Open Journal of Preventive Medicine
Vol.3 No.9(2013), Article ID:40391,9 pages DOI:10.4236/ojpm.2013.39070
Motivations and barriers to utilizing adult walking buses: An examination of demographic correlates of willingness to participate in a community-based walking program
![]()
1Department of Sociology, University of Alabama at Birmingham, Birmingham, USA; *Corresponding Author: amilner@uab.edu
2Department of Civil, Construction, and Environmental Engineering, University of Alabama at Birmingham, Birmingham, USA
Copyright © 2013 Adrienne Milner et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 17 October 2013; revised 18 November 2013; accepted 29 November 2013
Keywords: Walking Bus; Exercise Motivations; Exercise Barriers; Perceptions; Birmingham; Alabama
ABSTRACT
Walking buses are a way to increase physical activity by encouraging people to walk rather than rely on motorized forms of transportation. Several communities support walking school buses as an alternative mode of pupil transportation to schools. A possible extension of this concept is the introduction of adult walking buses. Given the novelty of the concept, very little is currently known about the public’s perceptions regarding adult walking buses and their potential effectiveness to increase physical activity and decrease obesity among adults. To bridge this gap, this study examined motivations and barriers to participation in an adult walking bus program in Birmingham, Alabama using a comprehensive questionnaire survey. Analysis of over 340 responses revealed a positive reception of the concept among the survey responders. More specifically, 60.1% of the sample reported they would definitely or probably participate in a walking bus program. Results from nested ordinal logistic regression analysis indicate that health benefits are the strongest motivation for willingness to participate in a walking bus program. Sensitivity to environmental issues is also a significant predictor of willingness to participate across models. The most significant barrier to willingness to participate in a walking bus program is limited time. The significance of demographic variables (obesity, race/ ethnicity, and age) as predictors of willingness to participate is reduced once motivations and barriers are controlled. In conclusion, the positive response to the program among our sample is encouraging and suggests that adult walking buses should be explored further as an active alternative transportation option with a potential to improve the health and wellbeing of participants.
1. INTRODUCTION
Obesity is on the rise nationwide and is a particularly serious concern in the state of Alabama. Data from the 2012 Behavioral Risk Factor Surveillance System (BRFSS) reveal a 30% - 35% self-report obesity rate among Alabama adults [1]. Obesity is the result of excess energy consumption relative to energy expenditures. Thus, lack of physical activity and sedentary lifestyles result in increased obesity and poorer health. Indeed, physical inactivity has been claimed to be the biggest public health problem in the 21st century [2]. According to the Centers for Disease Control and Prevention (CDC), more than 32% of Alabama adults are physically inactive [3]. In order to increase physical activity and combat the obesity epidemic in the state, this study focuses on walking, the simplest, most accessible, and preferred method of physical activity prescribed for the treatment and prevention of obesity [4,5]. Specifically, the study examines whether walking buses are a viable option to influence physical activity and decrease obesity among Alabama adults.
A walking bus is an active form of transportation that encourages people to walk as a way to reach their destinations, rather than rely on personal or public motor vehicles. Like traditional buses, walking buses have designated routes, stops, and drivers who lead the group of walking passengers to their destination. A similar concept (namely the walking school bus) has been used widely as an alternative mode of transportation for school children. Research in Canada, New Zealand, the UK, and in urban communities in the US has shown that children’s walking school buses effectively promote weight loss, academic achievement, pedestrian safety, and social cohesion [6-9].
This study examines the potential application of this successful concept to adults, where similar health benefits are expected to be achieved since walking helps individuals manage their weight, reduce their risk and manage type II diabetes, lower their blood pressure, and lower low-density lipoprotein (LDL) cholesterol [10].
It can be argued that walking buses are even more beneficial for adults than children because adults, for the most part, are more sedentary than children. Walking bus participation may be especially attractive to adults because aside from encouraging physical activity, walking buses have the added advantages of raising community awareness of how walkable a community is and where improvements can be made, providing social networking opportunities, decreasing crime, reducing traffic congestion and pollution, and minimizing transportation costs. Walking as a group may be a feasible option to increase physical activity among Alabama adults because past research indicates that opportunities to exercise in a group were the most preferred method of support to increase physical activity among inactive adults [4]. Coleman et al. [11] found that assigning sedentary individuals to walking groups significantly improved their body composition, cardiovascular health, and systolic blood pressure. Interestingly, these improvements were sustained over time where participants indicated that “making walking part of my lifestyle” was the most important factor in maintaining their walking habits. A walking bus program does exactly that: rather than forces individuals to exercise, it incorporates exercise into their daily lives. Additionally, walking buses may increase physical activity due to the highly visible nature of walking as a way to reach destinations, and research has shown that belief that one’s neighbors are physically active is also positively associated with walking [12,13].
2. BACKGROUND
Casey, De Civita, and Dasgupta [14] found that in a supervised exercise program of individuals with type 2 diabetes, motivation was the most critical factor in exercising both during and following the program, and postprogram, walking emerged as most frequent form of activity. Past research indicates that traditional goals of health promotion are secondary in motivation for participating in walking programs, where social relationships are more important. In their research on mall walking among older adults, researchers [15,16] found that routine participation among older adults was dictated by social connections with other participants rather than potential for positive returns on health. Prusak and Darst [17] also found that when given a choice of nine different types of walking activities, adolescent girls were significantly more likely to choose social over exercise/fitness and game-like/competitive activities. In fact, fewer than 25% of adolescents in the study of Utter et al. [18] exercised alone.
Aside from social interaction, previous research shows several other motivating factors for walking. For example, Boarnet et al. [19] found that walking in the South Bay area of Los Angeles is motivated by the concentration of local shopping and service destinations in its commercial core. Bopp, Kaczynski, and Wittman [20] found that individuals with eco-friendly attitudes were more likely to walk and bike to work, and these individuals also reported more self-efficacy, fewer barriers, and more motivators for active commuting.
