Open Journal of Urology, 2013, 3, 253-255
http://dx.doi.org/10.4236/oju.2013.36047 Published Online October 2013 (http://www.scirp.org/journal/oju)
Tips for Office-Based Transurethral Biopsy and
Fulguration as a Treatment of Tiny Bladder Tumors*
Teiichiro Aoyagi1#, Isao Kuroda1, Masaaki Tachibana2
1Tokyo Medical University, Ibaraki Medical Center, Inashiki, Japan
2Toky o Medical University, T o kyo, Japan
Email: #aoyagite@tokyo-med.ac.jp
Received August 8, 2013; revised September 6, 2013; accepted September 14, 2013
Copyright © 2013 Teiichiro Aoyagi et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Among the patients who underwent outpatient cystoscopy as a follow up of bladder cancer, quite a few patients are ob-
served tiny papillary lesions suspicious for tumor recurrence. Tran surethral biop sy and/or resection under spinal or gen-
eral anesthesia in a hospitalized setting are the usual procedures for th is kind of patients, even thou gh these procedures
are simple and brief. We tried transurethral biopsy and fulguration as a treatment for very small bladder tumor in an
outpatient setting and here describe tips for these procedures. Olympus CYF-VA flexible cystoscope, a 3 Fr. diathermy
probe, monopolar electrosurgical unit were used. No additional anesthetics except for 10 ml of 2% Xylocaine gel ap-
plied to (male patient’s) urethra as an initial flexible cystoscopic procedure, was required for tumor treatment. Distilled
water was used as an irrigation fluid. Experienced tips of the procedures to avoid tumor recurrence are as follows: tu-
mor should be one location, size of the tumor should be less than 5 mm, bladder should be washed several times after
the fulguration with hundreds ml of distilled water. We conclud e that outpatient biopsy and fulguration for tiny bladder
tumor is effective and less invasive procedure as a treatment of bladder cancer patients.
Keywords: Transurethral Surgery; Bladder Cancer; Office Urology; Fulguration; Biopsy
1. Introduction
Office-based cystoscopic examination is a usual estab-
lished method as an initial and postoperative surveillance
of bladder tumor [1]. During the follow up period, small,
low grade and superficial bladder tumor recurs in quite a
few patients [2]. Although experience and efficacy of
office-based fulguration for low grade papillary lesions
has been reported previously, this procedure does not
performed routinely in the clinical practice, presumably
because there is no precise explanation on actual meth-
odology and safety [3-5]. However, considering increas-
ing comorbidities, use of anti-coagulation medication,
economic restriction and so on, ambulatory treatment for
these lesions should be beneficial both for patients and
surgeons [6]. Here, we present the tips of ambulatory
biopsy and fulguration treatment for tiny bladder papil-
lary lesions with some improvements after experiences of
failure cases.
2. Patients and Methods
Fourteen patients, 19 procedures were enrolled in this
report. The patient profiles are listed in the Table 1. All
the patients had the history of transurethral resection
(TUR) or nephroureterectomy surgery under spinal or
general anesthesia previously, and followed with repeat
surveillance flexible cystoscopy in an outpatient setting.
Safety to use diathermia for these patients was confirmed
by previous surgery, and informed consent on the treat-
ment of ambulatory procedures was made by patient’s
signature. This report does not violate ethical standards
of the Declaration of Helsinki and its revisions. No addi-
tional anesthetics except for 10 ml of 2% Xylocaine gel
applied to (male patient’s) urethra as an initial flexible
cystoscopic procedure, was required for tumor treatment.
Olympus (Tokyo, Japan) CYF-VA flexible cystoscope
and Versa Pro unit, Takei (Tokyo Japan) monopolar
electrosurgical unit B-1, Olympus flexible biopsy forceps
and 3 Fr. Takei Bugbee ureteroscope electrode were used.
