 Open Journal of Stomatology, 2013, 3, 338-343 OJST http://dx.doi.org/10.4236/ojst.2013.37057 Published Online October 2013 (http://www.scirp.org/journal/ojst/) Case report involving temporomandibular dysfunction, eagle’s syndrome and torus mandibularis —Multidisciplinary approaches Takami Hirono Hotta1, Cássio Edvard Sverzut2, Marcelo Palinkas3*, César Bataglion3, Melissa Oliveira Melchior3, Patrícia Tiemy Hirono Hotta4, Sérgio Olavo Petenusci5, Simone Cecilio Hallak Regalo5 1Department of Dental Materials and Prosthodontics, Ribeirão Preto School of Dentistry, University of São Paulo, Ribeirão Preto, Brazil 2Department of Oral and Maxillofacial Surgery and Periodontology, Ribeirão Preto School of Dentistry, University of São Paulo, Ribeirão Preto, Brazil 3Department of Restorative Dentistry, Ribeirão Preto School of Dentistry, University of São Paulo, Ribeirão Preto, Brazil 4Department of Surgery, Prosthodontics and Maxillofacial Traumatology, São Paulo Dental School, University of São Paulo, São Paulo, Brazil 5Department of Morphology, Stomatology and Basic Pathology, Ribeirão Preto School of Dentistry, University of São Paulo, Ribeirão Preto, Brazil Email: *palinkas@usp.br Received 6 August 2013; revised 6 September 2013; accepted 23 September 2013 Copyright © 2013 Takami Hirono Hotta et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT The prevalence of torus mandibularis, Eagle’s syn- drome and parafunctional activity was reported to be higher in patients with temporomandibular joint dysfunction and might be useful as an indicator of increased risk of temporomandibular disorders. This study case report was to evaluate a 62-year-old fe- male patient, with limited mandibular and cervical movements, articular and muscular pain, ear fullness, irritation of the lingual mucosa, discomfort associated with movement of her tongue, involving temporo- mandibular dysfunction, torus mandibularis and Ea- gle’s syndrome. The treatment comprehended the collection of data of Helkimo’s Clinical Dysfunction Index, electromyographic activity of the masseter and temporalis muscles in rest position and bite force, masticatory efficiency, speech evaluation and oclusal splint, after the excision of the stylohyoid process and mandibularis torus. The authors found a decrease in electromyographic activity of masticatory muscles, a reduction of painful symptoms throughout the region muscular and joint pains, an increase in the ampli- tude of mandibular movements, an improvement in masticatory efficiency and an increase in bite force. Keywords: Temporomandibular Dysfunction; Eagle’s Syndrome; Torus Mandibularis; Electromyography; Bite Force 1. INTRODUCTION Torus mandibularis (TM) is an exophytic bone growth that usually occurs bilaterally along the lingual surface of the premolar area of the mandible, superior to the mylo- hyoid ridge [1,2]. In patients who are completely or par- tially edentulous, the occurrence of TM can interfere with the prosthetic treatment plan in dentate patients. TM can interfere with masticatory and speech functions. Therefore, even when asymptomatic, the surgical re- moval of the tori is indicated in these cases [3,4]. The etiology of TM has been investigated by several authors; however, no consensus has been reached. It is generally accepted that genetic factors contribute to the occurrence of TM [5-8]. The prevalence of both TM and parafunctional activity has been reported to be higher in patients with tem- poromandibular joint dysfunction [9], and therefore, these factors may be useful indicators of an increased risk of temporomandibular disorders in some patients. Eagle’s syndrome affects the head and neck structures and produces headache, earache, changes in swallowing and speech, and facial, cervical and eye pain [10-14]. Symptoms may also occur along the distribution of the external and internal carotid artery branches due to com- *Corresponding author. OPEN ACCESS 