M. DEBNATH, S. KHANNA 251
5. Discussion
The first recorded use of silver nitrate to stimulate clo-
sure of tympanic membrane perforations is by William
Wilde in 1848 [3]. The office chemical myringoplasty
was introduced by Roosa in 1876 and was popularized by
Derlacki in the 1950s who reported good results and the
procedure came to be known as the Derlacki method [4].
In his method he used trichloroacetic acid to cauterize
perforation followed by antibiotic sufflation and covering
with sterile cotton pledgets and prescribing Euthymol ear
drops. Two decades later, Derlacki reported that he and
his colleagues (Shambaugh, Harrison and Clemis) at
Otologic Professional Associates at Chicago and cumula-
tively treated 1277 pars tensa perforations between 1953
and 1972 and had successfully healed at least 1027 of
them (80.4%) [5].
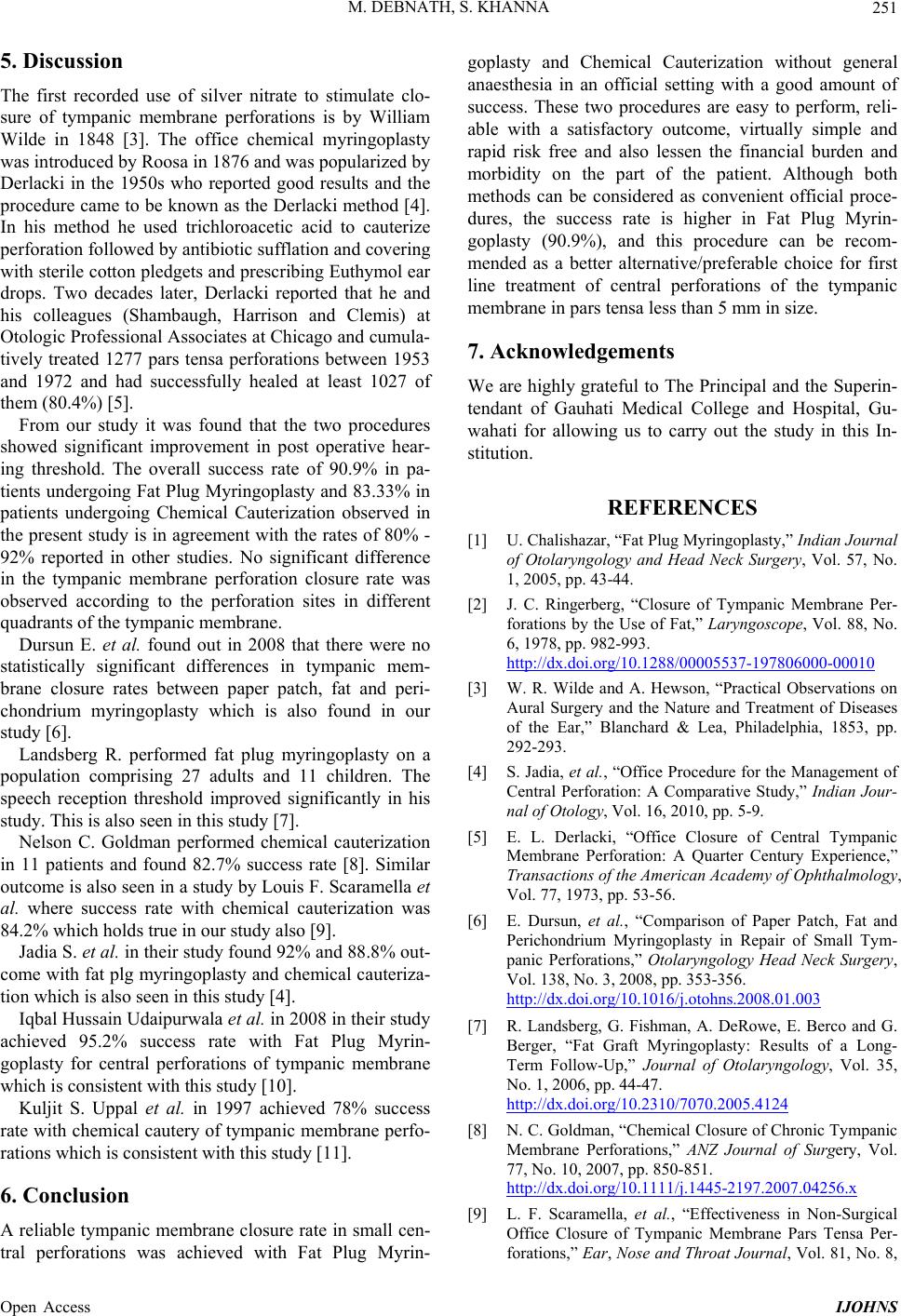
From our study it was found that the two procedures
showed significant improvement in post operative hear-
ing threshold. The overall success rate of 90.9% in pa-
tients undergoing Fat Plug Myringoplasty and 83.33 % in
patients undergoing Chemical Cauterization observed in
the present study is in agreement with the rates of 80% -
92% reported in other studies. No significant difference
in the tympanic membrane perforation closure rate was
observed according to the perforation sites in different
quadrants of the tympanic membrane.
