A. D. Abbas / Open Journal of Nursing 3 (2013) 1-6
498
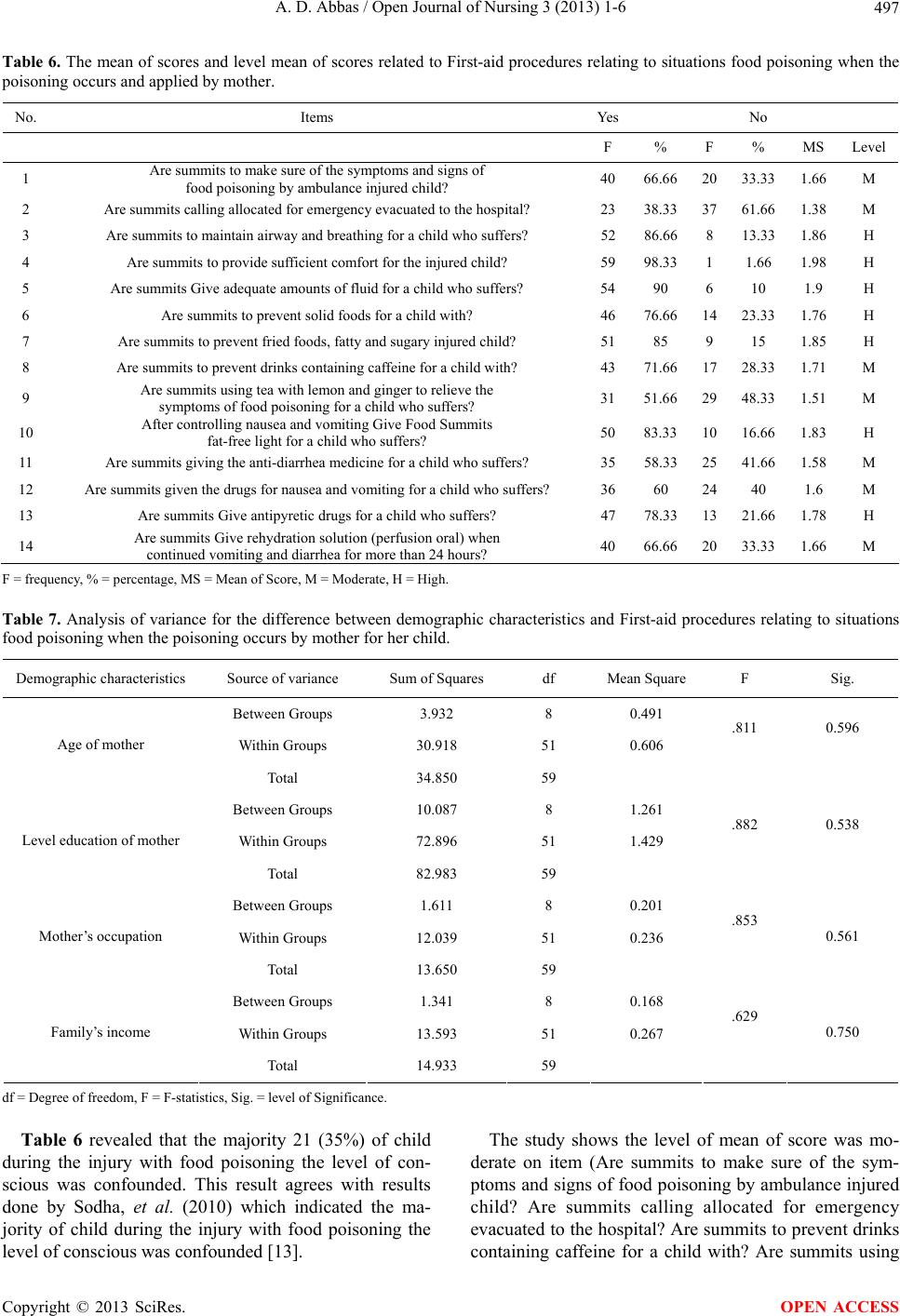
tea with lemon and ginger to relieve the symptoms of
food poisoning for a child who suffers? Are summits giv-
ing the anti-diarrhea medicine for a child who suffers?
Are summits given the drugs for nausea and vomiting for
a child who suffers? And are summits Give rehydration
solution (perfusion oral) when continued vomiting and
diarrhea for more than 24 hours?).
