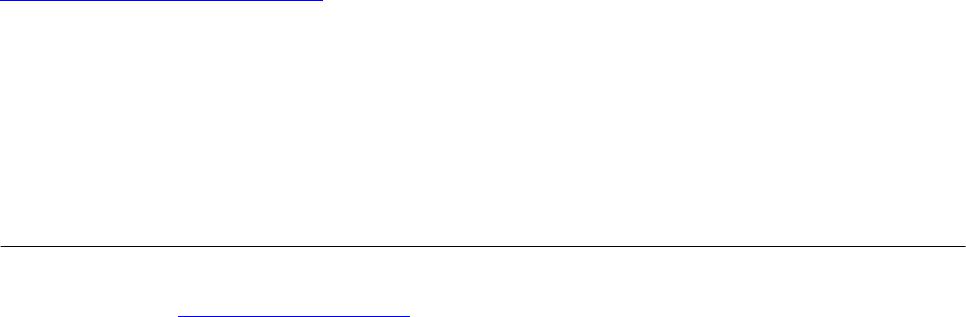
 Vol.1, No.2, 40-51 (2013) Open Journal of Therapy and Rehabilitation http://dx.doi.org/10.4236/ojtr.2013.12008 Action for Rehabilitation from Neurological Injury (ARNI): A pragmatic study of functional training for stroke survivors Cherry Kilbride1, Meriel Norris1, Nicola Theis2, Amir A. Mohagheghi2* 1Centre for Research in Rehabilitation, School of Health Sciences and Social Care, Brunel University, London, UK 2Centre for Sports Medicine and Human Performance , School of Sport and Education, Brunel University, London, UK; *Corresponding Author: amir.mohagheghi@brunel.ac.uk Received 5 June 2013; revised 8 July 2013; accepted 20 July 2013 Copyright © 2013 Cherry Kilbride et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT This study evaluated the effectiveness of a twelve-week community-based functional train- ing on measures of impairment, activity and par- ticipation in a group of stroke survivors. Isome- tric strength of the knee musculature , Centre-O f- Pressure (COP) based measures of balance, Berg Balance Scale (BBS), 10 m walk test, and the Subjective Index of Physical and Social Out come (SIPSO), were recorded at baseline, post- intervention, and after twelve weeks (follow-up). Exercise instructors delivered training once a week in a group format at a community centre. Significant improvement was noted in the BBS (p < 0.002), and 10 m walk speed (p = 0.03) post intervention which remained unchanged at fol- low-up. Total SIPSO score improved signifi- cantly post-intervention (p = 0.044). No other significant differences and no adverse effects were observed. It is possible that functional training provided more opportunity for the im- provement of dynamic aspects of balance con- trol that could be captured by the BBS but not with the traditional measures of balance using COP data. Results also suggest positive effects on the level of participation, and lack of asso- ciation between measures of impairment and activity. Community based functional training could be effective and used to extend access to rehabilitation services beyond the acute and sub-acute stages after st ro ke. Keywords: Balance; Centre-of-Pressure; Functional Training; Hemiplegia; ICF; Rehabilitation; Strength; Stroke 1. INTRODUCTION Stroke is the single biggest cause of severe adult dis- ability in the UK [1], and affects between 178 and 317 people per 100,000 population in England each year [2]. One in four men and one in five women aged 45 and over will have a stroke during their lifetime [3] with a quarter of new strokes being in those aged under 65 [1]. Stroke therefore represents a sizeable challenge on mul- tiple levels. At the societal level, stroke is estimated to cost in the region of £2.8 billion per annum in the UK [2,4]. On a personal level, the “costs” are arguably greater; while one third of people who have a stroke fully recover, a third die, with the remaining third having to contend with residual motor and sensory abnormalities, many of whom also have associated psychological side-effects [5,6]. More specifically, stroke can result in impairments such as the loss of muscle strength [7-13], and dexterity and proprioception [14,15]. Additionally, postural steadiness (the ability to maintain balance dur- ing dynamic and static activities) is often reduced [16, 17]. As balance is an integral part of everyday function- ing, alterations in this modality can have a detrimental effect on many aspects of a person’s life including their ability to walk [18,19]. Currently rehabilitation post stroke is predominantly limited to the acute and sub-acute stages with limited access beyond 6 months [20,21]. However evidence sug- gests that functional recovery can continue beyond six months, with the recovery plateau post stroke being strongly debated in the literature [22-24]. Yet how on- going rehabilitation can be achieved presents a challenge given that current access to community-based therapies, in particular physiotherapy, has been described by stroke survivors as being too brief and time limited to promote best recovery [25,26]. Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 41 The need to develop strategies for accessing further rehabilitation beyond the current NHS pathways is evi- dent. Delivery of health and well-being interventions by non-healthcare professionals is not without precedence and is a growing area of interest [27-29]. For example, people living with cardiovascular conditions in the com- munity are commonly referred to exercise groups run by professional fitness instructors [30]. Similarly more pro- vision for the continuing input for stroke survivors from outside the health system is being seen, and the evidence for community based exercise after stroke schemes is growing and highlighted in policy and clinical stroke guidelines for further development [20,31,32]. Action for Rehabilitation from Neurological Injury (ARNI) is a UK based charity founded in 2001 by a stroke survivor which aims to help bridge this gap by providing functional training for people with stroke. The service is delivered by ARNI accredited exercise in- structors (non-medical) and is focused on the achieve- ment of functionally-oriented tasks through improving strength, endurance, balance and coordination, and mo- tivation as described in the ARNI manual and a two day training programme [33]. ARNI training is a multimodal approach of which functional strength training is one component. For example, participants in the group for- mat may practice sit to stand to strengthen hip and knee extensors. Consequently, improvement in strength is ex- pected as a benefit of ARNI training. ARNI is mostly delivered on a one to one basis as opposed to a group format, although in service delivery models (e.g. Bed- fordshire and Hertfordshire), a group format has been adopted which is a decision mostly driven by financial and personnel constraints [34]. While there are numerous personal testimonies to the success of the approach for individual stroke survivors [35], to date there is no em- pirical evidence of outcomes and uncertainty remains as to the effects of this training programme. The aim of this 16 month pragmatic study was to eva- luate the effectiveness and acceptability of ARNI func- tional training programme for people with stroke using a group model for service delivery. Findings from a quali- tative evaluation relating to the acceptability of taking part in the ARNI training programme are reported else- where (Norris et al.