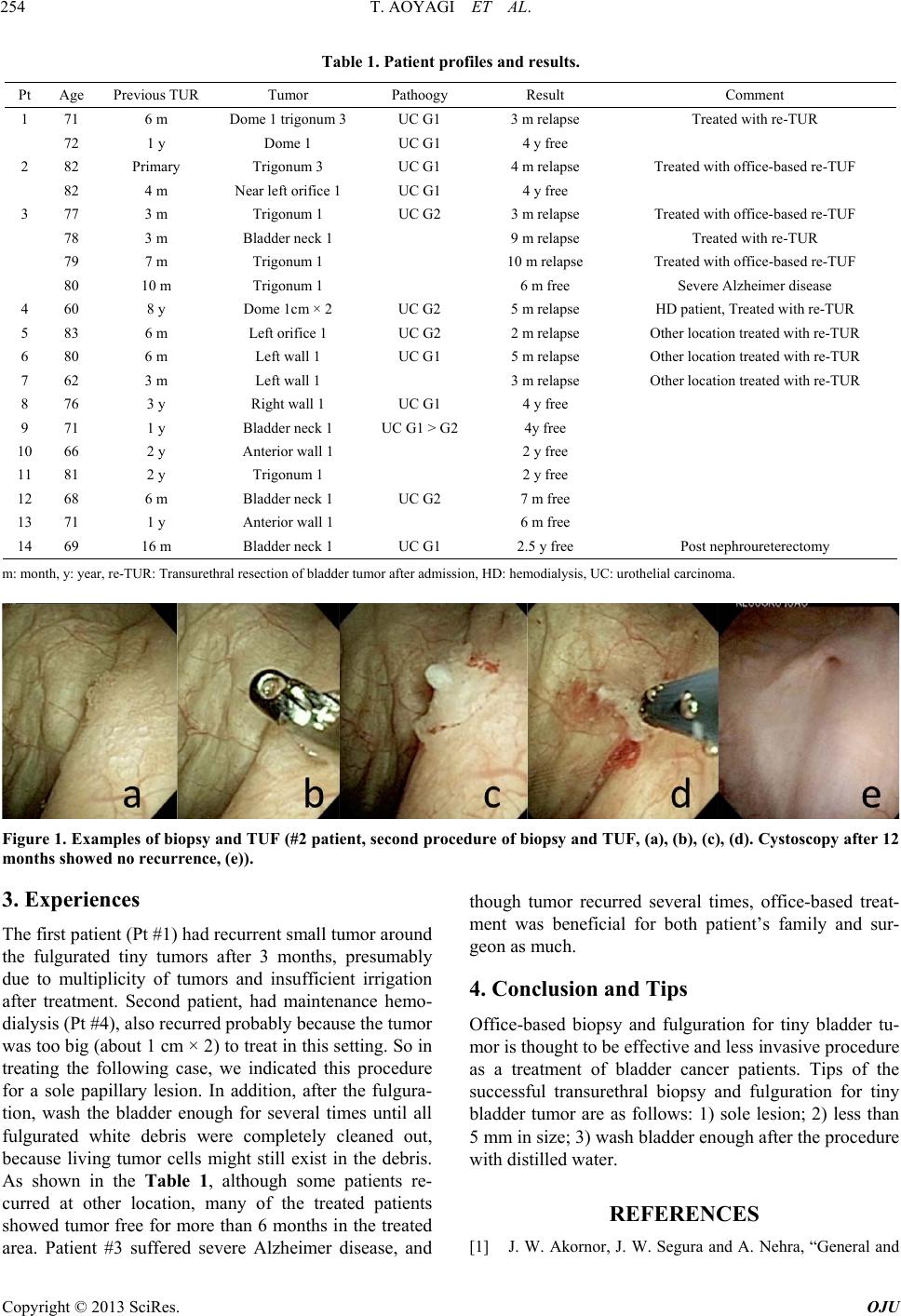
Normal saline was used for observation, and distilled
water was used for treatment as irrigation fluid (Figure
1).
*The authors declare that they have no conflict of interests, no funds
and no grant on thi s project.
#Corresponding author.
C
opyright © 2013 SciRes. OJU