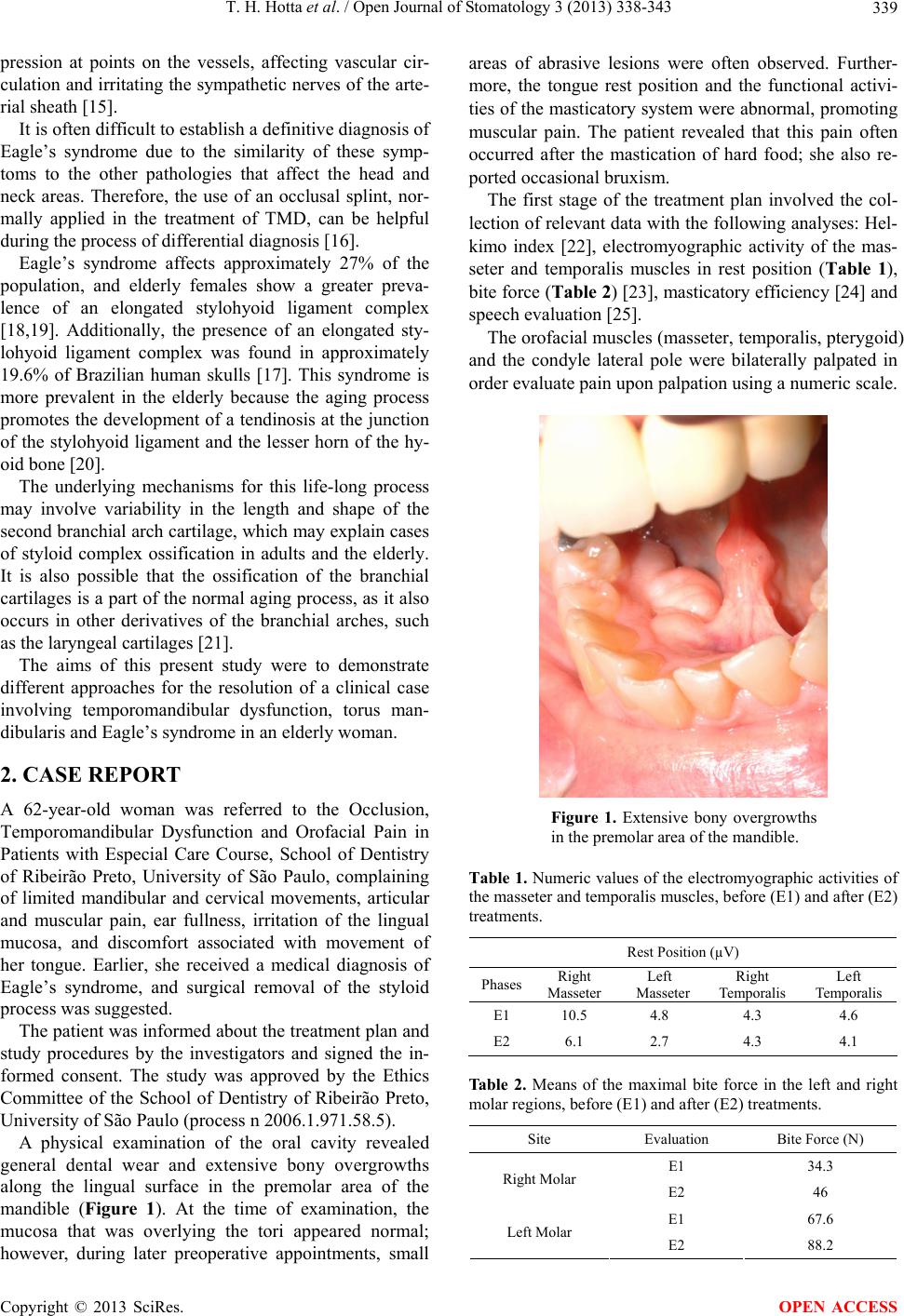 T. H. Hotta et al. / Open Journal of Stomatology 3 (2013) 338-343 339 pression at points on the vessels, affecting vascular cir- culation and irritating the sympathetic nerves of the arte- rial sheath [15]. It is often difficult to establish a definitive diagnosis of Eagle’s syndrome due to the similarity of these symp- toms to the other pathologies that affect the head and neck areas. Therefore, the use of an occlusal splint, nor- mally applied in the treatment of TMD, can be helpful during the process of differential diagnosis [16]. Eagle’s syndrome affects approximately 27% of the population, and elderly females show a greater preva- lence of an elongated stylohyoid ligament complex [18,19]. Additionally, the presence of an elongated sty- lohyoid ligament complex was found in approximately 19.6% of Brazilian human skulls [17]. This syndrome is more prevalent in the elderly because the aging process promotes the development of a tendinosis at the junction of the stylohyoid ligament and the lesser horn of the hy- oid bone [20]. The underlying mechanisms for this life-long process may involve variability in the length and shape of the second branchial arch cartilage, which may explain cases of styloid complex ossification in adults and the elderly. It is also possible that the ossification of the branchial cartilages is a part of the normal aging process, as it also occurs in other derivatives of the branchial arches, such as the laryngeal cartilages [21]. The aims of this present study were to demonstrate different approaches for the resolution of a clinical case involving temporomandibular dysfunction, torus man- dibularis and Eagle’s syndrome in an elderly woman. 2. CASE REPORT A 62-year-old woman was referred to the Occlusion, Temporomandibular Dysfunction and Orofacial Pain in Patients with Especial Care Course, School of Dentistry of Ribeirão Preto, University of São Paulo, complaining of limited mandibular and cervical movements, articular and muscular pain, ear fullness, irritation of the lingual mucosa, and discomfort associated with movement of her tongue. Earlier, she received a medical diagnosis of Eagle’s syndrome, and surgical removal of the styloid process was suggested. The patient was informed about the treatment plan and study procedures by the investigators and signed the in- formed consent. The study was approved by the Ethics Committee of the School of Dentistry of Ribeirão Preto, University of São Paulo (process n 2006.1.971.58.5). A physical examination of the oral cavity revealed general dental wear and extensive bony overgrowths along the lingual surface in the premolar area of the mandible (Figure 1). At the time of examination, the mucosa that was overlying the tori appeared normal; however, during later preoperative appointments, small areas of abrasive lesions were often observed. Further- more, the tongue rest position and the functional activi- ties of the masticatory system were abnormal, promoting muscular pain. The patient revealed that this pain often occurred after the mastication of hard food; she also re- ported occasional bruxism. The first stage of the treatment plan involved the col- lection of relevant data with the following analyses: Hel- kimo index [22], electromyographic activity of the mas- seter and temporalis muscles in rest position (Table 1), bite force (Ta ble 2 ) [23], masticatory efficiency [24] and speech evaluation [25]. The orofacial muscles (masseter, temporalis, pterygoid) and the condyle lateral pole were bilaterally palpated in order evaluate pain upon palpation using a numeric scale. Figure 1. Extensive bony overgrowths in the premolar area of the mandible. Table 1. Numeric values of the electromyographic activities of the masseter and temporalis muscles, before (E1) and after (E2) treatments. Rest Position (µV) Phases Right Masseter Left Masseter Right Temporalis Left Temporalis E1 10.5 4.8 4.3 4.6 E2 6.1 2.7 