—in press). This paper specifically reports the effectiveness of training based on data from a range of biomechanical, physical and psychosocial measures. Reported results can be used for the calcula- tion of sample size in future larger studies, and provide insight into the potential obstacles of service delivery. 2. METHODS A pragmatic mixed methods approach was used. The intervention provided was a 12 week, 1 1/2 hour weekly group based ARNI programme [33]. Training was deliv- ered by two exercise instructors to a maximum of 8 par- ticipants to ensure safety and to maximise the opportu- nity for individuals to have some 1:1 time with an in- structor (whilst the remaining people continued exercis- ing as part of the group) to address personal goals. In total, four groups completed the training programme, which is described in detail elsewhere [33]. The pro- gramme took place in a newly built leisure centre facility in West London, UK. In line with the International Classification of Func- tioning, Disability, and Health (ICF) levels, impairment was assessed by biomechanical tests of strength and postural steadiness and activity was measured through the use of the Berg Balance Scale (BBS) and 10 m walk. The validated Patient Reported Outcome Measure, SIPSO, was used as a measure of both social and physi- cal impact acting as an indicator of participation [36]. 2.1. Participants All participants who volunteered to take part in the study were community dwelling stroke survivors who had finished formal physical rehabilitation. Participants in the study were screened and referred by a physio- therapist and all received GP clearance before taking part in the training. In total 30 stroke survivors participated in the intervention. Thirteen participants (4 F, 9 M, mean age 53 years; range 19 - 80 years; average time post stroke 20 months; range 4 - 154 months) volunteered to Table 1. Anthropometric data of participants. PARTICIPANTGender WEIGHT (N) AGE (Yr) SIDE TIME SINCE STROKE (months) 1 M 684 46 R 12 2 M 733 32 R 154 3 F 752 19 R 7 4 M 732 63 L 11 5 F 730 58 L 7 6 F 585 52 R 8 7 M 817 33 R 17 8 M 1040 48 L 13 9 M 877 76 R 4 10 F 612 49 R 12 11 M 890 80 R 6 12 M 528 56 L 5 13 M 831 76 R 4 Note. Side refers to the paretic side: R = right, L = left. Copyright © 2013 SciRes. OPEN ACCESS 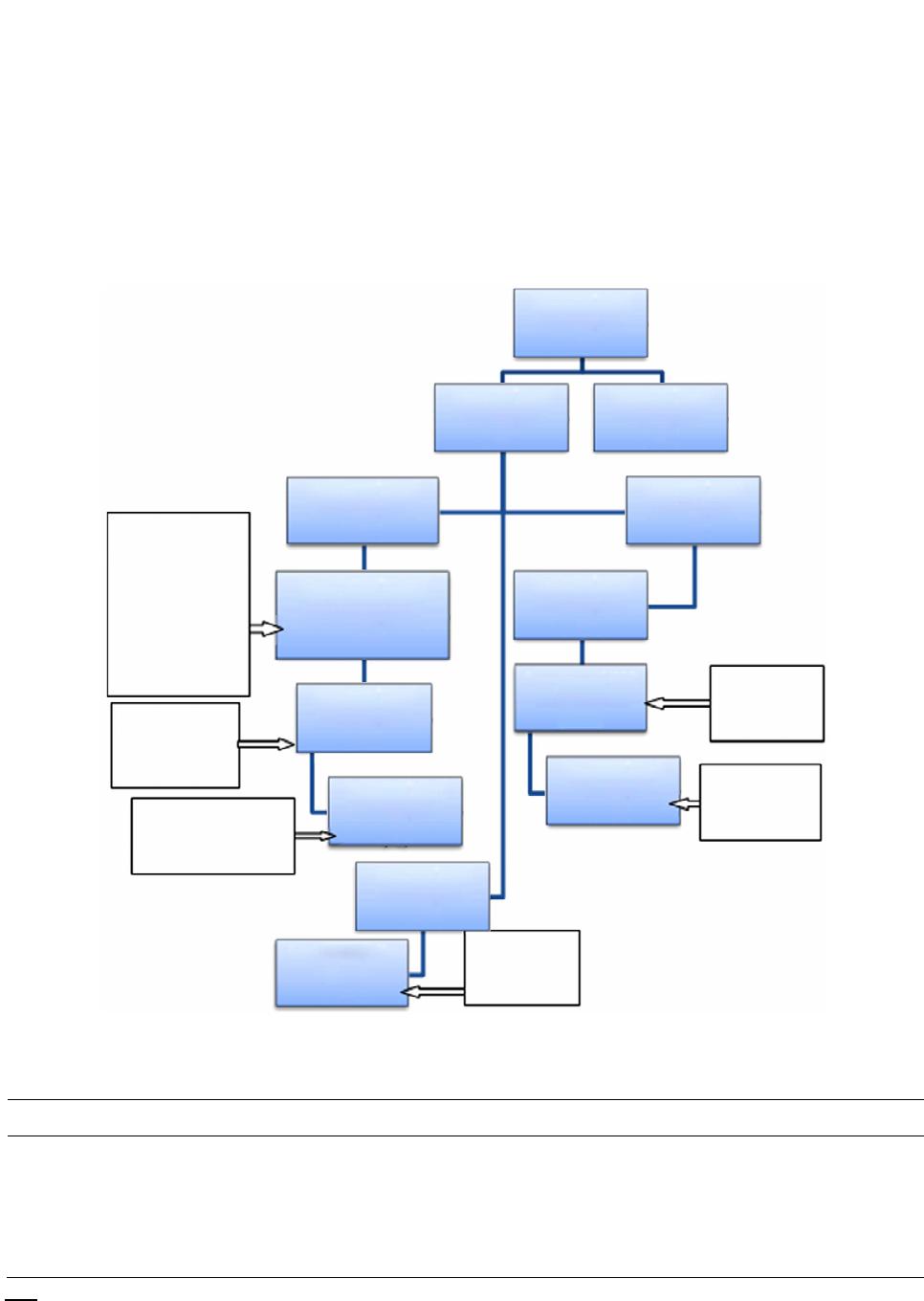 C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 Copyright © 2013 SciRes. 42 complete various aspects of the impairment and activity testing, which had an inclusion criteria of independent standing balance for a minimum of 2 minutes and the cognitive ability to follow simple instructions required for the strength tests (Table 1). The SIPSO which was open to all participants was completed by 23 participants who equally had a diverse profile in terms of age and time since stroke. Figure 1 presents a flow chart of assessments completed and num- ber of participants at each stage whose data contributed to the results and analyses including withdrawals and reasons for non-completion. Demographics of partici- pants who took part in the ARNI training are presented in Table 2. Ethics approval for the conduction of the study was obtained from the Brunel University School of Sport and Education Research Ethics Committee, and all participants provided informed consent before taking part in the study. n = 4 did not respond to mailout Completed clinical and lab testing post-training (n = 11) n = 7 did not respond to mailout n = 3 did not meet testing requirement for clinical testing n = 4 did not meet testing requirement for lab based measures. n = 2 because of medical condition, n = 1 refused n = 2 unable to attend, n = 1 ecause of illness Completed focus group (n = 22) n = 2 unable to attend on date Completed SIPSO post-training (n = 19) Completed clinical and lab testing at 3 months follow up (n = 8) Volunteered for focus group (n = 24) Completed SIPSO at 3 months follow up (n = 12) Completed SIPSO post-training (n = 23) Completed clinical testing pre-training (n = 14) Lab based measures (n = 13) Volunteered for physical testing (n = 17) Volunteered for research arm (n = 25) Accepted onto training programme (n = 30) Volunteered for SIPSO (n = 23) Did not volunteer for research arm (n = 5) Figure 1. Flowchart of assessments completed and participation at each stage of the study. Table 2. Demographic data of participants in the ARNI training. Characteristic Totals/Average (range) Physical testing SIPSO Focus Groups Participants 25 14 23 22 Gender 9 F, 16 M 4 F, 10 M 9 F, 13 M 8 F, 13 M Age (years) 61.6 (19 - 84) 61.6 (19 - 82) 61.6 (19 - 84) 61.6 (19 - 84) Time since stroke (years) 3.18 (0.5 - 26) 1.71 (0.5 - 13) 2.23 (0.5 - 26) 1.67 (0.5 - 13) OPEN ACCESS No.te Physical testing refers to both clinical and lab based measures.  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 43 2.2. Procedure All measures were taken at baseline, post intervention and at 3 month follow-up and were repeated in the same order. They were conducted by the same researchers to maintain consistency. For the tests of postural stability, the participant was asked to stand comfortably on a Kistler piezoelectric force platform (type 9281B11; Kistler, Switzerland); arms by their side, while maintaining their gaze on a (black circle) target mounted on a wall in front of them at three meters distance, and keep this position for 30 sec- onds. No instruction with respect to the foot placement was provided. Coordinates of the centre of pressure (COP) in the anteroposterior (AP) and mediolateral (ML) directions recorded during the last 20 seconds of quiet standing were used to calculate eight measures of pos- tural steadiness (total, AP, and ML excursions of the COP; total, AP, and ML velocity of the COP; AP and ML range of COP excursion) according to Prieto et al. [37]. A maximum of three successful trials were col- lected based on the participant’s ability to maintain their balance or follow the instructions for the duration of the trial and the average of the outcome measures were used in the analysis. The participant sat down between trials for thirty seconds to avoid fatigue. It was decided to test the strength of the knee flexor and extensor muscle groups as an indicator of strength in the lower limb since a significant correlation amongst strength measured from different muscle groups of the lower limb after stroke has been reported [38,39]. A System 3 Biodex