While items (Are summits to maintain airway and
breathing for a child who suffers? Are summits to pro-
vide sufficient comfort for the injured child? Are sum-
mits Give adequate amounts of fluid for a child who suf-
fers? Are summits to prevent solid foods for a child with?
Are summits to prevent fried foods, fatty and sugary in-
jured child? After controlling nausea and vomiting Give
Food Summits fat-free light for a child who suffers? And
are summits Give antipyretic drugs for a child who suf-
fers?) was high in Table 6.
This result agrees with results obtained from study
done by Longphre, et al. (2007) which indicated that
most of items related to First-aid procedures relating to
situations food poisoning when the poisoning occurs was
moderate level mean of scores [14].
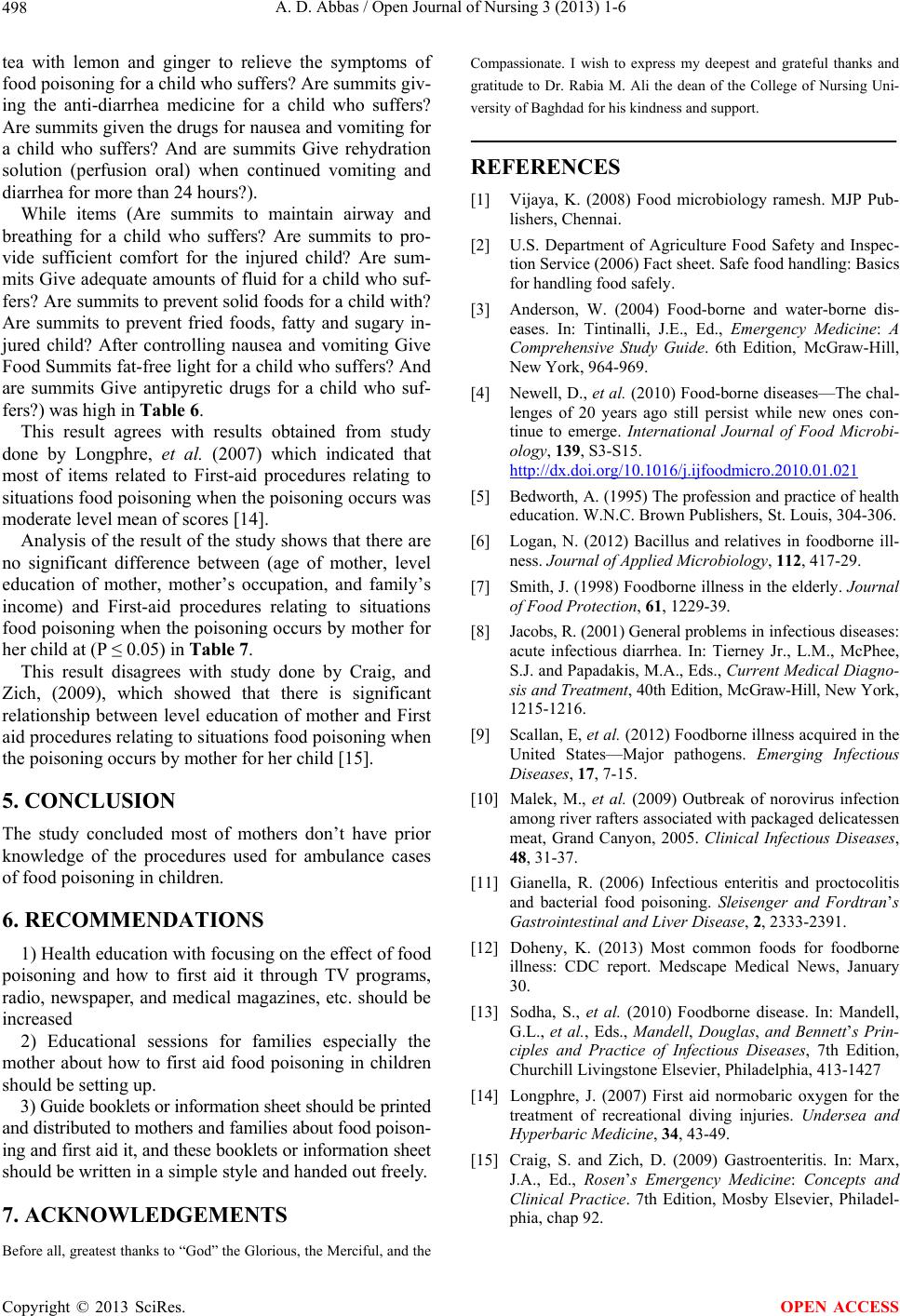
Analysis of the result of the study shows that there are
no significant difference between (age of mother, level
education of mother, mother’s occupation, and family’s
income) and First-aid procedures relating to situations
food poisoning when the poisoning occurs by mother for
her child at (P ≤ 0.05) in Table 7.