In addition to identifying incentives to walk, previous research has identified various barriers to physical activity and walking in particular. Lee et al. [21] found that barriers to walking in overweight and obese individuals included bad weather, inadequate lighting, lack of shade, unattended dogs, disconnected sidewalks, poor walking surfaces, no interesting places to walk, and no benches. In this research, safety concerns also limited participants’ desire to walk where older individuals feared injury from activity and younger individuals feared traffic accidents. In their research on families that live nearby schools in which their children attend, Ahlport et al. [22] found that interpersonal characteristics of parents and children, environmental characteristics, and environmental and policy characteristics of schools all serve as barriers to walking to school.
Alfonzo [23] argued that there are five levels of walking needs that need to be met in order for individuals to be motivated to walk: feasibility; accessibility; safety; comfort; and pleasure. This hierarchy of needs relates to individuals’ demographic characteristics and living environment, particularly, in terms of race/ethnicity, socioeconomic status, age, and gender. Previous research [24- 27] reveals key differences between racial and ethnic groups in terms of physical activity levels and obesity. Not only is race/ethnicity correlated with socioeconomic status and factors related to built environment that influence physical activity patterns, higher levels of socioeconomic status are associated with higher levels of exercise [18,28]. Additionally, leisure time physical activity [29] and bouts of moderate to vigorous physical activity is highest among non-Hispanic Whites compared to African-Americans and Mexican-Americans [30].
Along with race/ethnicity and socioeconomic status, studies indicate gender differences in walking behavior. Clifton and Livi [31] found that women are more sensitive to safety issues (both traffic and crime) and more likely to walk than men, but men walk longer distances. In this study, differences in motivation were also gendered, where the main reason men chose to walk was convenience while for women, it was health benefits. Helling [32] also found gender as well as age differences in walking, where middle-aged men were the least likely to engage in 30 minutes or more of walking or biking per day, though younger and older men were more likely than similar aged women to walk or bike. Like Clifton and Livi [31], Helling [32] found that women make shorter trips (both in terms of miles and minutes) beginning in middle age.
3. OBJECTIVE
Based on these previous findings, the present study examines motivations and barriers to participating in an adult walking bus program and how demographic factors affect willingness of participation. Specifically, the current study seeks to address how race/ethnicity, socioeconomic status, age, gender, and obesity relate to different reasons individuals are likely to participate and not participate in an adult walking bus program.
4. METHOD
In order to better understand perceptions, attitudes, and potential interest for an adult walking bus program, we collected data on the motivations for participating and not participating in such a program in the vicinity of the University of Alabama at Birmingham (UAB) in Birmingham, Alabama through the use of a custom made questionnaire survey.
4.1. Population Studied
The data for the present study were collected between June and July 2013 in two ways using paper and online survey tools. More specifically, 2614 paper surveys were delivered to residences in targeted census tracts that are within a two mile radius of the midpoint of the triangle between three Birmingham neighborhoods, namely Southside, Lakeview, and Downtown. These three neighborhoods are all less than 1.5 miles (less than a 30 minute walk) from one another and each contain desirable walking destinations (employment, restaurants, shopping, entertainment venues, etc.). An online survey was also administered to faculty, staff, and students at UAB which is central to all three neighborhoods and makes up a large portion of the city’s population (over 25,000 UAB employees and 17,500 UAB students) and structure (spanning over 80 blocks). The research team received a total of 341 completed surveys (115 paper and 226 online survey responses). However, 17.4% of the surveys contained missing information on one or more of the study variables. List-wise deletion is employed leaving a final sample size of 280.
4.2. Measures
The survey included questions about how interested individuals are in a walking bus program as well as specific reasons for participation/non-participation. The question, “How likely would you be to participate in a walking bus program?” was measured on a 5-point likert scale (1 = would never participate; 2 = probably would not participate; 3 = am neutral about participating; 4 = probably would participate; 5 = would definitely participate). There were eight questions assessing specific motivations for participating in a walking bus program which were also measured on a 5-point likert scale ranging from 5 = extremely important to 1 = not important at all. Respondents were asked: “How important are the following reasons for participating in a walking bus program to you: “to lose weight”; “to get some exercise”; “to meet new people”; “to reduce crime (e.g. drunk driving) in my community”; “to help the environment”; “to minimize transportation costs”; “to improve the walkability of my neighborhood”; “because I would already like to walk, but fear walking alone.”
Questions about perceived barriers to using a walking bus were also included and were measured on a five pointlikert scale ranging from 5 = extremely important to 1 = not important at all. Barriers include no desire to increase physical activity, limited time, physical health does not permit walking, and do not see the usefulness of walking buses The survey also included several socio-demographic characteristics that are known correlates of walking such as respondents’ race/ethnicity (non-Hispanic white and non-white), age (in continuous years), education(college graduate and non-college graduate), obesity status (BMI greater than or equal to 30 based off self-reported height and weight, gender (female = 1), and income bracket before taxes measured on a seven point scale and treated as continuous (1 = $0 - $24,999; 2 = $25,000 - $49,999; 3 = $50,000 - $74,999; 4 = $75,000 - $9999; 5 = $100,000 - $149,9999; 6 = $150,000 - $199,999; 7 = $200,000 or above).
4.3. Analysis
The study first examined the percentage of respondents who stated that the motivation or barrier is extremely important (=5) for their participation or nonparticipation in a walking bus program. Next, means and percentages were computed for all variables by race/ ethnicity and for the total sample so that variation in participation, motivations, and barriers can be examined by race/ethnicity. Exploratory factor analysis suggests that the reasons for participation “to lose weight” and “to get some exercise” be combined to create a measure of health reasons so this is done by summing the two measures and dividing the sum by the number of measures (two). This approach was adopted in the study; however, all other motivations and barriers were examined separately. Lastly, we estimate nested ordinal logistic models predicting walking bus participation. The first model included the motivations and barriers for walking bus participation. The second model examined how sociodemographic characteristics influence willingness to participate in a walking bus program, and the third model includes both the motivations and barriers and also the socio-demographic characteristics to examine mediation between the two sets of factors.