Isokinetic Dynamometry system (Bio- dex Medical Systems, New York, USA) was used for the assessment of strength of both the non-paretic (NP) and paretic (P) sides. The non-paretic limb was tested first. The participants were asked to produce maximum iso- metric knee extension or flexion torques while in a seated position (back rest angle at 85 degrees) at two different joint angles equal to 90% and 80% of the available range of motion between 90 degree of knee flexion and full extension. Using this procedure, torques were measured at angles closer to full knee extension. The order of angle at which strength was tested was al- ternated between the participants. Verbal encouragement was provided during the trials. At each joint angle tested, the participant was asked to produce a maximum extension torque for five seconds followed by a maximum flexion torque for five seconds. There was a ten second rest interval between each exten- sion-flexion torque pair. Three pairs of extension-flexion torques were produced at each joint angle. There was 120 seconds rest interval between the sets of exten- sion-flexion torque production at the two angles. Maxi- mum torques recorded during the last two pairs of torque production were normalised to the body weight [40,41] and their average was used in the final analysis. Some participants were unable to produce torques above the value used by the system for gravity correction. For these individuals/sessions the gravity correction value deter- mined by the system at the time of testing was used as the maximum torque to prevent missing values for the analysis. Accordingly, maximum torque could have been overestimated in such circumstances. Dynamometry and force platform data were sampled at 100 Hz. The Berg Balance [42] was carried out in accordance with published guidelines. The 10 m walk was repeated three times with a one metre lead in and out distance. The average of the three trials was calculated and the participant was given the option to rest between trials to minimise the impact of fatigue. The SIPSO was com- pleted independently by the participants. 2.3. Data Analysis Clinical data were analysed in SPSS (SPSS Inc.; ver. 18.02) using a variety of tests as appropriate including t-test, ANOVA, related samples Friedman’s Two-way analysis of variance or a one tail sign test. For the bio- mechanical data, conventional paired t-test, one-way ANOVA, and MANOVA with repeated measures (side, joint angle, and testing session) was used to test the ef- fect of training on balance and strength data between the NP and P sides at baseline and post-training, or across the three (baseline and post-training and follow up) testing sessions at the two joint angles. The level of sig- nificance for all tests was selected at 0.05 (α = 0.05). An intention to treat analysis was conducted. Attendance rate was good averaging 74% - 90% across the four groups. 3. RESULTS Different number of participants took part in different tests. Figure 1 illustrates a flow chart of the study where reasons for drop outs are also included. 3.1. Measures of Impairment Overall, postural stability performance of the partici- pants did not show any statistically significant differ- ences across the three sessions, or between the baseline and post-training sessions (all p values > 0.05). Results for the postural steadiness are illustrated in Figures 2 and 3. For the extension torque at the baseline and post- training sessions, the effects of side and joint angle were significant. As expected, the non-paretic (NP) legs were significantly stronger than the paretic (P) legs (F[1,10] = 19.98; p = 0.001), and the torques produced at the rela- tively more extended joint angle were smaller (F[1,10] = 44.61; p = 0.0001). For the flexion torque, only the effect of side was significant where NP legs produced higher flexion torque values compared to the P legs (F[1,10] = Copyright © 2013 SciRes. OPEN ACCESS 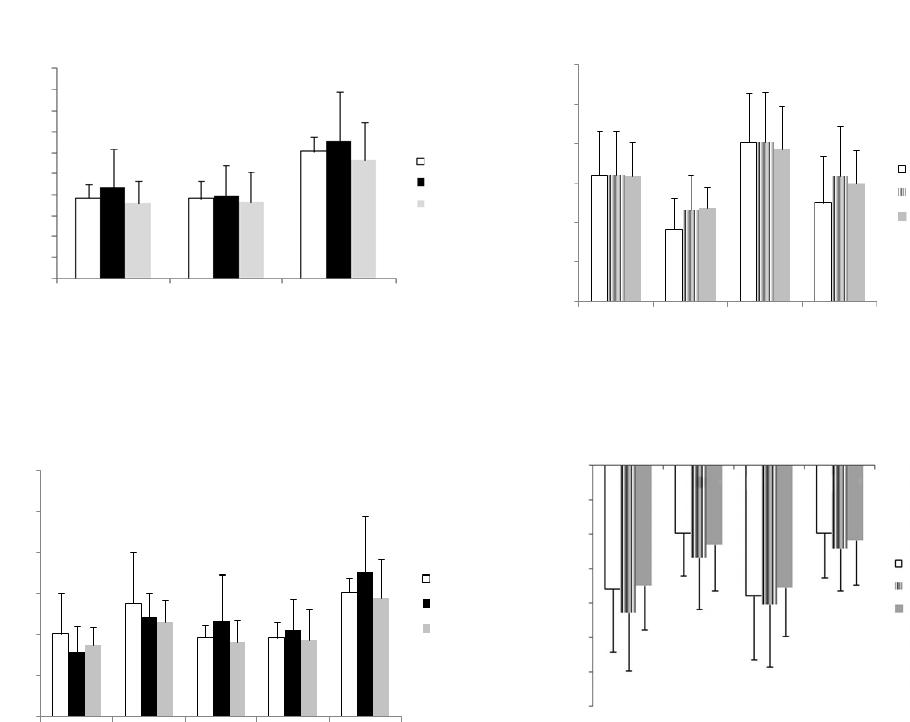 C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 44 PRE POST FO L MLEX APEX TOTEX 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 COP Excursion (m) Figure 2. MLEX = excursion of the centre of pressure (COP) in the mediolateral (side-to-side) direction; APEX = excursion of the COP in the anteroposterior (forward-backward) direction; TOTEX = total excursion of the COP. Error bars are group standard deviations. PRE, POST, and FOL refer to the pre-, post- and follow-up testing sessions. 0.06 0.05 0.04 0.03 0.02 0.01 0 RML RAP MVEL ML MVEL AP MVEL PRE POST FO L Figure 3. R ML = range of COP excursion in the mediolateral direction (m); R AP = range of COP excursion in the antero- posterior direction (m); M VEL ML = mean velocity of the COP in the ML direction (m/s); M VEL AP = mean velocity of the COP in the AP direction (m/s); M VEL = mean velocity of the COP (m/s); Error bars are group standard deviations. PRE, POST, and FOL refer to the pre-, post- and follow-up testing sessions. 9.26; p = 0.012). Similar results were found when the extension torques results were analysed across three ses- sions (F[1,7] = 24.15; p = 0.002 for the effect of side, and (F[1,7] = 54.60; p = 0.0001 for the effect of joint angle), but the difference between the NP and P sides for the flexion torques became non-significant (Figures 4 and 5). 3.2. Measures of Activity Results for the measures of activity are shown in Ta- ble 3. Balance as measured by the BBS indicated a sig- nificant improvement across the testing sessions (F[2,11] = 10.63; p < 0.002) and all participants improved their scores. The average change from baseline to follow-up sessions was 6 points. This exceeded the minimal de- tectable change (MDC) for chronic stroke (defined as >6 months post stroke) which was reported as 2.5 points on the BBS [43]. It should be further noted that there was a 0.120 0.100 0.080 0.060 0.040 0.020 0.000 Extension (normalised) torque PRE POST FOLLO W PEXT90 PEXT90 NPEXT80 PEXT80 Figure 4. NP = non-paretic; P = paretic; Ext = extension torque; 90 and 80 refer to the testing joint position as percentage of available knee joint range of motion. 90 is a relatively more extended (straight) joint angle. Torque values are normalised to the body weight. Error bars are group standard deviations. PRE POST FOLLOW 0.000 −0.020 −0.040 −0.060 −0.080 −0.100 −0.120 −0.140 Flexion (normalised) torque PFLEX90 PFLEX90 NPFLEX80 PFLEX80 Figure 5. NP = non-paretic; P = paretic; FLEX = flexion torque; 90 and 80 refer to the testing joint position as percentage of available knee joint range of motion. 