernoff, N. B. Schiller and H. Hollander, “Cardiac Manifestations of Human Immunodeficiency Virus Infection: A Two-Dimensional Echocardiographic Study,” Journal of the American College of Cardiology, Vol. 13, No. 5, 1989, 1030-1036. doi:10.1016/0735-1097(89)90256-8
- C. Khunnawat, S. Mukerji, D. Havlichek, R. Touma and G. S. Abela, “Cardiovascular Manifestations in Human Immunodeficiency Virus-Infected Patients, American Journal of Cardiology, Vol. 103, No. 2, 2009, pp. 292-293.
- K. M. Zareba and S. E. Lipshultz, “Cardiovascular Complications in Patients with HIV Infection,” Current Infectious Disease Reports, Vol. 5, No. 6, 2003, pp. 513-520. doi:10.1007/s11908-003-0096-5
- G. Barbaro, “Cardiovascular Manifestations of HIV Infection,” Circulation, Vol. 106, 2002, pp. 1420-1425. doi:10.1161/01.CIR.0000031704.78200.59
- S. B. Devi, Th. S. D. Singh and R. Ningshen, “Cardovascular Manfestations Of HIV infection/AIDS,” Postgraduate Medicine, Association of Physicians of India, Mumbai, Vol. 55, 2012, pp. 537-550.
- N. Reinsch, P. Kahlert, S. Esser, A. Sundermeyer, K. Neuhaus, N. Brockmeyer, A. Potthoff, R. Erbel and T. Buck, “Till Neumann Echocardiographic Findings and Abnormalities in HIV Infected Patients: Results from a Large, Prospective, Multicenter HIV-Heart Study,” American Journal of Cardiovascular Disease, Vol. 1, No. 2, 2011, pp. 176-184.
NOTES
*Corresponding author.