H. H. Alamdari et al. / J. Biomedical Science and Engineering 6 (2013) 1062-1071
1070
5.2. Experiments
The tests on the prototype device without breathing noise
resulted in very low errors and high SNRs. As expected,
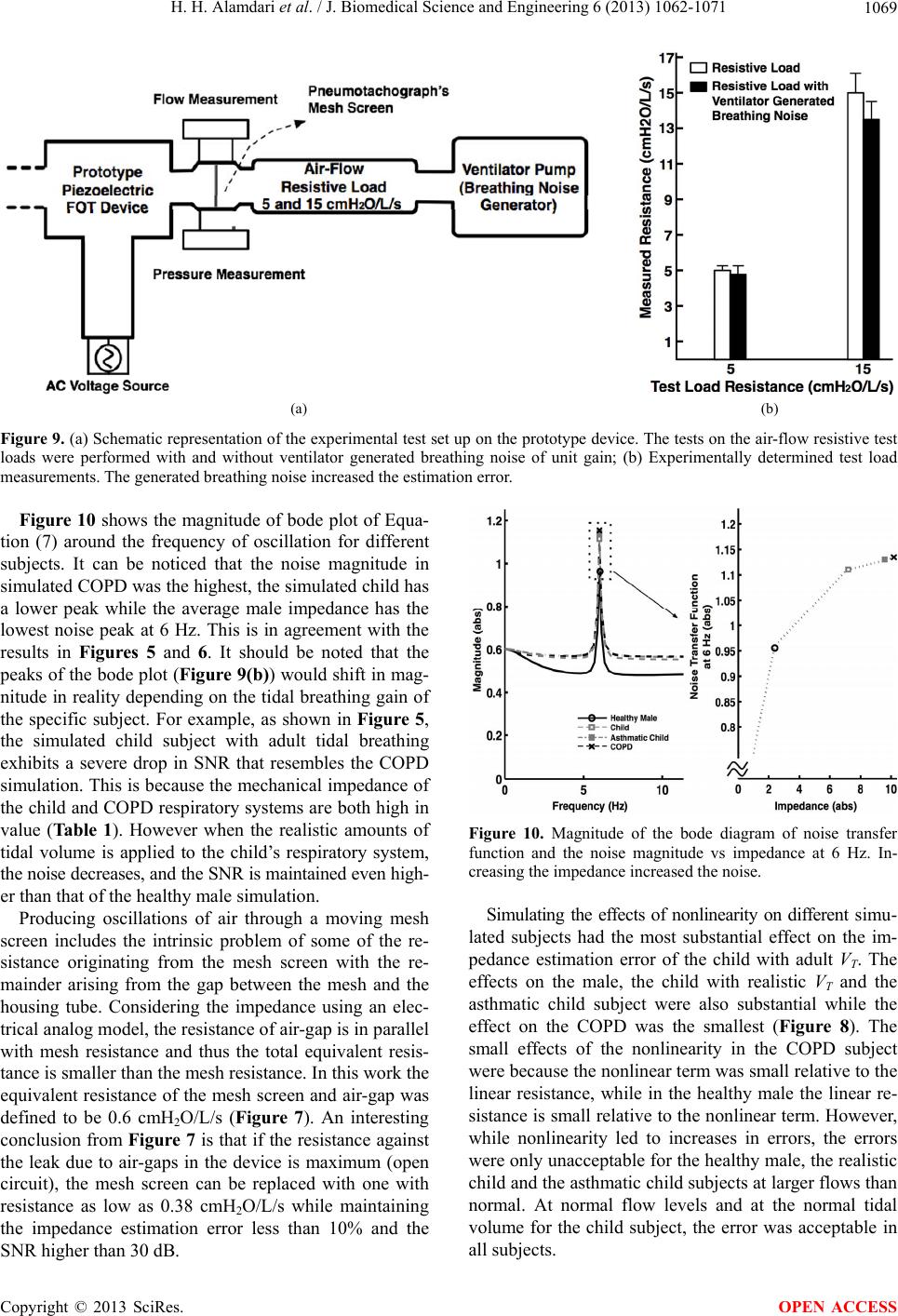
after adding the breathing noise the SNR dropped and
errors increased. However in the case of the 15 cmH2O/L/s
test load which is higher than would be anticipated for
adult subjects, but possible for children with airway ob-
struction [13] the error reached the maximum recom-
mended value (Figure 9(b)). Children fortunately have
lower breathing noise, and thus this design is likely suit-
able for a large range of subjects. These are for normal or
nearly normal tidal volumes. However if measurements
are to be made under larger ventilation conditions such
as with exercise, the reduction in SNR would begin to
cause larger errors in estimating impedance. If this is un-
acceptable then larger oscillatory flows would be recom-
mended using one or a combination of following techni-
ques:
Movement amplification techniques including me-
chanical lever and/or using longer customized piezo-
electric multimurphs and/or using multiple actuators
at the same time for increasing the applicable force.
Using an actuator with higher surface area to generate
higher pressure oscillations.