90 is a relatively more ex- tended (straight) joint angle. Torque values are normalised to the body weight. Error bars are group standard deviations. ceiling effect, for this measure for 2 participants at fol- low-up. As a consequence it was possible that the results did not fully demonstrate the improvement achieved. The 10 m walk test also indicated an improvement. Nine of the eleven tested improved their walking speed post intervention and there was a general trend for im- provement from baseline to the follow-up testing ses- sions. However, these changes did not reach significance level. The improvement from baseline to post-training session was significant (p = 0.03) on a 1-tail sign test. These pairwise results supported an overall trend towards improvement. MDC for chronic stroke is documented as a 16% change [44] and the baseline to follow up changes achieved this illustrating a 37% improvement in walking speed. The minimally clinically important difference (MCID) is reported in the subacute population as 0.16 m/s [45]. This study indicated a MCID change of 0.15 m/s in this chronic population. 3.3. Measure of Participation The SIPSO scores indicated a borderline significant Copyright © 2013 SciRes. OPEN ACCESS 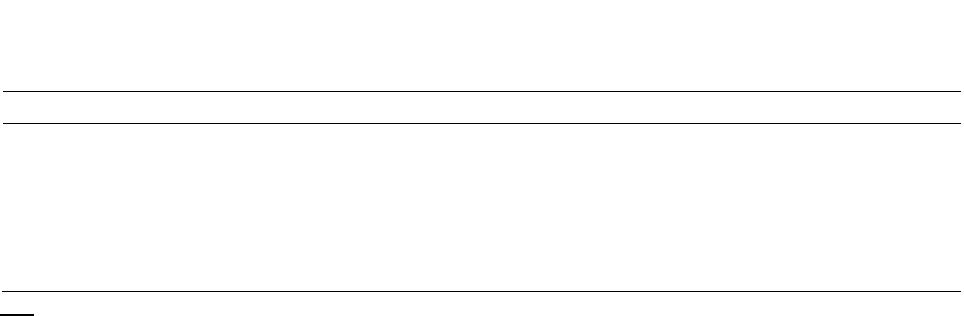 C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 Copyright © 2013 SciRes. OPEN ACCESS 45 Table 3. Mean (SD) of outcome measures at baseline (T0), post intervention (T1), and 3 months follow-up (T2). T0 T1 T2 Sig. BBS2 44.09 (11.90) 49.36 (11.13) 50.25 (8.78) F(2,11) = 10.63; p < 0.0022 10 m walk 25.08 (24.15) 18.85 (16.67) 18.06 (13.55) F(2,11) = 1.69 ns SIPSO total1 23.32 (6.45) 26.84 (6.81) 28.83 (6.10) χ2(2) = 6.26; p = 0.0441 SIPSO section a (physical)2 11.84 (4.72) 13.84 (4.23) 14.17 (4.86) F(2,22) = 1.72 ns SIPSO section b (social)2 11.47 (3.41) 13 (3.96) 13.75 (3.02) F(2,22) = 1.78 ns Note. BBS—increase score indicate improvement, 10 m walk—decrease score indicates improvement, SIPSO—increase score indicates improvement. 1Analysed with Friedman’s two way analysis of variance. 2Analysed with ANOVA. improvement overall (p = 0.044). However, when con- sidered independently, the changes in physical and social subsections were non-significant (Physical: F[2,22] = 1.72, ns; Social: F[2,22] = 1.78, ns). 4. DISCUSSION The purpose of the study was to evaluate the effec- tiveness of a twelve-week ARNI functional training pro- gramme delivered in a group format on measures of im- pairment, activity, and participation in stroke survivors. While no significant improvement in the strength of the lower limb and COP-based measures of postural steadi- ness were noted, an improvement in functional balance activity and a trend toward walking faster post interven- tion were seen. The SIPSO showed a significant overall improvement in the level of participation, but the physi- cal and social subsections did not alter significantly. 4.1. Effect of ARNI Functional Training on Strength 4.1.1. Knee Extensor Muscles Group In contrast to the results of the present study, im- provement in muscle strength with functional training in stroke patients has been reported before [46-48]. How- ever, in these studies examination of the isometric mus- cle strength was mostly conducted at angles which fa- voured torque production, i.e. at longer lengths of the muscle. In the present study the extensor muscles group were tested at short lengths at angles similar to those adopted during the stance phase of gait [49,50]. Inas- much as extension torque was not tested at long muscle lengths, it was not possible to rule out if improvement in muscle strength had occurred at long lengths. Selective weakness of the hemiparetic muscles at shorter muscles lengths have been reported elsewhere in the literature, with this impairment attributed to the reduced rate of motor unit firing, differentially reduced excitability of the motor cortex, and changes in the operating range of the extensor muscles amongst others [51-54]. Present findings support the relative weakness of the knee ex- tensor muscles group in the P compared to the NP side, and suggest that the employed functional training regime did not affect the underlying impaired mechanisms for the selective muscle weakness at shorter lengths in twelve weeks. Lack of improvement in muscle strength with training in the present study could also be an artefact due to the methodology employed for the analysis of the dyna- mometry results. As stated before, some participants were not capable of producing torque above the values used by the dynamometry system for gravity correction at the initial assessment, but they produced recordable torque in the subsequent sessions (Figure 6). For these participants, we perhaps overestimated the maximal torque by using the individualised gravity correction value in the pre-testing session for the analysis. There- fore increase in muscle strength after intervention, rep- resented by small recordable torque, might have not reached to the level of significance. 4.1.2. Knee Flexor Muscles Group For the flexor group, the present results are partially consistent with those of Koo et al. [54] who employed a range of different joint angles to evaluate the strength of the elbow flexor muscles in a group of hemiparetic and control participants. Koo et al. [54] found no difference in the flexion torque between the two groups, but re- ported that at the shorter lengths of the muscle, i.e. at the more flexed positions, flexor muscles in the hemiparetic group were relatively weaker. In the current study, strength in the Hamstrings group was only assessed at the longer lengths. Therefore, the results are not against the notion of joint position dependency of muscular weakness in stroke survivors as discussed by Koo et al. and others (indicated above), but do not fully support the similarity of the knee flexion strength between the P and NP since a significant difference between the P and NP flexion torque was observed when the results of the pre- and post-testing sessions were compared. 