5. RESULTS
Table 1 displays the percentage of respondents who stated that the motivation or barrier is extremely important for their participation or non-participation in the walking bus program.
The most common motivation cited as extremely important is exercise (45.2% of the total sample). Additionally, improving the walkability of the neighborhood, losing weight, and helping the environment are also common reasons stated for walking bus participation (35.0%, 30.8%, and 30.8% respectively). The most common barrier to walking bus participation is limited time (21.3%
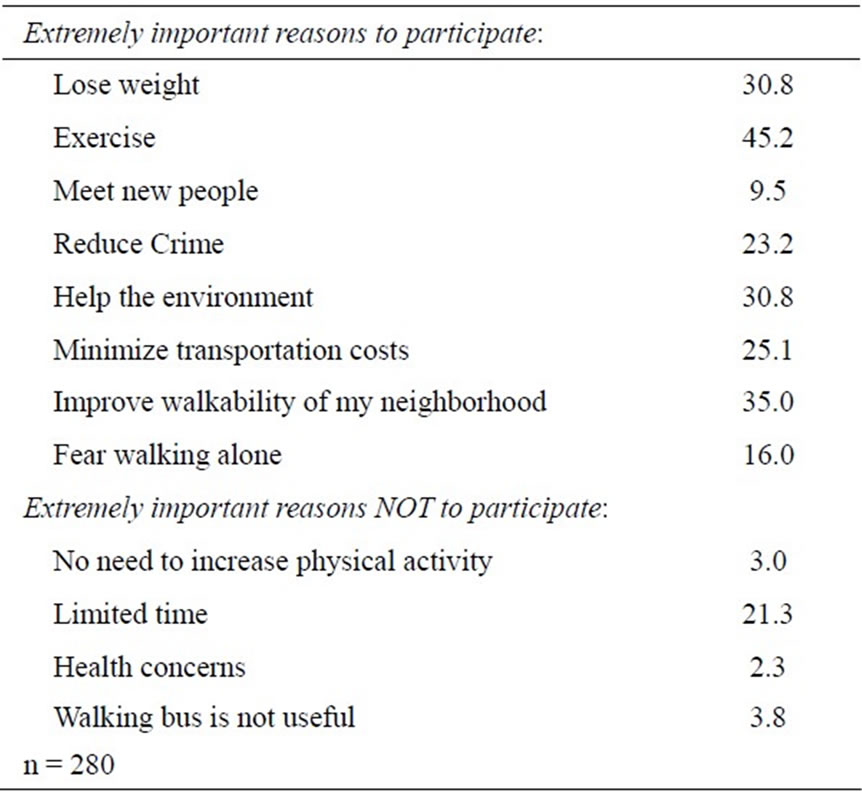
Table 1. Motivations for walking bus participation in Birmingham, Alabama.
of the sample stated that this barrier is extremely important).
Table 2 displays the percentages and means for all study variables for the whole sample and by race/ethnicity. We find a generally positive response to the idea of a walking bus program. More specifically, 60.1% of the sample said they would definitely or probably participate in a walking bus program and this is especially true among non-Whites, 77.7% of which reported that they probably or definitely would participate. Respondents who indicated that they probably or definitely would participate in a walking bus program were telephoned and over 95% verbally consented to participating in a pilot walking bus program.
As reflected in Table 1, health reasons appear to be an important motivation for participating in a walking bus program, especially among non-Whites. Among Whites, improving the walkability of the neighborhood, followed by helping the environment, appear to be the most important motivations. Additionally, fear of walking alone appears to be a more important motivation for nonWhites compared to Whites. 27.9% of the sample is obese, and non-Whites are more likely to be obese than Whites (41.7% compared to 23.1%). The sample is mostly white (74.3%), female (80%), and highly educated (75.7% have at least a four year degree), which is likely due to the proximity of samples to the University of Alabama at Birmingham campus. Non-white study respondents have lower education, lower income, and are more likely to be female compared to Whites.
Table 3 presents the ordinal logistic regression models predicting willingness to participate in a walking bus program. Model 1 contains the motivations and barriers for walking bus participation and these factors explain roughly 21% of the variation in willingness of participation in a walking bus program. Health reasons are the strongest motivator for willingness to participate in a walking bus program (OR: 1.85, 95% CI: 1.47 - 2.34). Desire to help the environment and desire to meet new people also increase the likelihood of willingness to participate (OR: 1.39, 95% CI: 1.05 - 1.84 and OR: 1.23, 95% CI 1.00 - 1.52).
Of the barriers to participation, limited time has the strongest association with willingness to participate in a walking bus program (OR: 0.55, 95% CI 0.45 - 0.66) followed by not finding walking busses useful (OR: 0.69, 95% CI 0.54 - 0.88). Though improving the walkability of the neighborhood is often indicated as an extremely important reason to participate in walking buses, this motivation is not significant once other motivations are controlled. Specifically, helping the environment as a motivation reduces the impact of the motivation to increase the walkability of my neighborhood to non-significance.
