E. Kelechi et al. / Modern Chemotherapy 2 (2013) 69-72
70
blood pressure (80/50 mmHg). Her chest was clinically
clear, while she had suprapubic tenderness and offensive
vaginal discharge associated with altered blood and cer-
vical excitation tenderness. There was no suburethral or
cervical lesion. Due to her previous conflicting investi-
gation reports, the patient was booked for examination
under anesthesia, where she had torrential bleeding that
was coming from uterine cavity. Thus, a pregnancy test
was ordered that led to the diagnosis of choriocarcinoma.
Although a titrated serum hCG could not be done, an
analysis of urine hCG was positive at 1:200 d ilution. Her
blood group was B+, while her husband’s was O+. Her
PCV on admission was 12% and her total white blood
cell count, platelet count, serum electrolytes and urea
were within normal limits.
She was successfully resuscitated with antibiotics and
massive blood transfusion (20 units). Further evaluation
did not show any evidence of lung, liver or brain metas-
tases. Meanwhile, prognostic scoring of the patient was
uncertain as she was not “pregnant” and the serum hCG
could not be assayed, but she was placed at clinical stage
I (tumour confined to the uterus). She was then com-
menced on cancer chemotherapy.
Therapy was instituted using Methotrexate 50 mg on
days 1, 3, 5 and 7; Folinic acid 7 mg on days 2, 4, 6 and
8; Cyclophosphamide 650 mg daily for 5 days (in sa-
line), and Adriamycin 75 mg stat on day 1. Following
the first course of chemotherapy, the bleeding ceased and
the patient made tremendous clinical improvement. The
course was repeated on day 21, while the patient was
consistently monitored for signs of toxicity. Pregnancy
test became negative at the end of the second course. She
was scheduled to receive one more course of chemo-
therapy but she defaulted due to high cost of the cyto-
toxic drugs and the apparent relief of her symptoms. She
presented three months later with relapse and features of
metastasis and died.
3. DISCUSSION
Gestational trophoblastic disease most commonly fol-
lows molar pregnancy and may also occur following
normal or ectopic pregnancies and spontaneous or thera-
peutic abortions. Its incidence varies with figures as high
as 1 in 120 pregnancies in some areas of Asia and South
America, compared to 1 in 1200 in United States [5]. In
the United Kingdom, it has a calculated in cidence of 1 in
714 live births [3]. Metastatic gestational trophoblastic
disease occurs in 4% patients after local management of
Hydatidiform mole [5]. The incidence of choriocarci-
noma after complete hydatidiform mole is about 1000
times greater than after a normal pregnancy . It may oc-
cur ab initio as in the case presented [1,6]. Choriocarci-
noma is a rare tumour. In western countries, the inci-
dence is 1 in 45,000 to 50,000 pregnancies [5,7]. Higher
incidence is reported from, Africa, Asia and South Ame-
rica [8]. Majority of cases occur in women aged less than
35 year s of age [5].
Choriocarcinoma is suspected when there is persistent
or irregular uterine haemorrhage, following abortion or
hydatidiform mole. However, as illustrated in this case, it
could also be suspected in cases of undiagnosed vaginal
bleeding, even in the absence of pregnancy. Rapid growth
and haemorrhage make the tumour a gynecological
emergency. Metastasis may occur in lung, pelvis and
vagina. Rare sites include gastrointestinal tract, spleen,
and kidney. The central nervous system is seldom in-
volved in the absence of pulmonary metastasis [2]. Meta-
static disease occurs in 4% of patients after local man-
agement of hydatidiform mole and very rarely after term
pregnancies or abortions [1]. Sometimes they may be
combined with malignant germ cells components; and it
may be difficult to differentiate a primary tumour from a
metastasis. For females in non reproductive age group,
the tumours may arise from ovarian germ cells, which is
histologically similar to gestational uterine choriocarci-
noma [6].
Hitherto, serum hCG assay has remained the key fac-
tor in diagnosis and monitoring of the progression of the
disease. This has made clinical prognostic scoring easy
and objective, as the serum hCG provides a sensitiv e and
reliable indicator of the body burden of the tumour, its
progression and regression in response to treatment [1].