4.3 4.1 Ta b l e 2 . Means of the maximal bite force in the left and right molar regions, before (E1) and after (E2) treatments. Site Evaluation Bite Force (N) E1 34.3 Right Molar E2 46 E1 67.6 Left Molar E2 88.2 Copyright © 2013 SciRes. OPEN ACCESS  T. H. Hotta et al. / Open Journal of Stomatology 3 (2013) 338-343 340 This scale consisted of 11 points, beginning with “0” (no pain) and ending in “10” (the worst imaginable pain) [26] (Table 3). Using the Hugoson Index [27], the observed occlusal wear was classified as level 1 (attrition of enamel down to dentin spots), confirming the presence of bruxism that was reported earlier by the patient. Maximum mouth opening and the right and left lateral movements were measured with a millimeter ruler. To measure the maximum mouth opening movement, the patient was requested to open her mouth, and the dis- tance between the incisal borders was measured. The patient performed right and left lateral movements, and the distance between the mandibular and maxillary mid- lines was measured. As there was no coincidence, a pen- cil mark was made on the surface of the maxillary incisor, corresponding to the mandibular midline, and a meas- urement was later taken. The protrusion distance be- tween the maxillary and mandibular incisal borders was measured with a ruler (Table 4). The patient’s masticatory efficiency was determined using a coconut and sieve system, before and after treat- ment. The patient received four aliquots of coconut pieces, weighing a total of 20 g. Each piece of food was chewed for 50 cycles. After mastication, the chewed par- ticles were expelled into a set of five sieves (5, 4, 3, 2 and 1 mm) and were washed with water. Then, the parti- cles were separated according to the granulometric mesh particles contained in each sieve, and these particles were put inside test tubes (A, B, C, D and E), according their sizes. The test tubes were centrifuged for 5 minutes, and the volumetric data were inserted in a mathematical for- mula (4A + 2B + C/D + E) to obtain the index of masti- cation (>10 = optimal, 5.0 to 9.9 = good, 2.0 to 4.9 = regular, 1.0 to 1.9 = bad, <1.0 = terrible) (Table 5). Afterward, the TMs were completely removed under local anesthesia. The inferior alveolar nerves were Table 3. Intensity of muscular and articular pain, before (E1) and after (E2) treatments. Masseter Temporalis Lateral Pterygoid Condyle Lateral Pole Right Left Right Left Right Left RightLeft E1 7 5 8 3 8 7 8 2 E2 7 2 2 0 3 0 5 0 Table 4. Numeric values of the measurements of mandibular movements, before (E1) and after (E2) treatments. Mandibular Movements (mm) Mouth Opening Right Laterality Left Laterality Protrusion E1 29 5 4 2 E2 50 8 9 3 blocked with 1.8 ml of anesthetic solution containing mepivacaine (2 percent) and epinephrine (1:100.000), applied to each side. The surgical approach consisted of an intrasulcular incision that extended from one first molar to the other. Afterward, a full-thickness flap was carefully elevated, exposing both TMs and preserving the insertion of the genioglossus muscles. The delimita- tion of the TMs was performed using a surgical length #702 taper fissure crosscut carbide bur. Afterward, a thin, straight chisel was positioned into the gap and lightly hammered twice, resulting in the easy removal of the TMs. The bone irregularities were removed with a man- ual Seldin bone file #12 to obtain a smooth surface along the lingual cortical. The surgical field was copiously ir- rigated with sterile saline solution, and the wound was sutured in a non-continuous fashion with 4 - 0 black silk thread mounted in a 1.7 cm - 12 circle needle (Ethicon, São Paulo, Brazil). The biopsied tissues were sent to the Department of Morphology, Stomatology and Physiol- ogy for histopathological analysis, which confirmed the diagnosis of TM. The patient was medicated with sodic diclofenac (50 mg every 8 hours for 3 days) and dipiron (500 mg every 8 hours, to