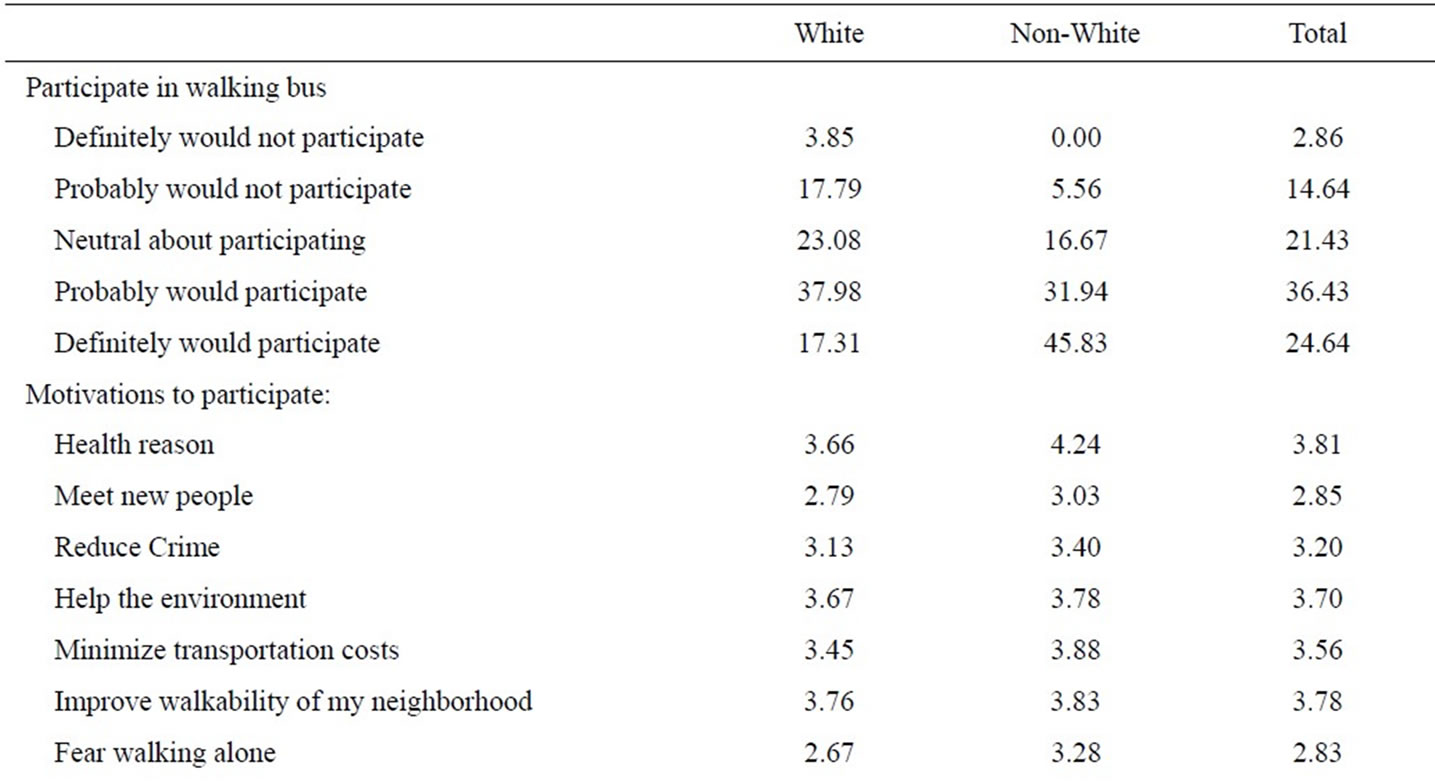
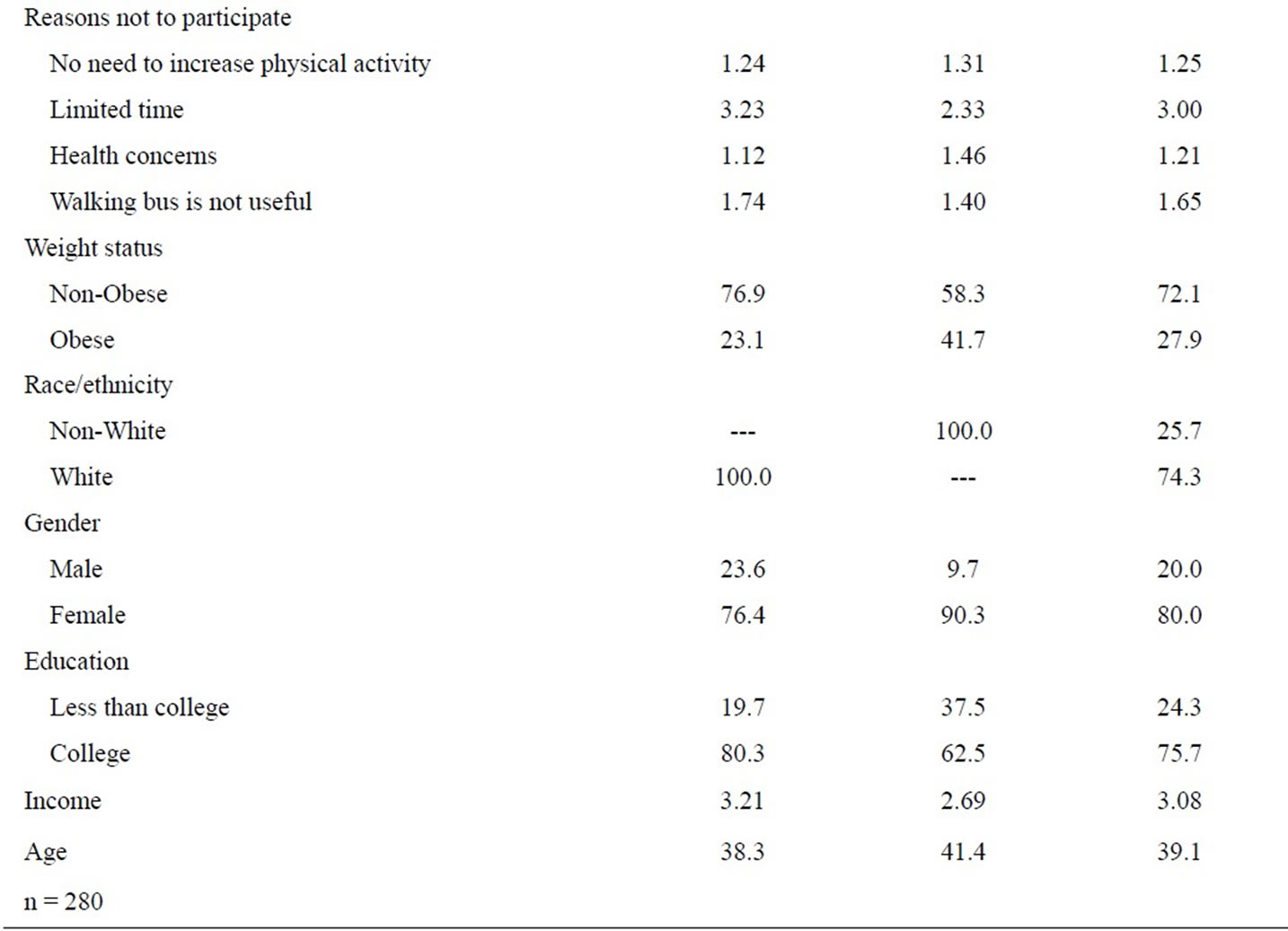
Table 2. Means and percentages of the study variables for the total sample and by race/ethnicity.