However, in resource-limited settings, like ours, serial
dilution test for urine hCG has also proven to be a useful
diagnostic tool. The emphasis, however, should be to
correlate the urine titers with serum values. This will
enhance prognostication of patients for appropriate che-
motherapy. According to I.A. McNeish et al. [9], proper
classification of patients (as low risk) did not compro-
mise outcome, but rather prevented undue exposure to
potentially carcinogenic chemotherapy.
Traditionally, patients with uterine choriocarcinoma
have been categorized as low risk (score of 0 to 5), me-
dium risk (score of 6 to 9) and high risk (score > 9), us-
ing the prognostic scoring system [1]. This enables ra-
tional use of chemotherapy with emphasis on the risk of
developing resistance. However, I.A. McNeish et al. [9]
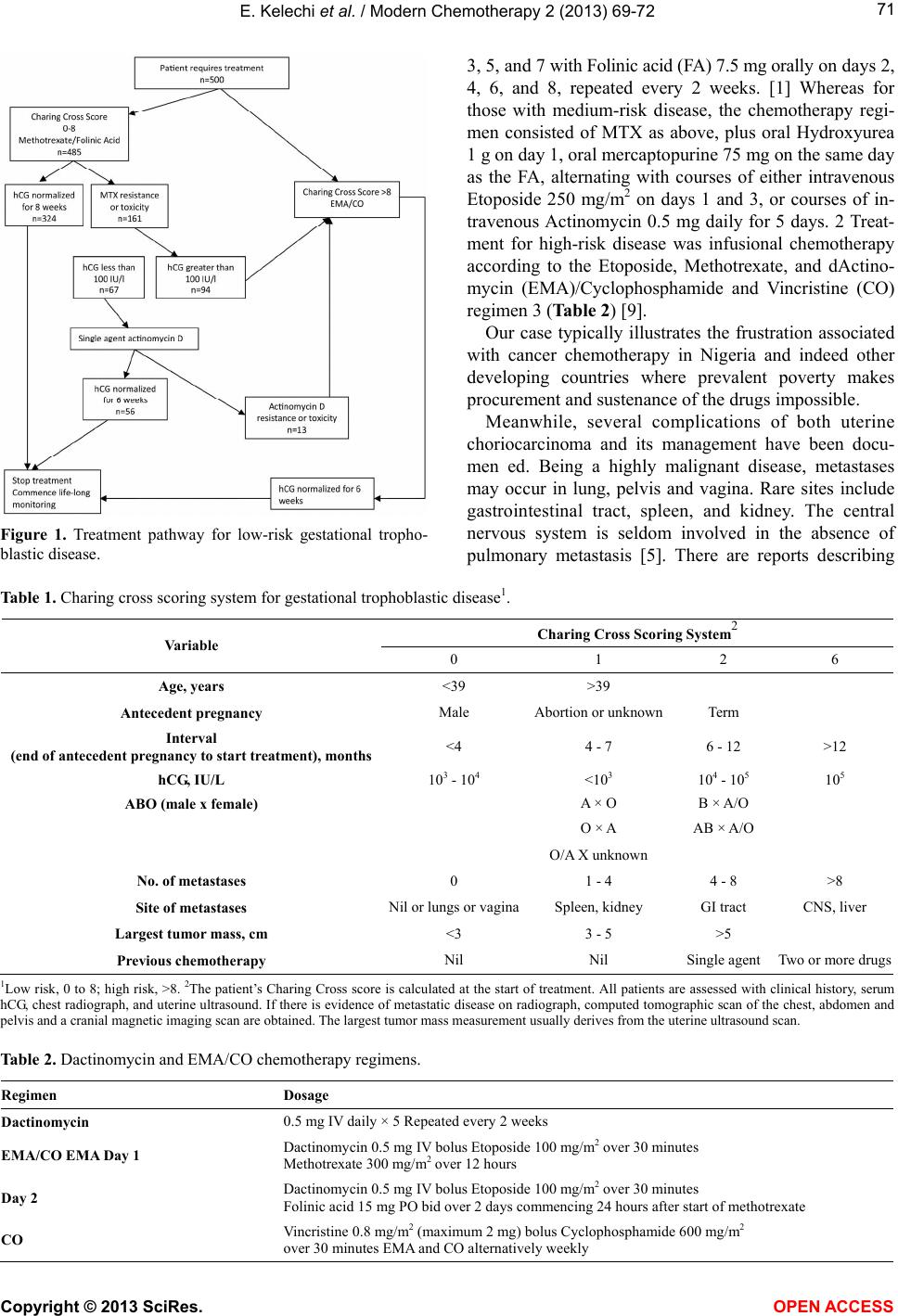
have proposed a new scoring system: Charing Cross
scoring system (Table 1), which is intended to further
reduce the risk of undue exposure to chemotherapy. This
