G. P. Guimarães, J. G. Martini / Open Journal of Obstetrics and Gynecology 3 (2013) 35-40 37
in line with results presented by the Min istry of Health [4]
highlighting Southern Brazil as the largest proportion of
births alive in this age group, whereas the Northern re-
gion presents the highest rates of high-risk pregnancies
in teens.
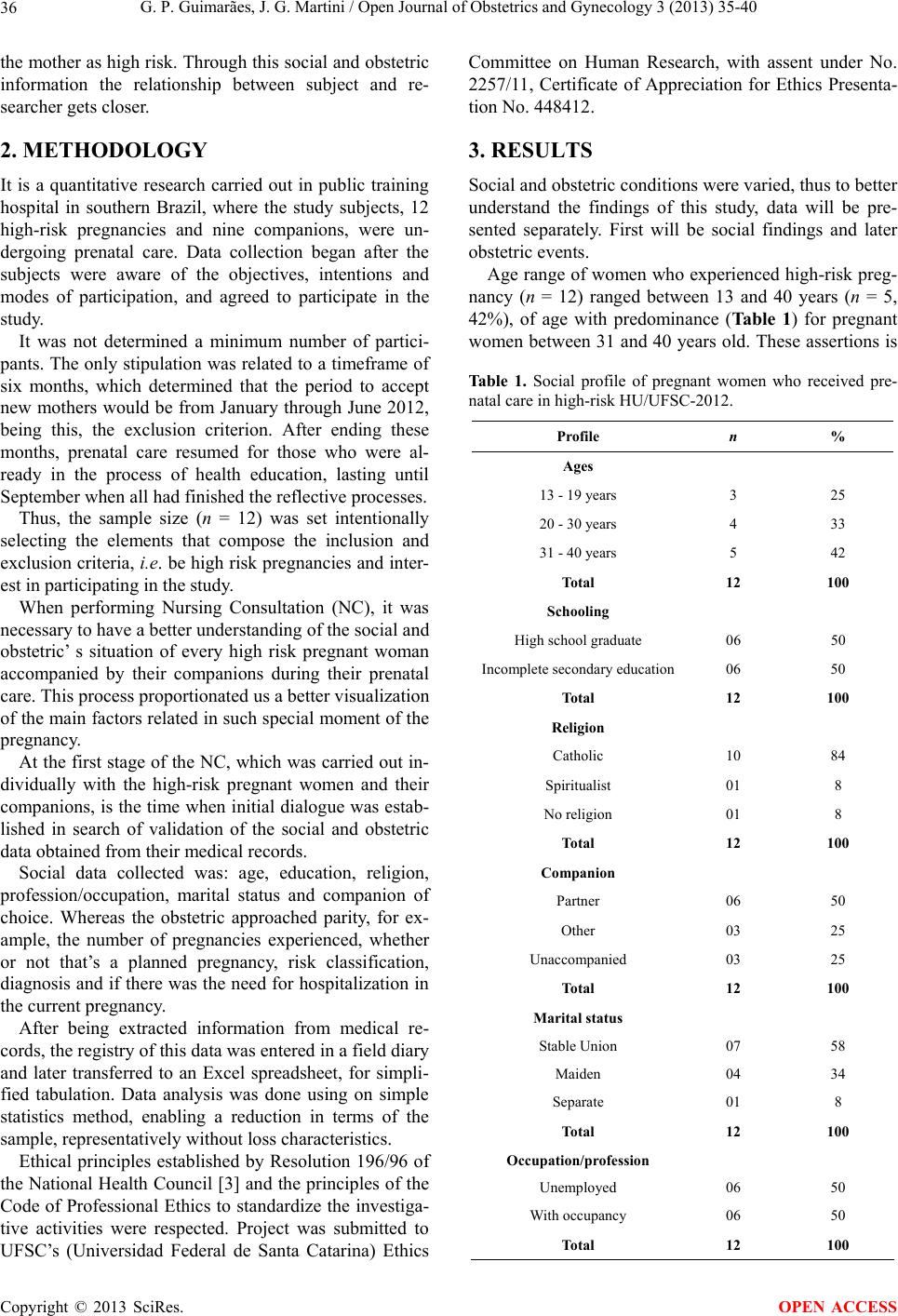
The lower age group of women who underwent high
risk prenatal in this study was adolescents (n = 3, 25%).