This result disagrees with study done by Craig, and
Zich, (2009), which showed that there is significant
relationship between level education of mother and First
aid procedures relating to situations food poisoning when
the poisoning occurs by mother for her child [15].
5. CONCLUSION
The study concluded most of mothers don’t have prior
knowledge of the procedures used for ambulance cases
of food poisoning in children.
6. RECOMMENDATIONS
1) Health education with focusing on the effect of food
poisoning and how to first aid it through TV programs,
radio, newspaper, and medical magazines, etc. should be
increased
2) Educational sessions for families especially the
mother about how to first aid food poisoning in children
should be setting up.
3) Guide booklets or information sheet should be printed
and distributed to mothers and families about food poison-
ing and first aid it, and these booklets or information sheet
should be written in a simple style and handed out freely.
7. ACKNOWLEDGEMENTS
Before all, greatest thanks to “God” the Glorious, the Merciful, and the
Compassionate. I wish to express my deepest and grateful thanks and
gratitude to Dr. Rabia M. Ali the dean of the College of Nursing Uni-
versity of Baghdad for his kindness and support.
REFERENCES
[1] Vijaya, K. (2008) Food microbiology ramesh. MJP Pub-
lishers, Chennai.
[2] U.S. Department of Agriculture Food Safety and Inspec-
tion Service (2006) Fact sheet. Safe food handling: Basics
for handling food safely.
[3] Anderson, W. (2004) Food-borne and water-borne dis-
eases. In: Tintinalli, J.E., Ed., Emergency Medicine: A
Comprehensive Study Guide. 6th Edition, McGraw-Hill,
New York, 964-969.
[4] Newell, D., et al. (2010) Food-borne diseases—The chal-
lenges of 20 years ago still persist while new ones con-
tinue to emerge. International Journal of Food Microbi-
ology, 139, S3-S15.
http://dx.doi.org/10.1016/j.ijfoodmicro.2010.01.021
[5] Bedworth, A. (1995) The profession and practice of health
education. W.N.C. Brown Publishers, St. Louis, 304-306.
[6] Logan, N. (2012) Bacillus and relatives in foodborne ill-
ness. Journal of Applied Microbiology, 112, 417-29.
[7] Smith, J. (1998) Foodborne illness in the elderly. Journal
of Food Protection, 61, 1229-39.
[8] Jacobs, R. (2001) General problems in infectious diseases:
acute infectious diarrhea. In: Tierney Jr., L.M., McPhee,
S.J. and Papadakis, M.A., Eds., Current Medical Diagno-
sis and Treatme nt, 40th Edition, McGraw-Hill, New York,
1215-1216.
[9] Scallan, E, et al. (2012) Foodborne illness acquired in the
United States—Major pathogens. Emerging Infectious
Diseases, 17, 7-15.
[10] Malek, M., et al. (2009) Outbreak of norovirus infection
among river rafters associated with packaged delicatessen
meat, Grand Canyon, 2005. Clinical Infectious Diseases,
48, 31-37.
[11] Gianella, R. (2006) Infectious enteritis and proctocolitis
and bacterial food poisoning. Sleisenger and Fordtran’s
Gastrointestinal and Liver Disease, 2, 2333-2391.
[12] Doheny, K. (2013) Most common foods for foodborne
illness: CDC report. Medscape Medical News, January
30.
[13] Sodha, S., et al. (2010) Foodborne disease. In: Mandell,
G.L., et al., Eds., Mandell, Douglas, and Bennett’s Prin-
ciples and Practice of Infectious Diseases, 7th Edition,
Churchill Livingstone Elsevier, Philadelphia, 413-1427
[14] Longphre, J. (2007) First aid normobaric oxygen for the
treatment of recreational diving injuries. Undersea and
Hyperbaric Medicine, 34, 43-49.
[15] Craig, S. and Zich, D. (2009) Gastroenteritis. In: Marx,
J.A., Ed., Rosen’s Emergency Medicine: Concepts and
Clinical Practice. 7th Edition, Mosby Elsevier, Philadel-
phia, chap 92.
Copyright © 2013 SciRes. OPEN ACCESS