new system proposes the use of Methotrexate-Folinic
acid regimen for low risk disease (score 0 - 8), while
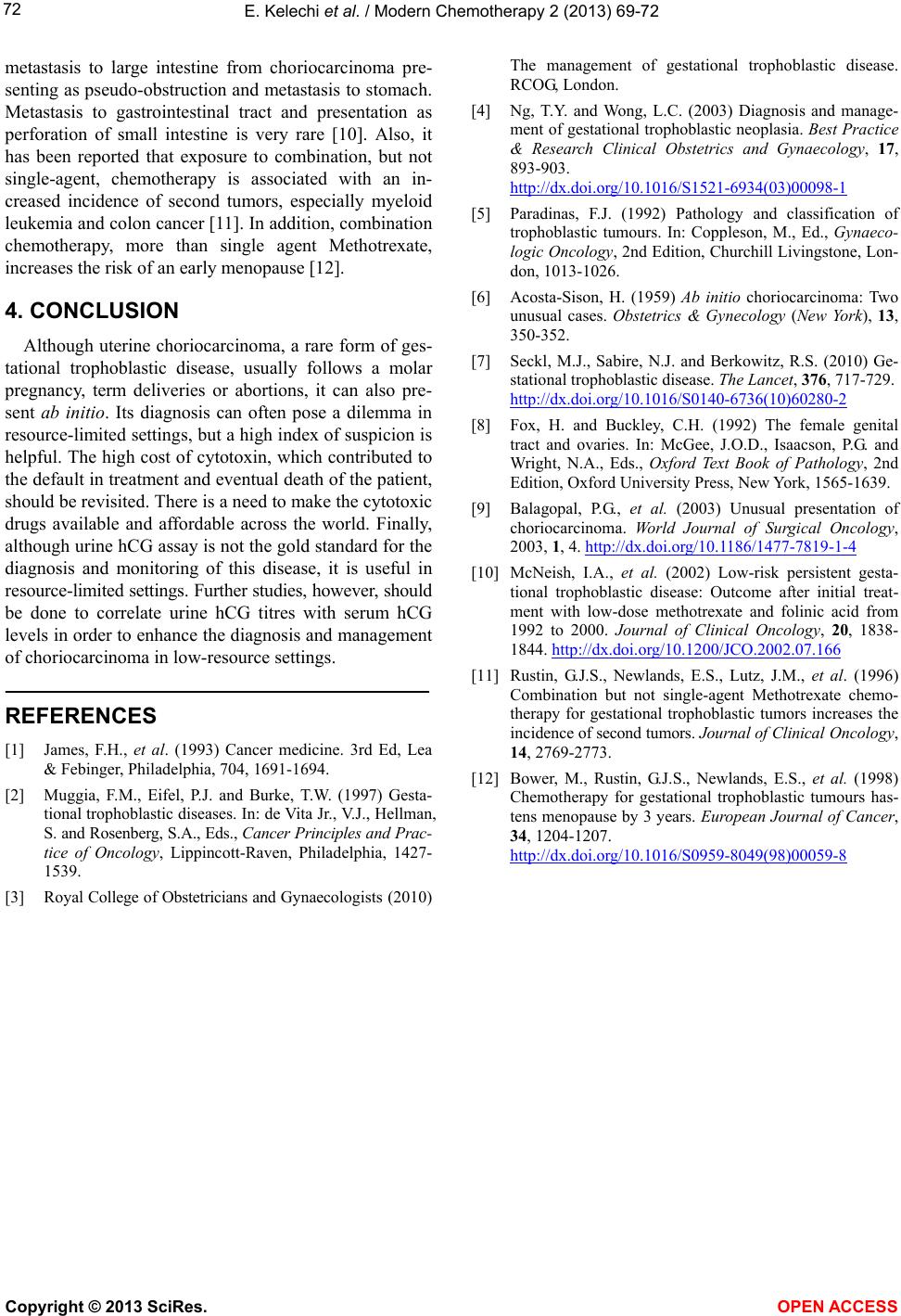
EMA/CO (Etoposide, Methotrexate, Actinomycin D,
Cyclophosphamide and Oncovin) is reserved for high
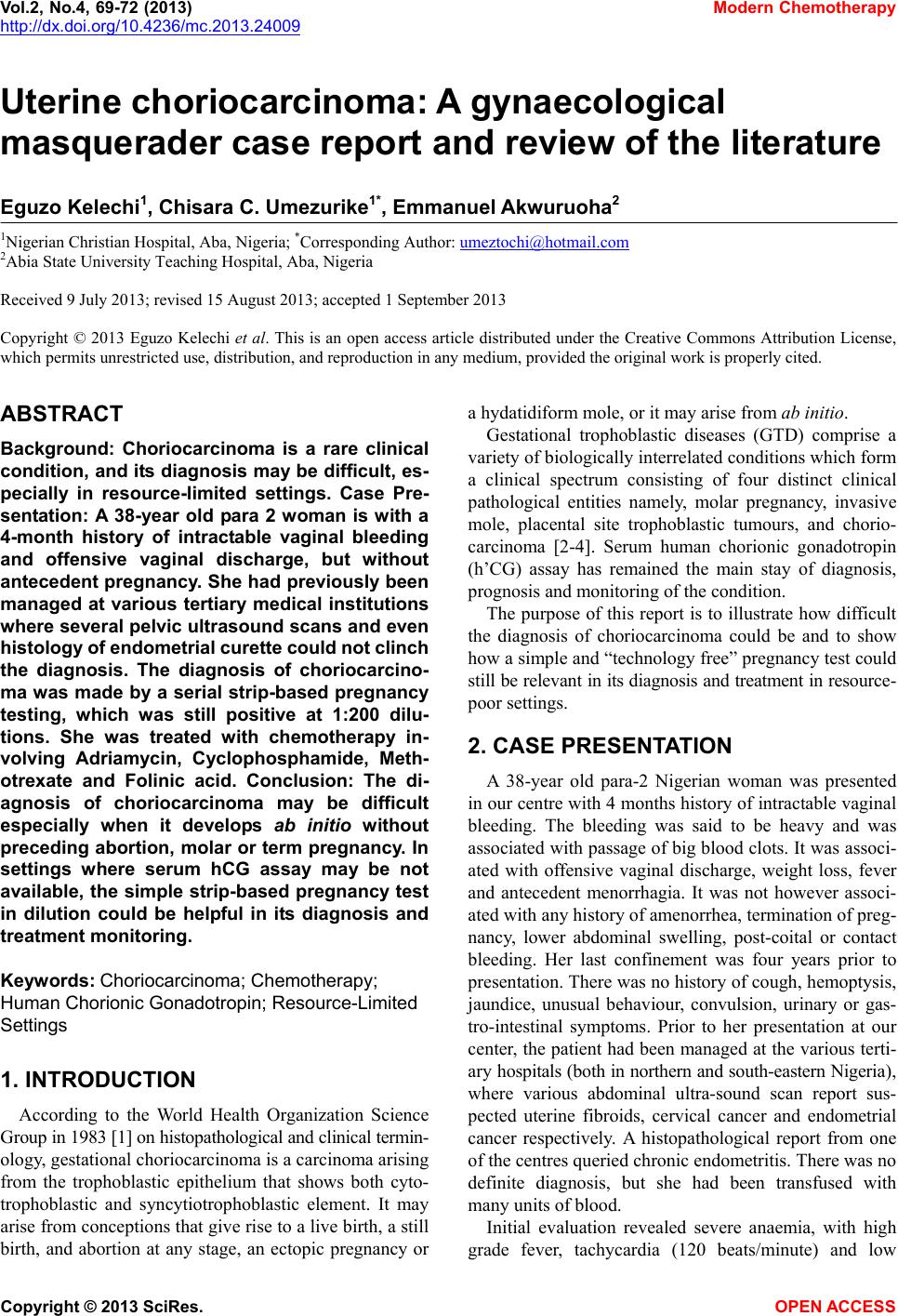
risk disease (score > 8). An algorithm (Figure 1) has also
been developed to enhance case management.
Initial treatment for those with low-risk disease was
Methotrexate (MTX) (50 mg intramuscularly on days 1,
Copyright © 2013 SciRes. OPEN A CCESS