Dursun E. et al. found out in 2008 that there were no
statistically significant differences in tympanic mem-
brane closure rates between paper patch, fat and peri-
chondrium myringoplasty which is also found in our
study [6].
Landsberg R. performed fat plug myringoplasty on a
population comprising 27 adults and 11 children. The
speech reception threshold improved significantly in his
study. This is also seen in this study [7].
Nelson C. Goldman performed chemical cauterization
in 11 patients and found 82.7% success rate [8]. Similar
outcome is also seen in a study by Louis F. Scaramella et
al. where success rate with chemical cauterization was
84.2% which holds true in our study also [9].
Jadia S. et al. in their study found 92% and 88.8% out-
come with fat plg myringoplasty and chemical cauteriza-
tion which is also seen in this study [4].
Iqbal Hussain Udaipurwala et al. in 2008 in their stud y
achieved 95.2% success rate with Fat Plug Myrin-
goplasty for central perforations of tympanic membrane
which is consistent with this study [10].
Kuljit S. Uppal et al. in 1997 achieved 78% success
rate with chemical cautery of tympanic membran e perfo-
rations which is consistent with this study [11].
6. Conclusion
A reliable tympanic membrane closure rate in small cen-
tral perforations was achieved with Fat Plug Myrin-
goplasty and Chemical Cauterization without general
anaesthesia in an official setting with a good amount of
success. These two procedures are easy to perform, reli-
able with a satisfactory outcome, virtually simple and
rapid risk free and also lessen the financial burden and
morbidity on the part of the patient. Although both
methods can be considered as convenient official proce-
dures, the success rate is higher in Fat Plug Myrin-
goplasty (90.9%), and this procedure can be recom-
mended as a better alternative/preferable choice for first
line treatment of central perforations of the tympanic
membrane in pars tensa less than 5 mm in size.
7. Acknowledgements
We are highly grateful to The Principal and the Superin-
tendant of Gauhati Medical College and Hospital, Gu-
wahati for allowing us to carry out the study in this In-
stitution.
REFERENCES
[1] U. Chalishazar, “Fat Plug Myringoplasty,” Indian Journal
of Otolaryngology and Head Neck Surgery, Vol. 57, No.
1, 2005, pp. 43-44.
[2] J. C. Ringerberg, “Closure of Tympanic Membrane Per-
forations by the Use of Fat,” Laryngoscope, Vol. 88, No.
6, 1978, pp. 982-993.
http://dx.doi.org/10.1288/00005537-197806000-00010
[3] W. R. Wilde and A. Hewson, “Practical Observations on
Aural Surgery and the Nature and Treatment of Diseases
of the Ear,” Blanchard & Lea, Philadelphia, 1853, pp.
292-293.
[4] S. Jadia, et al., “Office Procedure for the Management of
Central Perforation: A Comparative Study,” Indian Jour-
nal of Otology, Vol. 16, 2010, pp. 5-9.
[5] E. L. Derlacki, “Office Closure of Central Tympanic
Membrane Perforation: A Quarter Century Experience,”
Transactions of the American Academy of Ophthalmology,
Vol. 77, 1973, pp. 53-56.
[6] E. Dursun, et al., “Comparison of Paper Patch, Fat and
Perichondrium Myringoplasty in Repair of Small Tym-
panic Perforations,” Otolaryngology Head Neck Surgery,
Vol. 138, No. 3, 2008, pp. 353-356.
http://dx.doi.org/10.1016/j.otohns.2008.01.003
[7] R. Landsberg, G. Fishman, A. DeRowe, E. Berco and G.
Berger, “Fat Graft Myringoplasty: Results of a Long-
Term Follow-Up,” Journal of Otolaryngology, Vol. 35,
No. 1, 2006, pp. 44-47.
http://dx.doi.org/10.2310/7070.2005.4124
[8] N. C. Goldman, “Chemical Closure of Chronic Tympanic
Membrane Perforations,” ANZ Journal of Surgery, Vol.
77, No. 10, 2007, pp. 850-851.
http://dx.doi.org/10.1111/j.1445-2197.2007.04256.x
[9] L. F. Scaramella, et al., “Effectiveness in Non-Surgical
Office Closure of Tympanic Membrane Pars Tensa Per-
forations,” Ear, Nose and Throat Journal, Vol. 81, No. 8,
Open Access IJOHNS