Model 2 contains only the socio-demographic characteristics and explains about 7% of the variation in willingness to participate in a walking bus program. We find that being obese and being older increases the likelihood of willingness to participate (OR: 1.88, 95% CI 1.13 - 3.14 and OR: 1.04, 95% CI 1.02 - 1.06, respectively). Additionally, Whites are less likely to want to participate compared to non-Whites and having a higher income is associated with a lower likelihood of wanting to participate (OR: 0.39, 95% CI 0.23 - 0.67 and OR: 0.83 95% CI 0.72 - 0.96).
Model 3 includes the full set of covariates; motivations, barriers, and socio-demographic characteristics and explains about 22% of the variation in willingness to participate in a walking bus program. Examining the mediation effects on motivations and barriers to walking bus participation we find that including the socio-demographic factors reduces the OR for health reasons and meeting new people as a motivation for walking bus participation. The OR for health reasons is reduced to 1.69
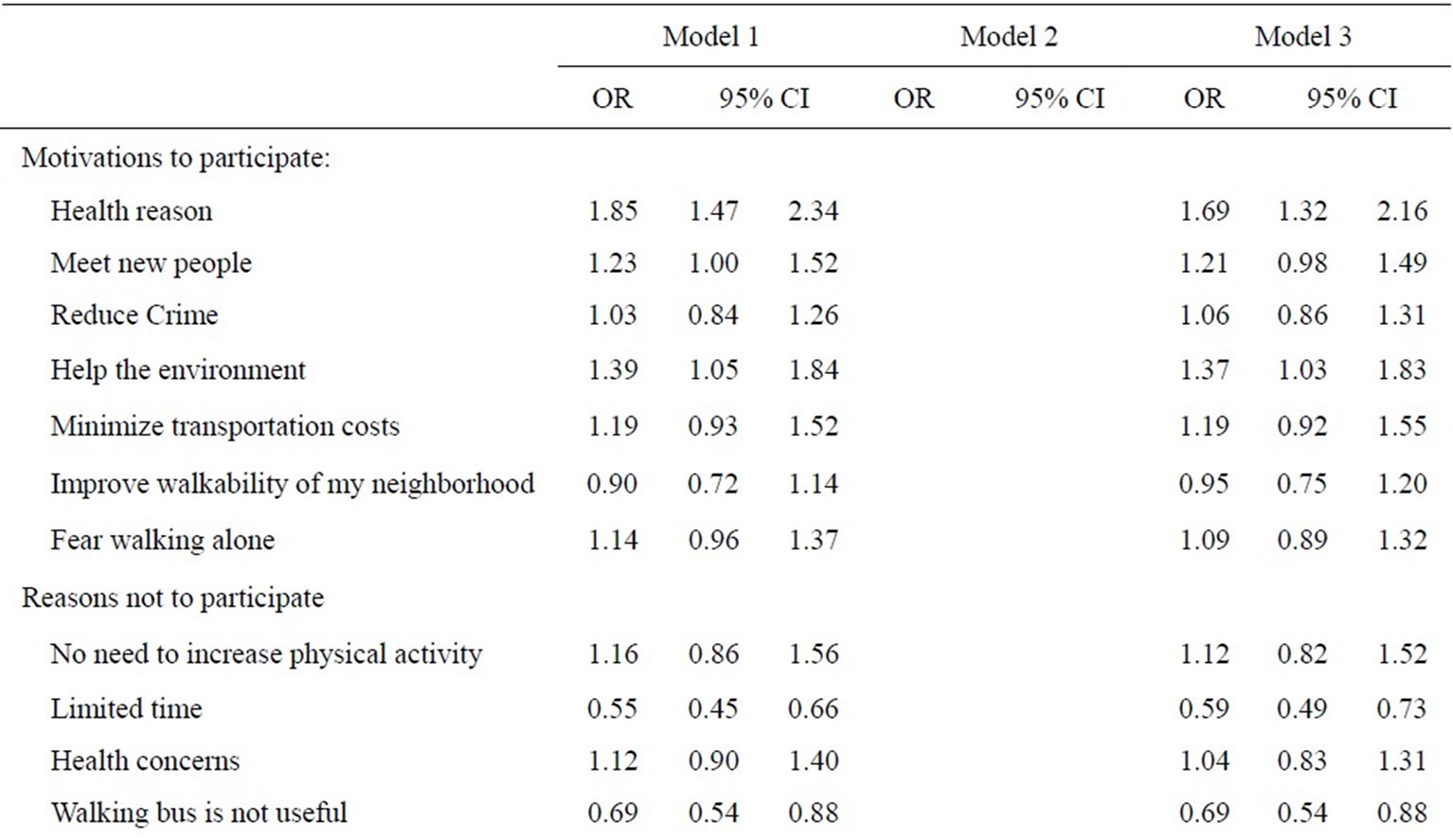
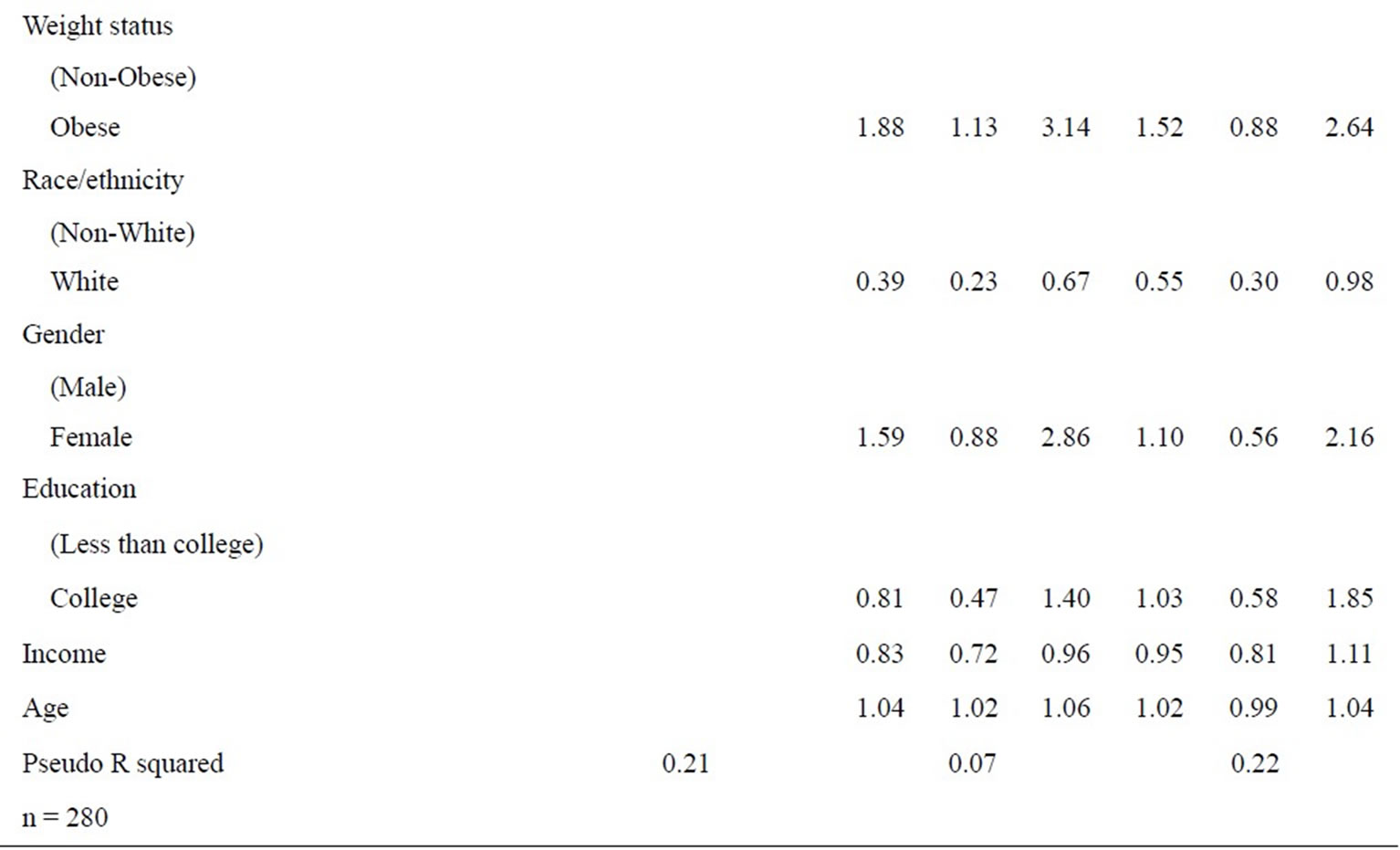
Table 3. Odds ratios (OR) and 95% cofidence intervals (CI) for ordinal logit predicting walking bus participation (1 = not at likely to 5 = extremely likely) in Birmingham, Alabama.
(95% CI 1.32 - 2.16) in Model 3 from 1.85 in Model 1, though the confidence interval does not include one, indicating it is still significantly associated with willingness to participate. The OR for meeting new people is no longer significant and is reduced to 1.21 (95% CI: 0.98 - 1.49) in Model 3 compared to OR: 1.23 in Model 1 that did not control for socio-demographic factors. Including the socio-demographic characteristics does little to the ORs for barriers. Additionally, we find that the motivations and barriers mediate the significant associations found in Model 2 for the socio-demographic factors. The 95% CI for obesity, age, and income now all include one and are no longer significantly associated with willingness to participate. Controlling for health reasons for willingness to participate in a walking bus program reduces obesity to non-significance and controlling for limited time reduces the association for income. Controlling for the barrier of health concerns reduces age to non-significance.
6. DISCUSSION
The analysis of the data showed that motivations and barriers to walking bus participation identified in this study explain about 21% of the variation in willingness to participate in an adult walking bus program. Health reasons and environment considerations were strong motivators for wanting to participate, while limited time is the most common barrier to walking bus participation.
It was also observed that respondents with higher social status (income and race/ethnicity) are less likely to want to use a walking bus though the barrier limited time explains the relationship between willingness to participate and income. Perhaps this finding contradicts previous research suggesting higher socioeconomic status (SES) results in greater levels of exercise because higher social status individuals in the current study may already have access to exercise facilities, such as a gym, and have an exercise routine in place. This may limit their time to utilize the walking buses. In addition, higher SES individuals in the current study are more likely to have access to private means of transportation, which may limit their desire to participate in this type of walking program.
