Vol.2, No.8, 448-449 (2013) Case Reports in Clinical Medicine
http://dx.doi.org/10.4236/crcm.2013.28117
A case of penile gangrene
Bobby Desai*, Irina Brennan, Brandon Allen
Department of Emergency Medicine, University of Florida College of Medicine, Gainesville, USA;
*Corresponding Author: bdesai@ufl.edu
Received 28 August 2013; revised 30 September 2013; accepted 20 October 2013
Copyright © 2013 Bobby Desai et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Penile gangrene is a rare entity and is usually
associated with significant trauma. We report on
a self-inflicted cause of penile gangrene in a pa-
tient who sought enhancement.
Keywords: Penis; Gangrene; Enhancement
1. INTRODUCTION
Penile modification is done for many reasons,
including peer pressure, enhancement of penile girth and
length, and for a perceived increase in female pleasure
[1]. There can be significant complications of modifica-
tion, from the urethral injury, to penile abscesses. Late
complications of modifications include chronic pain and
erectile dysfunction [2]. Penile modification is becoming
more commonplace in the United States [2].
2. CASE
A 55-year-old man with no significant past medical
history presented to the emergency department with the
waiting room triage complaint of priapism. He reported
progressive worsening of penile pain and swelling for
three weeks after an attempt at male enhancement at
home. The patient had no difficulty with urination and
denied fevers or chills. His review of systems was non-
contributory. On physical examination, his vital signs
were normal, with no fever. His cardiac, respiratory,
abdominal and neurologic exam was normal. On physi-
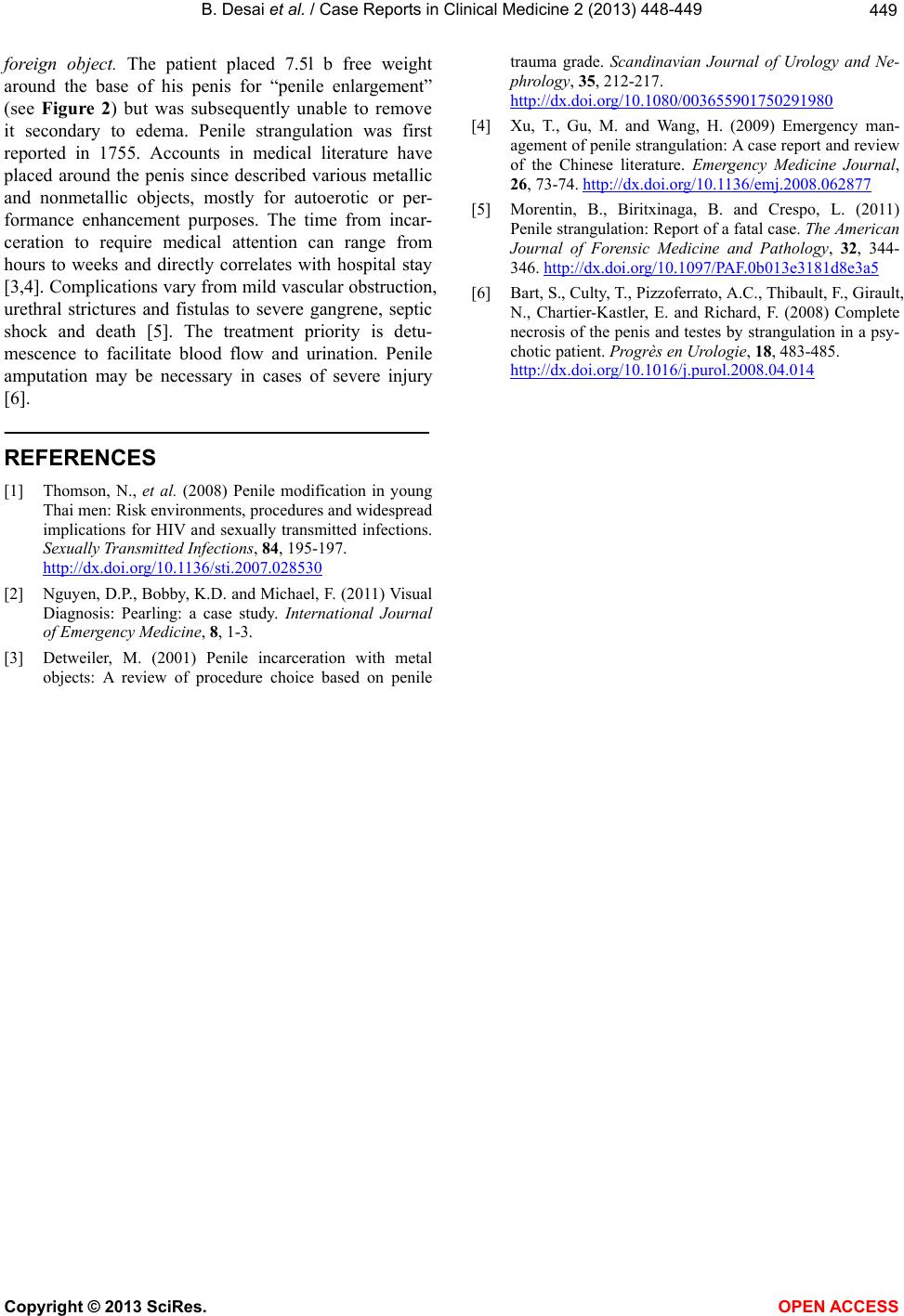
cal examination of his inguinal and genital area, a foul-
smelling, poikilothermic, edematous and insensate penis
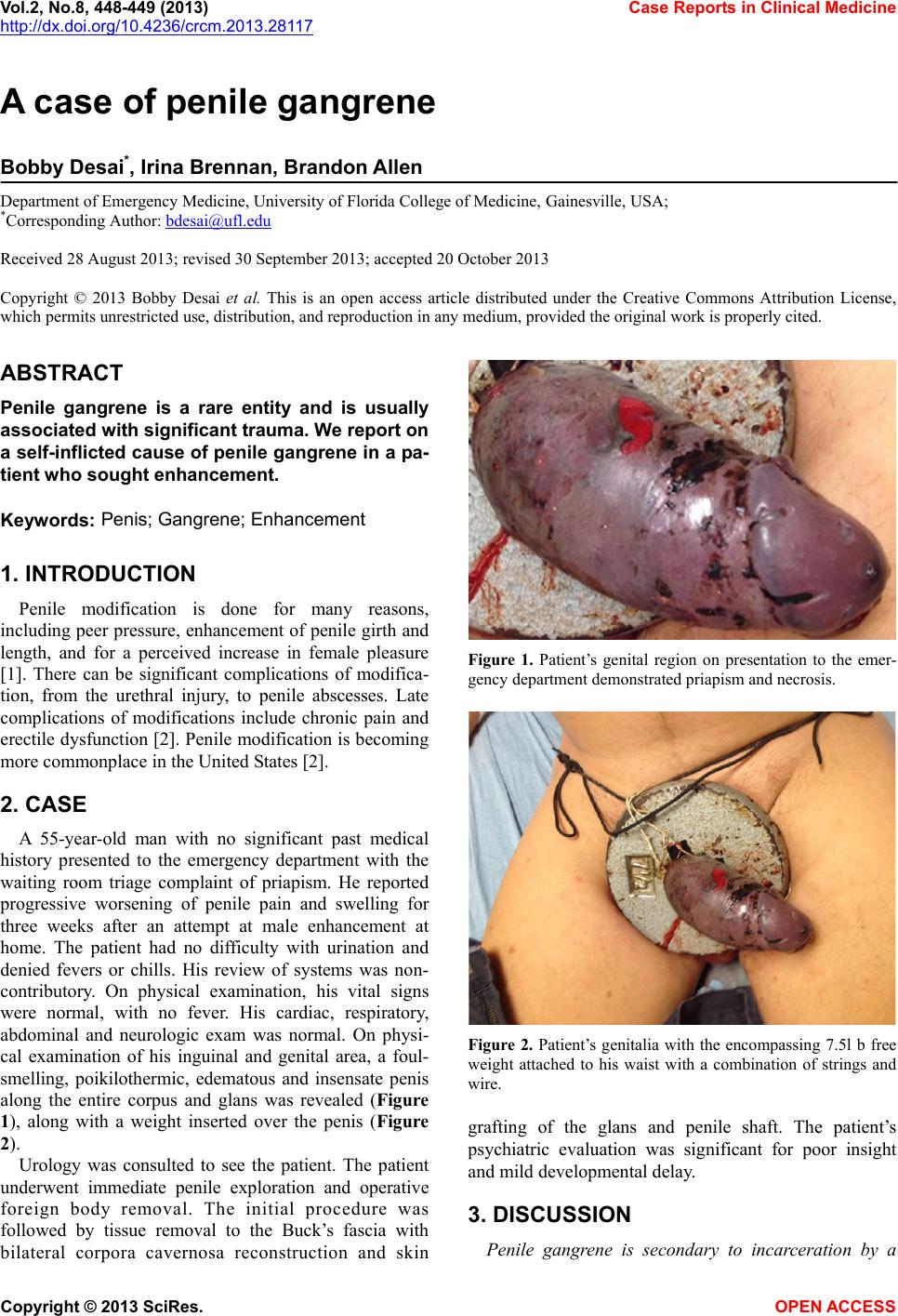
along the entire corpus and glans was revealed (Figure
1), along with a weight inserted over the penis (Figure
2).
Urology was consulted to see the patient. The patient
underwent immediate penile exploration and operative
foreign body removal. The initial procedure was
followed by tissue removal to the Buck’s fascia with
bilateral corpora cavernosa reconstruction and skin
Figure 1. Patient’s genital region on presentation to the emer-
gency department demonstrated priapism and necrosis.
Figure 2. Patient’s genitalia with the encompassing 7.5l b free
weight attached to his waist with a combination of strings and
wire.
grafting of the glans and penile shaft. The patient’s
psychiatric evaluation was significant for poor insight
and mild developmental delay.
3. DISCUSSION
Penile gangrene is secondary to incarceration by a
Copyright © 2013 SciRes. OPEN ACCESS