4.1.3. Relationship between Impairment and Activity Existence of a correlation between strength and activ- 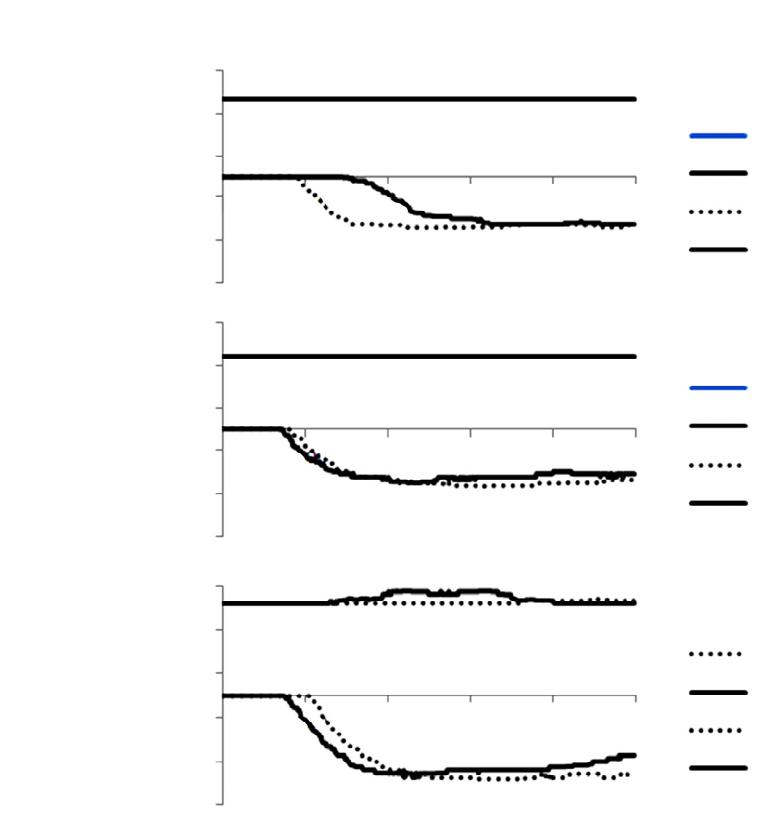 C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 46 0 1000 2000 3000 4000 5000 25 15 5 −5 −15 −25 Torque (Nm) Time (msec) Ext - T2 Ext - T3 Flex - T2 Flex - T3 Ext - T2 Ext - T3 Flex - T2 Flex - T3 Ext - T2 Ext - T3 Flex - T2 Flex - T3 0 1000 2000 3000 4000 5000 Time (msec) 0 1000 2000 3000 4000 5000 Time (msec) 25 15 5 −5 −15 −25 Torque (Nm) 25 15 5 −5 −15 −25 Torque (Nm) Figure 6. Extension and flexion torques produced by a participant at the 90% of the available range of motion in the pre- (upper panel) and post-training (middle panel), and follow-up (lower panel) sessions. Ext = extension torque; Flex = flexion torque; T2 and T3 refer to the second and third attempt from which maximum torques were calculated. Choice of sign for torques is arbitrary. The participant was incapable of producing exten- sion torque at the tested angle in both pre- and post-training sessions (hence the over- lapped flat lines), but produced recordable torques in the follow-up session during the third attempt. ity (function) after stroke is a matter of controversy [11, 55,56]. In the present study, a significant improvement in the BBS and a trend toward improvement in walking speed demonstrated partial improvement in the activity level which was not associated with improvement in strength. Klein et al. [12] also reported that the preferred gait speed was not limited by the weakness in stroke pa- tients. There are some explanations for the apparent lack of association between measures of function and strength. It has been suggested that measures of strength similar to that employed in the present study are context specific and whether a measure of static strength (e.g. maximum isometric torque) can be representative of strength during dynamic tasks (such as walking) is not clear [57]. Other measures of strength (e.g. isokinetic peak torque and work of the knee extensor muscles) were significantly correlated to the gait velocity (particularly at faster speeds) in chronic stroke survivors [72,73]. Differences in the methodology (with isokinetic assessment of strength resembling more to the strength requirement during dynamic tasks), and recruitment of a group of more homogenous and less impaired participants in these studies might explain differences in the findings. Studies which reported a significant correlation be- tween the maximum isometric strength of the knee ex- tensor and flexor muscles and walking speed and endur- ance in stroke population only reported low to medium values for the relationship between the two variables Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 47 [58-60]. It has also been argued that motor behaviour of patient populations follows a non-linear trend where for some individuals, small (insignificant) alteration in one measure (e.g. strength) might result in a significant change in the behaviour (e.g. ability to stand or walk faster), whilst for others, it only prevents deterioration of the current condition [61]. This is similar to the sugges- tion made by Bohannon [62] who argued that a strength threshold related to the functional demand of a task should be reached for the successful completion of the task, beyond which increase in strength would not have any significant further influence on the efficiency of the task performance. In such circumstances improvement of strength might improve the speed of the task completion or act as a reserve against deterioration of the perform- ance. 4.1.4. Relationship between Clinical and Biomechanical Measures of Balance The significant improvement in balance as demon- strated by the BBS was in line with improvement re- ported in similar studies of exercise groups after stroke [63,64]. Of particular interest, however, was the im- provement across all participants irrespective of their age and time post stroke. Such improvement was not associ- ated with alteration in the COP-based measures of pos- tural stability, or increased strength in the P leg [74]. Participants were included in the present study if they could maintain an unsupported stance for two minutes, and hence would score maximum points in the “standing unsupported” item of the BBS. Therefore, any changes in the other aspects of balance abilities assessed by the BBS could result in a lack of association between the results of the two tests. Only moderate correlation between the BBS and COP-based measures of balance has been re- ported before and authors attributed the findings to the different aspects of the balance abilities represented by these tests [65,66]. ARNI training included standing up from the floor and transfer of weight alternatively to the stronger and weaker sides of the body during functional tasks. It is therefore possible that the underlying mecha- nisms for the more dynamic balance activities benefited further from the training. 4.2. ARNI Functional Training May Improve Quality of Life In view of these positive results in activity it is per- haps surprising that the SIPSO did not indicate more extensive changes in quality of life, although the trend was for some improvement. Previous work has ques- tioned the direct link between physical capacity and quality of life [67] and the present results suggest that this relationship is certainly not linear. The SIPSO con- siders a variety of factors including both community ambulation and communication with friendship networks. Three participants had communication problems which naturally were not addressed in the ARNI training. Walking speed is a commonly used indicator of activity potential and therefore can have an important difference on the stroke survivors’ ability to interact with their sur- roundings. However, while walking speed and balance are associated with community walking, other factors such as confidence and self-efficacy are equally impor- tant and were not measured in this study [68]. It is argued that results such as those reported in this paper reinforce the call to extend rehabilitation pathways beyond the initial acute and sub-acute periods and ques- tion the effectiveness of the current environment for stroke survivors to maximise their activity and functional potential [69]. They further highlight a need for an ex- tended rehabilitation pathway supported by community resources. Previous research has involved fitness in- structors in providing exercise to stroke survivors with some positive results [47,64]. However, research also indicates that uptake and continuation is limited by ac- cess to specialised gym facilities and self-consciousness created as a result of exercising with able bodied people [70,71]. This study was run in a health facility but re- quired no specialist gym equipment, and while it was run in a group format, the results would indicate that suffi- cient training effect was achieved for at least the clinical measures to change. 