However, the results of this survey are promising in that walking bus programs among adults may be a viable way to increase physical activity among non-Whites. Past research has found much lower levels of physical activity among non-Whites compared to Whites [29,30]. Additionally, these groups tend to suffer from more of the co-morbidities related to obesity and inactivity compared to whites [33]. Implementing walking bus programs may be a viable way to increase physical activity among this group that is particularly vulnerable to inactivity and the health risks that it imposes.
Findings from previous studies also indicate that participation in a walking program is often determined by social rather than health factors [15,16,18], however in the present study, once socio-demographic characteristics are controlled, the motivation of meeting new people in willingness to participate in a walking bus program reduces to non-significance. This could be because in previous research, social reasons as motivation for exercise were determined by relationships that were already formed, while in the current study, social motivation was represented by the formation of new relationships.
Several respondents who were telephoned to participate in a follow up walking bus pilot program asked if their significant others, roommates, and/or close friends could also join the program. This suggests that future studies about social motivations for participation in adult walking buses should include an item about whether utilizing the buses with friends, coworkers, or family was an important reason that individuals would participate in the program.
Another possible reason why health and environmental rather than social reasons emerged as the most important motivations for walking bus participation could be due to the uniqueness of our sample. Because of the focus on the UAB community, the sample is highly educated (75.7% have at least a four year degree). The highly-educated nature of the sample could have affected the motivations and willingness to participation in a walking bus program because more highly educated individuals are more likely to be aware of both the benefits of walking and the positive impact of walking on the environment, making health and environmental the strongest motivating factors for willingness to participate in the current study.
7. CONCLUSIONS AND RECOMENDATIONS
This study is the first of its kind to examine the motivations and barriers of participation in an adult walking bus program. The overall positive response to a walking bus program confirmed by the study results suggests that walking buses are a likely viable option for increasing physical activity and decreasing obesity.
Given the strong association between the motivations health and environment and willingness to participate in an adult walking bus program, in order to successfully implement an adult walking bus program, researchers should emphasize these benefits in advertising the program and recruiting potential participants. The results of this study also suggest that researchers should attempt to communicate to potential participants how walking buses save rather than waste time, perhaps by focusing on the way in which walking bus participation incorporates physical activity into individuals’ lives rather than forces them to take a certain amount of time out of their day to devote to exercise.
The main limitation of the study is small sample size. Future research on adult walking buses should attempt to survey a larger number of individuals in order to assess motivations and barriers to participation. A larger sample may also result in significant relationships between socio-demographic factors and willingness of participation that were not evident in the current study. In addition, the results of this study are specific to Birmingham, Alabama, and may not be applicable to populations in other cities. However, the fact that 21% of the variation in willingness to participate in an adult walking bus program was captured by the motivations and barriers listed in our survey suggests a starting place for researchers attempting to develop and implement adult walking bus programs in other geographic areas.
8. ACKNOWLEDGEMENTS
We are grateful to the UAB Minority Health and Health Disparities Research Center, Weight Watchers, Inc., and the One Great Community Council of the UAB Center for Clinical and Translational Science for the financial support that enabled us to complete this project.
REFERENCES
- Behavioral Risk Factor Surveillance System (BRFSS) CDC (2012). http://www.cdc.gov/obesity/data/adult.html
- Blair, S.N. (2009) Physical inactivity: The biggest public health problem of the 21st century. British Journal of Sports Medicine, 43, 1-2.
- CDC (2012) Alabama: State nutrition, physical activity, and obesity profile. http://www.cdc.gov/obesity/stateprograms/fundedstates/pdf/alabama-state-profile.pdf
- Booth, M.L., Bauman, A., Neville, O. and Gore, C.J. (1997) Physical activity preferences, preferred sources of assistance, and perceived barriers to increased activity among physically inactive Australians. Preventive Medicine, 26, 131-137. http://dx.doi.org/10.1006/pmed.1996.9982
- Browning, R.C., Mcgowan, C.P. and Kram, R. (2009) Obesity does not increase external mechanical work per kilogram body mass during walking. Journal of Biomechanics, 42, 2273-2278. http://dx.doi.org/10.1016/j.jbiomech.2009.06.046
- Kearns, R.A., Collins, D.C. and Neuwelt, P.M. (2003) The walking school bus: Extending children’s geographies? Area, 35, 285-292. http://dx.doi.org/10.1111/1475-4762.00177
- Kingham, S. and Ussher, S. (2007) An assessment of the benefits of the walking school bus in Christchurch, New Zealand. Transportation Research Part A: Policy and Practice, 41, 502-510. http://dx.doi.org/10.1016/j.tra.2006.11.008
- Mackett, R.L., Lucas, L., Paskins, J. and Turbin, J. (2003) A methodology for evaluating walking buses as an instrument of urban transport policy. Transport Policy, 10, 179-186. http://dx.doi.org/10.1016/S0967-070X(03)00019-2
- Mendoza, J.A., Levinger, D.D. and Johnston, B.D. (2009) Pilot evaluation of a walking school bus program in a low-income, urban community. BMC Public Health, 9, 122. http://dx.doi.org/10.1186/1471-2458-9-122
- MayoClinic (2013) Walking: Trim your waistline, improve your health. http://www.mayoclinic.com/health/walking/HQ01612
- Coleman, K., Raynor, H.R., Mueller, D.M., Cerny, F.J., Dorn, J.M. and Epstein, L.H. (1999) Providing sedentary adults with choices for meeting their walking goals. Preventive Medicine, 28, 510-519. http://dx.doi.org/10.1006/pmed.1998.0471
- Addy, C.L., Wilson, D.K., Kirtland, K.A., Ainsworth, B.E., Sharpe, P. and Kimsey, D. (2004) Associations of perceived social and physical environmental supports with physical activity and walking behavior. American Journal of Public Health, 94, 440-443. http://dx.doi.org/10.2105/AJPH.94.3.440
- Wilcox, S., Castro, C., King, A.C., Housemann, R. and Brownson, R.C. (2000) Determinants of leisure time physical activity in rural compared with urban older and ethnically diverse women in the United States. Journal of Epidemiology and Community Health, 54, 667-672. http://dx.doi.org/10.1136/jech.54.9.667
- Casey, D., De Civita, M. and Dasgupta, K. (2010) Understanding physical activityfacilitators and barriers during and following a supervised exercise programme in Type 2 diabetes: A qualitative study. Diabetic Medicine, 27, 79- 84.