Age range considered for teenagers in this study was 13
through 19 years old. This is taking into account the
minimum age advocated by Law 8069 of July 13, 1990,
which is provided for in the Child and Ad olescent Statute.
Teen is a person who is between the age of twelve and
eighteen years of age. World Health Organization (WHO)
adopts the rage between 15 and 19 years [5] for teens.
It was observed that the pregnant women in this study
were all literate (n = 12, 100%), varying only in the level
of education, being 50% high school graduate, and 50%
incomplete secondary education. The fact that these
women had a certain degree of education that provided
not only practical, visual and life knowledge, but also
written words and knowledge exchange during the proc-
ess of reflection-action-reflection. Some even had read
about the risk they were experiencing, and sought for
information in the virtual universe of the internet or
through people who reported their personal experiences
of pregnancy on their blogs, a space on the internet or-
ganized in reverse chronological order, focusing on a
particular theme, which can be written by a variable
number of people who share their personal experiences
and can post pictures, text, etc.
However, despite early adoption by the pregnant
women of electronic media search for knowledge related
to their situation, many readings came distorted, gener-
ating higher anxiety levels in them and their companions
and increasing emotional instability, requiring constant
back and forth to bring them to th eir reality and closer to
the context in which they were living .
Religion, predominating Catholicism (84%), was some-
thing strongly emphasized by the pregnant women,
which in conjunction with prenatal care provided com-
fort, motivation and strength to continue the journey of
risky pregnancy. Having faith was the base to keeping
them strong and to facing obstacles, besides the strong
presence of their companion, which provided greater
security in times of difficulty, o f expectations and also of
happiness.
The choice of companions by the pregnant women
during prenatal care was varied. M ost women 50% (n = 6)
were accompanied by their partners. Other choices of
companions were the mother and sister-in-law/God-
mother. It stood up the fact that some women 25% did
not have a companion, having to face the difficulties of
the high-risk pregnancy without any support, whether
from family, friends or someone who they could share
their feelings with and encourage a dialogic relationship
during the prenatal care assistance meetings.
An important fact that should be noted is the marital
status of the 12 pregnant women being followed. Most
women had a companion through a domestic union (sta-
ble union—Brazilian regulation) 58% (n = 7), allowing
for the sharing of moments experienced during the preg-
nancy. This study had a significant number of unmar-
ried pregnant women, a total of 34% (n = 4).
The constitution of the family income is exercised
with balance by the companion, considering that 50% of
pregnant women did not any realize profit-making ac-
tivities, devoting most of their time to domestic activities.
On the other hand, the other 50% of women from this
study had a professional occupation, such as: cleaning
ladies; maid; beautician; seamstress, bartender and op-
erator. Beside these activities, they still took care of their
home by performing domestic activities and, some, also
adopted the role of br eadwinner, denoting multiple work-
ing shifts.
The results presented so far allowed for a view of the
pregnant women’s social profile, focus of this study;
however, this is not enough to glimpse, in a global scale,
the high-risk pregnancy. For that, we present the obstet-
ric profile, trying to correlate the social and obstetric fac-
tors that pregnant women underwent during the high-risk
prenatal care which allows us to do broader and more
appropriate critical analysis.
Obstetric findings reflect the women’s profile since the
first moment, being that most of these women said they
had not planned for the pregnancy. Only some had
planned with their companions when to get pregnant.
The fact majority had not planned for the pregnancy may
justify the beginning of their prenatal care assistance
only in the second or third trimester of the pregnancy.
With respect to the parity of the women (Table 2),
there was a certain proximity between first pregnancy,
those who a generating their first child and second preg-
nancy. In greater number (n = 5, 42%) it was the group
of women that had had three or more pregnancies, which
are classified as multigravida.
Previous history of the studied pregnant women shows
that the minority of these women had risk situations in
some of their previous pregnancies, corresponding to
17%. Most women received low-risk prenatal care at
their local Basic Health Units—BHU, in contrast with
the current pregnancy where they were classified as
high-risk pregnancies and requiring to perform prenatal
at hospital of reference for such assistance.
After these pregnant women were considered of high-
risk and being monitored by the specialized prenatal care,
it was observed that the majority o f these high risk preg-
nant women 92% (n = 11) displayed a serene and un-
eventful pregnancy, with no need for hospitalization for
Copyright © 2013 SciRes. OPEN ACCESS