4.3. Limitations A sample of convenience was recruited for this eva- luative study and there were no control participants. The participating group was comprised of a broad range of stroke survivors with different levels of motor impair- ment who received training in a group format which rep- resented a real life situation. The standard model of the ARNI programme is on a 1:1 basis with resultant finan- cial implications. The present study only supports the effectiveness of the ARNI training in a group format as a form of service delivery for stroke survivors, where spe- cific trainings are individualised according to the abilities of the trainee [75]. Instructors who delivered the training were blinded to recruitment and hence the participants in the present study were not treated differently from the remaining of the training group. The research group was independent from ARNI. 5. CONCLUSION In summary, twelve weeks of ARNI functional train- ing positively affected activity and participation levels in a group of stroke survivors. Such improvements were however not associated with improvement at an impair- Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 48 ment level. No adverse effect was observed as a result of participating in the training or assessment sessions, and hence, the training can be undertaken as an adjunct to rehabilitation plans or as part of a longer term personal plan for health and wellbeing. 6. ACKNOWLEDGEMENTS Authors would like to thank London Borough of Hillingdon for fi- nancial support, Jackie O’Dowd for recruitment of the participants of this project. REFERENCES [1] National Audit Office (2010) Progress in improving stroke care: A good practice guide. National Audit Office. [2] Townsend, N., Wickramasinghe, K., Bhatnagar, P., Smolina, K., Nichols, M., Leal, J., Luengo-Fernandez, R. and Rayner, M (2012). Coronary heart disease statistics. British Heart Foundation, London. [3] Wolfe, C.D. (2000) The impact of stroke. British Medical Bulletin, 56, 275-286. http://dx.doi.org/10.1258/0007142001903120 [4] Saka, O., McGuire, A. and Wolfe, C. (2009) Cost of stroke in the United Kingdom. Age Ageing, 38, 27-32. http://dx.doi.org/10.1093/ageing/afn281 [5] Hackett, M.L., Yapa, C., Parag, V. and Anderson, C.S. (2005) Frequency of depression after stroke: A systematic review of observational studies. Stroke, 36, 1330-1340. http://dx.doi.org/10.1161/01.STR.0000165928.19135.35 [6] Sandercock, P., Dennis, M., Warlow, C., Van Gijn, J., Hankey, G., Bamford, J. and Warlow, J. (2001) Stroke: A practical guide to management. Wiley, Hoboken. [7] Ada, L., Dorsch, S. and Canning, C.G. (2006) Strength- ening interventions increase strength and improve activity after stroke: A systematic review: 1. The Australian Jour- nal of Physiotherapy, 52, 241-248. http://dx.doi.org/10.1016/S0004-9514(06)70003-4 [8] Patten, C., Lexell, J. and Brown, H.E. (2004) Weakness and strength training in persons with poststroke hemiple- gia: Rationale, method, and efficacy. Journal of Reha- bilitation Research and Development, 41, 293-312. http://dx.doi.org/10.1682/JRRD.2004.03.0293 [9] Prado-Medeiros, C.L., Silva, M.P., Lessi, G.C., Alves, M.Z., Tannus, A., Lindquist, A.R. and Salvini, T.F. (2012) Muscle atrophy and functional deficits of knee extensors and flexors in people with chronic stroke. Physical Ther- apy, 92, 429-439. http://dx.doi.org/10.2522/ptj.20090127 [10] Hafer-Macko, C.E., Ryan, A.S., Ivey, F.M. and Macko, R.F. (2008) Skeletal muscle changes after hemiparetic stroke and potential beneficial effects of exercise inter- vention strategies. Journal of Rehabilitation Research and Development, 45, 261. http://dx.doi.org/10.1682/JRRD.2007.02.0040 [11] Horstman, A.M., Beltman, M.J., Gerrits, K.H., Koppe, P., Janssen, T.W., Elich, P. and de Haan, A. (2008) Intrinsic muscle strength and voluntary activation of both lower limbs and functional performance after stroke. Clinical Physiology and Functional Imaging, 28, 251-261. http://dx.doi.org/10.1111/j.1475-097X.2008.00802.x [12] Klein, C.S., Brooks, D., Richardson, D., McIlroy, W.E. and Bayley, M.T. (2010) Voluntary activation failure contributes more to plantar flexor weakness than antago- nist coactivation and muscle atrophy in chronic stroke survivors. Journal of Applied Physiology, 109, 1337- 1346. http://dx.doi.org/10.1152/japplphysiol.00804.2009 [13] Miller, M., Flansbjer, U. and Lexell, J. (2009) Voluntary activation of the knee extensors in chronic poststroke sub- jects. American Journal of Physical Medicine & Reha- bilitation, 88, 286-291. http://dx.doi.org/10.1097/PHM.0b013e318198b569 [14] Bleyenheuft, Y. and Thonnard, J.L. (2011) Tactile spatial resolution in unilateral brain lesions and its correlation with digital dexterity. Journal of Rehabilitation Medicine, 43, 251-256. http://dx.doi.org/10.2340/16501977-0651 [15] Kiyama, R., Fukudome, K., Hiyoshi, T., Umemoto, A., Yoshimoto, Y. and Maeda, T. (2011) The loss of dexter- ity in the bilateral lower extremities in patients with stroke. Journal of Applied Biomechanics, 27, 122-129. [16] Lubetzky-Vilnai, A. and Kartin, D. (2010) The effect of balance training on balance performance in individuals poststroke: A systematic review. Journal of Neurological Physical Therapy, 34, 127-137. http://dx.doi.org/10.1097/NPT.0b013e3181ef764d [17] Marigold, D.S. and Eng, J.J. (2006) Altered timing of postural reflexes contributes to falling in persons with chronic stroke. Experimental Brain Research, 171, 459- 468. http://dx.doi.org/10.1007/s00221-005-0293-6 [18] Esquenazi, A., Ofluoglu, D., Hirai, B. and Kim, S. (2009) The effect of an ankle-foot orthosis on temporal spatial parameters and asymmetry of gait in hemiparetic patients. PM & R, 1, 1014-1018. http://dx.doi.org/10.1016/j.pmrj.2009.09.012 [19] Patterson, K.K., Parafianowicz, I., Danells, C.J., Closson, V., Verrier, M.C., Staines, W.R., Black, S.E. and McIlroy, W.E. (2008) Gait asymmetry in community-ambulating stroke survivors. Archives of Physical Medicine and Re- habilitation, 89, 304-310. http://dx.doi.org/10.1016/j.apmr.2007.08.142 [20] Department of Health (2007) National stroke strategy. Department of Health, London. [21] The Stroke Association (2010) Moving on: A vision for community based physiotherapy after stroke in England. [22] Verheyden, G. and Ashburn, A. (2011) Stroke. In: Stokes, M. and Stack, E., Eds., Physical Management for Neuro- logical Conditions, 3rd Edition, Elsevier Churchill Liv- ingstone, London, 9-28. [23] Hendricks, H.T., van Limbeek, J., Geurts, A.C. and Zwarts, M.J. (2002) Motor recovery after stroke: A sys- tematic review of the literature. Archives of Physical Medicine and Rehabilitation, 83, 1629-1637. http://dx.doi.org/10.1053/apmr.2002.35473 [24] Demain, S., Wiles, R., Roberts, L. and McPherson, K. (2006) Recovery plateau following stroke: Fact or fiction? Disability and Rehabilitation, 28, 815-821. Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 49 http://dx.doi.org/10.1080/09638280500534796 [25] The Stroke Association (2012) Struggling to recover. The Stroke Association, London. [26] Winchcombe, M. (2012) A life more ordinary—Findings from the long-term neurological conditions research ini- tiative. [27] Horgan, J., Bethell, H., Carson, P., Davidson, C., Julian, D., Mayou, R.A. and Nagle, R. (1992) Working party re- port on cardiac rehabilitation. British Heart Journal, 67, 412-418. http://dx.doi.org/10.1136/hrt.67.5.412 [28] Morgan, O. (2005) Approaches to increase physical activ- ity: Reviewing the evidence for exercise-referral schemes. Public Health, 119, 361-370. http://dx.doi.org/10.1016/j.puhe.2004.06.008 [29] Sharma, H., Bulley, C. and van Wijck, F.M.J. (2011) Experiences of an exercise referral scheme from the per- spective of people with chronic stroke: A qualitative study. Physiotherapy, 98, 336-343. http://dx.doi.org/10.1016/j.physio.2011.05.004 [30] Bethell, H., Lewin, R. and Dalal, H. (2009) Cardiac reha- bilition in the United Kingdom. Heart, 95, 271-275. http://dx.doi.org/10.1136/hrt.2007.134338 [31] Brazzelli, M., Saunders, D.H., Greig, C.A. and Mead, G.E. (2012) Physical fitness training for patients with stroke: Updated review. Stroke, 43, e39-e40. http://dx.doi.org/10.1161/STROKEAHA.111.647008 [32] Intercollegiate Stroke Working Party (2012) Maintaining standards—The national clinical guideline for stroke. 4th Edition, London. [33] Balchin, T. (2011) The successful stroke survivor. Bag- wyn, Surrey. [34] Luton stroke service on the world stage (2012). http://www.luton.gov.uk/news/Pages/Luton-stroke-servic e-on-the-world-stage.aspx [35] Stroke survivors information page. http://www.arni.uk.com/members-page.html#testimonials [36] Trigg, R. and Wood, V.A. (2000) The subjective index of physical and social outcome [SIPSO]: A new measure for use with stroke patients. Clinical Rehabilitation, 14, 288- 299. http://dx.doi.org/10.1191/026921500678119607 [37] Prieto, T.E., Myklebust, J.B., Hoffmann, R.G., Lovett, E.G. and Myklebust, B.M. (1996) Measures of postural steadiness: Differences between healthy young and eld- erly adults. IEEE Transactions on Biomedical Engineer- ing, 43, 956-966. http://dx.doi.org/10.1109/10.532130 [38] Bohannon, R.W. and Andrews, A.W. (1998) Relation- ships between impairments in strength of limb muscle ac- tions following stroke. Perceptual Motor Skills, 87, 1327- 1330. http://dx.doi.org/10.2466/pms.1998.87.3f.1327 [39] Bohannon, R.W. (2008) Is it legitimate to characterize muscle strength using a limited number of measures? Journal of Strength and Conditioning Research, 22, 166- 173. http://dx.doi.org/10.1519/JSC.0b013e31815f993d [40] Jaric, S. (2002) Muscle strength testing: Use of normali- sation for body size. Sports Medicine, 32, 615-631. http://dx.doi.org/10.2165/00007256-200232100-00002 [41] Jaric, S., Radosavljevic-Jaric, S. and Johansson, H. (2002) Muscle force and muscle torque in humans require dif- ferent methods when adjusting for differences in body size. European Journal of Applied Physiology, 87, 304- 307. http://dx.doi.org/10.1007/s00421-002-0638-9 [42] Berg, K.O., Wood-Dauphinee, S.L., Williams, J.T. and Gayton, D. (1989) Measuring balance in the elderly: Pre- liminary development of an instrument. Physiotherapy Canada, 41, 304-311. http://dx.doi.org/10.3138/ptc.41.6.304 [43] Liston, R.A. and Brouwer, B.J. (1996) Reliability and validity of measures obtained from stroke patients using the balance master. Archives of Physical Medicine and Rehabilitation, 77, 425-430. http://dx.doi.org/10.1016/S0003-9993(96)90028-3 [44] Flansbjer, U., Holmbäck, A.M., Downham, D., Lexell, J. and Sektion, I.V. (2005) What change in isokinetic knee muscle strength can be detected in men and women with hemiparesis after stroke? Clinical Rehabilitation, 19, 514- 522. http://dx.doi.org/10.1191/0269215505cr854oa [45] Tilson, J., Sullivan, K., Cen, S., et al. (2010) Meaningful gait speed improvement during the first 60 days post stroke: Minimal clinically important difference. Physical Therapy, 90, 196-208. http://dx.doi.org/10.2522/ptj.20090079 [46] Bale, M. and Strand, L.I. (2008) Does functional strength training of the leg in subacute stroke improve physical performance? A pilot randomized controlled trial. Clini- cal Rehabilitation, 22, 911-921. http://dx.doi.org/10.1177/0269215508090092 [47] Cramp, M.C., Greenwood, R.J., Gill, M., Lehmann, A., Rothwell, J.C. and Scott, O.M. (2010) Effectiveness of a community-based low intensity exercise programme for ambulatory stroke survivors. Disability and Rehabilita- tion, 32, 239-247. http://dx.doi.org/10.3109/09638280903095916 [48] Yang, Y.R., Wang, R.Y., Lin, K.H., Chu, M.Y. and Chan, R.C. (2006) Task-oriented progressive resistance strength training improves muscle strength and functional per- formance in individuals with stroke. Clinical Rehabilita- tion, 20, 860-870. [49] Chen, C., Chen, H., Tang, S.F., Wu, C., Cheng, P. and Hong, W. (2003) Gait performance with compensatory adaptations in stroke patients with different degrees of motor recovery. American Journal of Physical Medicine & Rehabilitation, 82, 925-935. http://dx.doi.org/10.1097/01.PHM.0000098040.13355.B5 [50] Milovanović, I. and Popović, D.B. (2012) Principal com- ponent analysis of gait kinematics data in acute and chro- nic stroke patients. Computational and Mathematical Me- thods in Medicine, 2012, Article ID: 649743. http://dx.doi.org/10.1155/2012/649743 [51] Ada, L., Canning, C. and Dwyer, T. (2000) Effect of mu- scle length on strength and dexterity after stroke. Clinical Rehabilitation, 14, 55-61. http://dx.doi.org/10.1191/026921500671430626 [52] Ada, L., Canning, C.G. and Low, S.L. (2003) Stroke pa- tients have selective muscle weakness in shortened range. Brain, 126, 724-731. http://dx.doi.org/10.1093/brain/awg066 Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 