- Duncan, H.H., Travis, S.S. and Mcauley, W.J. (1995) The meaning of and motivation for mall walking among older adults.Activities, Adaptation & Aging, 19, 37-52. http://dx.doi.org/10.1300/J016v19n01_03
- Travis, S.S., Duncan, H.H. and Mcauley, W.J. (1996) Mall walking. An effective mental health intervention for older adults. Journal of Psychosocial Nursing and Mental Health Services, 34, 36-38.
- Prusak, K. and Darst, P.W. (2002) Effects of types of walking activities on actual choices by adolescent female physical education students. Journal of Teaching in Physical Education, 21, 230-241.
- Utter, J., Denny, S., Robinson, E.M., Ameratunga, S. and Watson, P. (2006) Perceived access to community facilities, social motivation, and physical activity among New Zealand youth. Journal of Adolescent Health, 39, 770- 773. http://dx.doi.org/10.1016/j.jadohealth.2006.04.009
- Boarnet, M.G., Joh, K., Siembab, W., Fulton, W. and Nguyen, M.T. (2011) Retrofitting the suburbs to increase walking: Evidence from a land-use-travel study. Urban Studies, 48, 129-159. http://dx.doi.org/10.1177/0042098010364859
- Bopp, M., Kaczynski, A.T. and Wittman, P. (2011) The relationship of eco-friendly attitudes with walking and biking to work. Journal of Public Health and Management and Practice, 17, E9-E17. http://dx.doi.org/10.1097/PHH.0b013e31821138de
- Lee, C., Ory, M.G., Yoon, J. and Forjuoh, S.N. (2013) Neighborhood walking among overweight and obese adults: Age variations in barriers and motivators. Journal of Community Health, 38, 12-22. http://dx.doi.org/10.1007/s10900-012-9592-6
- Ahlport, K.N., Linnan, L., Vaughn, A., Evenson, K.R. and Ward, D.S. (2008) Barriers to and facilitators of walking and bicycling to school: Formative results from the non-motorized travel study. Health Education Behavior, 35, 221-244. http://dx.doi.org/10.1177/1090198106288794
- Alfonzo, M.A. (2005) To walk or not to walk? The hierarchy of walking needs. Environment and Behavior, 37, 808-836. http://dx.doi.org/10.1177/0013916504274016
- Frank, L.D., Kerr, J., Sallis, J.F., Miles, R. and Chapman, J. (2008) A hierarchy of sociodemographic and environmental correlates of walking and obesity. Preventive Medicine, 47, 172-178. http://dx.doi.org/10.1016/j.ypmed.2008.04.004
- Lovasi, G.S., Hutson, M.A., Guerra, M. and Neckerman, K.M. (2009) Built environments and obesity in disadvantaged populations. Epidemiologic Reviews, 31, 7-20. http://dx.doi.org/10.1093/epirev/mxp005
- Nicklas, B.J., Dennis, K.E., Berman, D.M., Sorkin, J., Ryan, A.S. and Goldberg, A.P. (2003) Lifestyle intervention of hypocaloric dieting and walking reduces abdominal obesity and improves coronary heart disease risk factors in obese, postmenopausal, African-American and Caucasian women. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 58, M181- M189. http://dx.doi.org/10.1093/gerona/58.2.M181
- Wen, L.M., Orr, N., Millet, C. and Rissel, C. (2006) Driving to work and overweight and obesity: Findings from the 2003 New South Wales Health Survey, Australia. International Journal of Obesity, 30, 782-786. http://dx.doi.org/10.1038/sj.ijo.0803199
- Gordon-Larsen, P., Nelson, M.C., Page, P. and Popkin, B.M. (2006) Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics, 117, 417-424. http://dx.doi.org/10.1542/peds.2005-0058
- Crespo, C.J., Smit, E., Anderson, R.E., Carter-Pokras, O. and Ainsworth, B.E. (2000) Race/ethnicity, social class and their relation to physical inactivity during leisure time: Results from the Third National Health and Nutrition Examination Survey, 1988-1994. American Journal of Preventive Medicine, 18, 46-53. http://dx.doi.org/10.1016/S0749-3797(99)00105-1
- Gordon-Larsen, P., McMurray, R.G. and Popkin, B.M. (1999) Adolescent physical activity and inactivity vary by ethnicity: The National Longitudinal Study of Adolescent Health. The Journal of Pediatrics, 135, 301-306. http://dx.doi.org/10.1016/j.amepre.2004.07.006
- Clifton, K.J. and Livi, A.D. (2005) Gender differences in walking behavior, attitudes about walking, and perceptions of the environment in three Maryland communities. Transportation Research Board Conference Proceedings, 2, 79-88.
- Helling, A. (2005) Connection between travel and physiccal activity: Differences by age and gender. Transportation Research Board Conference Proceedings, 2, 77-78.
- Cossrow, N. and Faulkner, B. (2004) Race/ethnic issues in obesity and obesity-related comorbidities. Journal of Clinical Endocrinology and Metabolism, 89, 2590-2594. http://dx.doi.org/10.1210/jc.2004-0339