Reducing the amount of leak due to air-gaps.
6. CONCLUSION
In this paper, for the first time, an oscillometry device
was designed based on optimization in a simulation that
included the device characteristics together with changes
in subject impedance including perturbations from brea-
thing. Although breathing noise reduced the SNR, the per-
formance remained acceptable and demonstrated a useful
design approach that led to the development of a feasible
accurate lightweight portable single frequency FOT de-
vice. Reducing the leak and improving the measurement
accuracy of the transducers as well as modifications in
the oscillating mesh and the actuator can improve the
results from the prototype device.
7. ACKNOWLEDGEMENTS
Hamed Hanafi and Lucas Posada were supported by the NSERC
CREATE program at Dalhousie University, S. A. Bhatawadekar was
supported by the NSERC.
The authors thank Guy Drapeau at Thorasys Medical Systems for his
great feedback especially for experiments. They also thank Andre Be-
zanson for his help with piezoelectric actuators.
REFERENCES
[1] DuBois, A.B., Brody, A.W., Lewis, D.H., Burgess Jr.,
B.F. (1956) Oscillation mechanics of lungs and chest in
man. Journal of Applied Physiology, 8, 587-594.
[2] Dellacà, R.L., Pompilio, P.P., Walker, P.P., Duffy, N., Pe-
dotti, A. and Calverley, P.M. (2009) Effect of bronchodi-
lation on expiratory flow limitation and resting lung me-
chanics in COPD. European Respiratory Journal, 33,
1329-1337.
http://dx.doi.org/10.1183/09031936.00139608
[3] Morita, T. (2003) Miniature piezoelectric motors. Sensors
and Actuators A, 103, 291-300.
http://dx.doi.org/10.1016/S0924-4247(02)00405-3
[4] Uchino, K., Kato, K. and Tohda, M. (1988) Ultrasonic li-
near motors using a multilayered piezoelectric actuator.
Ferroelectrics, 87, 331-334.
http://dx.doi.org/10.1080/00150198808201395
[5] Wang, Q.-M., Du, X.-H., Xu, B.M. and Eric Cross, L.
(1999) Electromechanical coupling and output efficien-
cy of piezoelectric bending actuators. IEEE Transactions
on Ultrasonics, Ferroelectrics, and Frequency Control,
46, 638-646. http://dx.doi.org/10.1109/58.764850
[6] Cheng, H.-M., Ewe, M.T., Bashir, R. and Chiu, G.T.-C.
(2001) Modeling and control of piezoelectric cantilever
beam micro-mirror and micro-laser arrays to reduce im-
age banding in electro photographic processes. Journal of
Micromechanics and Microengineering, 11487-11498.
[7] Goli, J., Smits, J.G. and Ballato, A. (1995) Dynamic bi-
morph matrix of end-loaded bimorphs. IEEE Internatio-
nal Frequency Control Symposium, 794-797.
http://dx.doi.org/10.1109/FREQ.1995.484086
[8] Brown, N., Xuan, W., Salome, C., Berend, N., Hunter, M.,
Musk, A., James, A. and King, G. (2010) Reference equ-
ations for respiratory system resistance and reactance in
adults. Respiratory Physiology & Neurobiology, 172,
162-168. http://dx.doi.org/10.1016/j.resp.2010.05.013
[9] Navajas, D., Alcaraz, J., Peslin, R., Roca, J. and Farre, R.
(2000) Evaluation of a method for assessing respiratory
mechanics during noninvasive ventilation. European Re-
spiratory Journal, 16, 704-709.
http://dx.doi.org/10.1034/j.1399-3003.2000.16d23.x
[10] Van Den Bergh, A. and Kerrebijn, K. (1985) Forced os-
cillation technique. Reference values for resistance and
reactance over a frequency spectrum of 2 - 26 Hz in heal-
thy children aged 2.3 - 12.5 years. Bulletin of European
Physiopathological Respiration, 21, 171-178.
[11] Lall, C.A., Cheng, N., Hernandez, P., Pianosi, P.T., Dali,
Z., Abouzied, A. and Maksym, G.N. (2007) Airway resis-
tance variability and response to bronchodilator in chil-
dren with asthma. European Respiratory Journal, 30,
260-268. http://dx.doi.org/10.1183/09031936.00064006
[12] Barbini, P., Cevenini, G. and Avanzolni, G. (2003) Non-
linear mechanisms determining expiratory flow limitation
in mechanical ventilation: A model-based interpretation.
Annals of Biomedical Engineering, 31, 908-916.
http://dx.doi.org/10.1114/1.1590665
[13] Oostveen, E., MacLeod, D., Lorino, H., Farre, R., Hantos,
Z., Desager, K. and Marchal, F. (2003) On behalf of the
ERS task force on respiratory impedance measurements:
“The forced oscillation technique in clinical practice: Me-
thodology, recommendations and future developments.”
European Respiratory Journal, 22, 1026-1041.
http://dx.doi.org/10.1183/09031936.03.00089403
Copyright © 2013 SciRes. OPEN ACCESS