50 [53] Horstman, A., Gerrits, K., Beltman, M., Janssen, T., Ko- nijnenbelt, M. and de Haan, A. (2009) Muscle function of knee extensors and flexors after stroke is selectively im- paired at shorter muscle lengths. Journal of Rehabilita- tion Medicine, 41, 317-321. http://dx.doi.org/10.2340/16501977-0331 [54] Koo, T.K., Mak, A.F., Hung, L.K. and Dewald, J.P. (2003) Joint position dependence of weakness during maximum isometric voluntary contractions in subjects with hemi-paresis. Archives of Physical Medicine and Rehabilitation, 84, 1380-1386. http://dx.doi.org/10.2340/16501977-0331 [55] Gerrits, K.H., Beltman, M.J., Koppe, P.A., Konijnenbelt, H., Elich, P.D., de Haan, A. and Janssen, T.W. (2009) I- sometric muscle function of knee extensors and the rela- tion with functional performance in patients with stroke. Archives of Physical Medicine and Rehabilitation, 90, 480-487. http://dx.doi.org/10.1016/j.apmr.2008.09.562 [56] Ng, S. (2010) Balance ability, not muscle strength and exercise endurance, determines the performance of hemi- paretic subjects on the timed-sit-to-stand test. American Journal of Physical Medicine & Rehabilitation, 89, 497- 504. http://dx.doi.org/10.1097/PHM.0b013e3181d3e90a [57] Fleishman, E.A. (1964) What do physical fitness test measure? A review of previous research. In: Cliffs, N.J., Ed., The structure and measurement of physical fitness, Prentice-Hall, Inc., Englewood, 27-37. [58] Dorsch, S., Ada, L., Canning, C.G., Al-Zharani, M. and Dean, C. (2012) The strength of the ankle dorsiflexors has a significant contribution to walking speed in people who can walk independently after stroke: An observa- tional study. Archives of Physical Medicine and Rehab- ilitation, 93, 1072-1076. http://dx.doi.org/10.1016/j.apmr.2012.01.005 [59] Pang, M. and Eng, J. (2008) Determinants of improve- ment in walking capacity among individuals with chronic stroke following a multi-dimensional exercise program. Journal of Rehabilitation Medicine, 40, 284-290. http://dx.doi.org/10.2340/16501977-0166 [60] Severinsen, K., Jakobsen, J.K., Overgaard, K. and An- dersen, H. (2011) Normalized muscle strength, aerobic capacity, and walking performance in chronic stroke: A population-based study on the potential for endurance and resistance training. Archives of Physical Medicine and Rehabilitation, 92, 1663-1668. http://dx.doi.org/10.1016/j.apmr.2011.04.022 [61] Buchner, D.M., Beresford, S.A., Larson, E.B., LaCroix, A.Z. and Wagner, E.H. (1992) Effects of physical activity on health status in older adults. II. Intervention studies. Annual Review of Public Health, 13, 469-488. http://dx.doi.org/10.1146/annurev.pu.13.050192.002345 [62] Bohannon, R.W. (2007) Muscle strength and muscle training after stroke. Journal of Rehabilitation Medicine, 39, 14-20. http://dx.doi.org/10.2340/16501977-0018 [63] Cramp, M.C., Greenwood, R.J., Gill, M., Lehmann, A., Rothwell, J.C. and Scott, O.M. (2010) Effectiveness of a community-based low intensity exercise programme for ambulatory stroke survivors. Disability and Rehabilita- tion, 32, 239-247. http://dx.doi.org/10.3109/09638280903095916 [64] Stuart, M., Benvenuti, F., Macko, R., Taviani, A., Segenni, L., Mayer, F., Sorkin, J.D., Stanhope, S.J., Macellari, V. and Weinrich, M. (2009) Community-based adaptive physical activity program for chronic stroke: Feasibility, safety, and efficacy of the Empoli model. Neurorehabilitation Neural Repair, 23, 726-734. http://dx.doi.org/10.1177/1545968309332734 [65] Frykberg, G.E., Lindmark, B., Lanshammar, H. and Borg, J. (2007) Correlation between clinical assessment and force plate measurement of postural control after stroke. Journal of Rehabilitation Medicine, 39, 448-453. http://dx.doi.org/10.2340/16501977-0071 [66] Niam, S., Cheung, W., Sullivan, P.E., Kent, S. and Gu, X. (1999) Balance and physical impairments after stroke. Archives of Physical Medicine and Rehabilitation, 80, 1227-1233. http://dx.doi.org/10.1016/S0003-9993(99)90020-5 [67] Hill, T., Gjellesvik, T., Moen, P., Tørhaug, T., Fimland, M., Helgerud, J. and Hoff, J. (2012) Maximal strength training enhances strength and functional performance in chronic stroke survivors. American Journal of Physical Medicine & Rehabilitation, 91, 393-400. http://dx.doi.org/10.1097/PHM.0b013e31824ad5b8 [68] Schmid, A.A., Van Puymbroeck, M., Altenburger, P.A., Dierks, T.A., Miller, K.K., Damush, T.M. and Williams L.S. (2012) Balance and balance self-efficacy are associ- ated with activity and participation after stroke: A cross- sectional study in people with chronic stroke. Archives of Physical Medicine and Rehabilitation, 93, 1101-1107. http://dx.doi.org/10.1016/j.apmr.2012.01.020 [69] Mead, G. and Bernhardt, J. (2011) Physical fitness train- ing after stroke, time to implement what we know: More research is needed. International Journal of Stroke, 6, 506-508. htt p :/ /dx . do i .o r g/10 .1111/j .17 47-4 9 49 .20 11 .00679.x [70] Rimmer, J.H., Wang, E. and Smith, D. (2008) Barriers associated with exercise and community access for indi- viduals with stroke. Journal of Rehabilitation Research and Development, 45, 315-322. http://dx.doi.org/10.1682/JRRD.2007.02.0042 [71] Scianni, A., Teixeira-Salmela, L.F. and Ada, L. (2012) Challenges in recruitment, attendance and adherence of acute stroke survivors to a randomized trial in Brazil: A feasibility study. Revista Brasileira de Fisioterapia, 16, 40-45. http://dx.doi.org/10.1590/S1413-35552012000100008 [72] Suzuki, K., Nakamura, R., Yamada, Y. and Handa, T. (1990) Determinants of maximum walking speed in he- miparetic stroke patients. The Tohoku Journal of Experi- mental Medicine, 162, 337-344. http://dx.doi.org/10.1620/tjem.162.337 [73] Hsu, A., Tang, P. and Jan, M. (2003) Analysis of im- pairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Ar- chives of Physical Medicine and Rehabilitation, 84, 1185- 1193. http://dx.doi.org/10.1016/S0003-9993(03)00030-3 [74] Genthon, N., Rougier, P., Gissot, A.S., Froger, J., Pelis- sier, J. and Perennou, D. (2008) Contribution of each lower limb to upright standing in stroke patients. Stroke, 39, 1793-1799. Copyright © 2013 SciRes. OPEN ACCESS  C. Kilbride et al. / Open Journal of Therapy and Rehabilitation 1 (2013) 40-51 Copyright © 2013 SciRes. OPEN ACCESS 51 http://dx.doi.org/10.1161/STROKEAHA.107.497701 [75] Roland, M. and Torgerson, D.J. (1998) Understanding Controlled Trials: What are pragmatic trials? British Medical Journal, 316, 285. http://dx.doi.org/10.1136/bmj.316.7127.285
|