prevent pain). The postopera- tive period was uneventful, and the final result was a success. After 2 months, an acrylic splint with anterior guid- ance for disocclusion in protrusion and canine guidance for disocclusion in lateral movements was provided to the patient, who wore it for 6 weeks and was submitted to weekly follow-up. 3. RESULTS The patient exhibited intense signs and symptoms of dysfunctions, such as limited jaw opening, pain during mandibular movements, and pain during articular and muscular palpation. She received an Acute Physiology and Chronic Health Evaluation III score (AIII) for an- amnestic dysfunction and, after treatment, for minor signs and symptoms of dysfunction, such as TMJ noises, fatigue of masticatory muscles and TMJ stiffness. The data collected on the evaluation of mandibular movements, functional evaluation of the TMJ, pain dur- ing mandible movements, muscular pain and articular pain accurately demonstrated the degree of TMJ dys- function, both before (DiIII—severe clinical symptoms Table 5. Numeric values of the volumetric data and mastica- tory index, before (E1) and after (E2) treatments. Masticatory Efficiency Sieve A Sieve B Sieve C Sieve D Sieve E Results Index E12 4 10 10 4 1.85 bad E23 6 10 5 1 5.66 good Copyright © 2013 SciRes. OPEN ACCESS  T. H. Hotta et al. / Open Journal of Stomatology 3 (2013) 338-343 341 of dysfunction) and after (DiII—moderate clinical symp- toms of dysfunction) treatments. 4. DISCUSSION Orofacial pain, joint noise and limited mandibular move- ments are symptoms commonly associated with TMD. Other symptoms, such as headache, earache, neck pain, tinnitus and dysphagia are also related to this disorder [28-30]. Similar signs and symptoms may be found in other diseases, such as Eagle’s syndrome, and it may be difficult to establish the correct diagnosis and appro- priate treatment [10,31]. To facilitate diagnosis, the patient should be submitted to a group of professionals from diverse disciplines, to provide a comprehensive assessment and consultation in cases that present several signs and symptoms, such as the case reported here. The first stage of the treatment plan involved the col- lection of data that allowed a global view of the patient’s clinical and functional conditions. The sequence of pro- cedures was then selected. The surgical treatment for Eagle’s syndrome involves the excision of the stylohyoid process [10,12]. However, such treatment involves the possibility of associating pathologies that may aggravate the symptoms. Therefore, a conservative, nonsurgical approach with an occlusal splint is often. Dentists should be aware of the risks of surgical inter- vention to provide a better diagnosis and therapeutic pro- cedure [32]. Because the occurrence of bilateral TM can interfere with masticatory and speech functions in dentate patients, affecting their quality of life, the clinicians in this case chose to apply surgical intervention. The favorable cli- nical results (tongue rest position and functional active- ties) confirmed the appropriateness of this choice. The ability to grind food is the end product of chewing, and several structures of the stomatognathic system work together so that chewing can be satisfactorily performed. To evaluate the masticatory function, which encom- passes the efficiency of the masticatory muscles and mas- ticatory performance, the maximum bite force is useful in both demonstrating how the system is fully interfaced and in revealing any anatomical changes and temporo- mandibular disorders that lead to an imbalance of this system [33]. After treatment, the patient’s masticatory efficiency improved. The activity began to be pleasant, without joint or muscular pain and without trauma to the area that previously accommodated the mandibular tori. The pa- tient could also chew food harder and faster. Occlusal splint therapy was applied to treat the pa- tient’s TMD and to assist the group of professionals dur- ing the differential diagnosis process, as previously sug- gested [16]. The satisfactory clinical outcomes were evi- denced in the increased amplitude of mandibular move- ments, decrease in muscular/articular pain and the im- provement in functional activities. The patient was instructed to chew pieces of test food as usual, and it was observed that chewing was per- formed on the left, with greater bite force on the left side. The right side exhibited greater muscle and joint pain, justifying the patient’s preference for chewing on the left side. It should be noted that the magnitude of the bite force varies when characteristics of the craniofacial com- plex are abnormal, especially in cases of temporoman- dibular dysfunction [34]. Electromyographical analysis of the masseter and tem- poralis muscles may be used to compare muscular activi- ties during rest and during clinical manipulation [18]. The results of electromyographic analyses showed that mean muscle activity was improved after the combina- tion of surgical therapy and the occlusal splint. This article reports a clinical case in which a combina- tion of surgical therapy and dental resources were used to treat limited mandibular movements and painful symp- toms in a patient with temporomandibular dysfunction, Eagle’s syndrome and torus mandibularis. In recent decades, the required care for older people has increased in the daily practice of dental professionals. Therefore, it is critical for clinicians to understand the situations that lead to discomfort in older patients. 5. CONCLUSION In summary, dental practitioners should understand the causes of anatomical changes, improving their patients’ quality of life by providing a more practical approach to the treatment of painful sintomatoligia in older people with Eagle’s syndrome, temporomandibular disorder and mandibular tori. 6. ACKNOWLEDGEMENTS The authors wish to thank Ribeirão Preto School of Dentistry, Univer- sity of São Paulo. REFERENCES [1] Antoniades, D.Z., Belazi, M. and Panayiotis, P. (1998) Concurrence of torus palatinus with palatal and buccal exostoses-Case report and review of the literature. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 85, 552-557. http://dx.doi.org/10.1016/S1079-2104(98)90290-6 [2] Hassan, K.S., Alagl, A.S. and Abdel-Hady, A. (2012) Torus mandibularis bone chips combined with platelet rich plasma gel for treatment of intrabony osseous defects: Clinical and radiographic evaluation. International Jour- nal of Oral and Maxillofacial Surgery, 41, 1519-1526. Copyright © 2013 SciRes. OPEN ACCESS  T. H. Hotta et al. / Open Journal of Stomatology 3 (2013) 338-343 342 http://dx.doi.org/10.1016/j.ijom.2012.02.009 [3] Al-Bayaty, H.F., Murti, P.R., Matthews, R. and Gupta, P.C. (2001) An epidemiological study of tori among 667 dental outpatients in Trinidad & Tobago, West Indies. Inte national Journal of Dentistry, 51, 300-304. http://dx.doi.org/10.1002/j.1875-595X.2001.tb00842.x [4] Raldi, F.V., Nascimento, R.D., Sá-Lima, J.R., Tsuda, C.A. and Moraes, M.B. (2008) Excision of an atypical case of palatal bone exostosis: A case report. Journal of Oral Science, 50, 229-331. http://dx.doi.org/10.2334/josnusd.50.229 [5] Matheus, R.A., Ramos-Perez, F.M., Menezes, A.V., Am- brosano, G.M., Haiter-Neto, F., Bóscolo, F.N. and de Almeida, S.M. (2009) The relationship between tem- poromandibular dysfunction and head and cervical pos- ture. Journal of Applied Oral Science, 17, 204-208. http://dx.doi.org/10.1590/S1678-77572009000300014 [6] Eggen, S. and Natvig, B. (1991) Variation in torus man- dibularis prevalence in Norway: a-statistical analysis us- ing logistic regression. Community Dentistry Oral Epi- demiology, 19, 32-35. http://dx.doi.org/10.1111/j.1600-0528.1991.tb00101.x [7] Haugen, L.K. (1992) Palatine and mandibular tori. A morphologic study in the current Norwegian population. Acta Odontologica Scandinavica, 50, 65-77. http://dx.doi.org/10.3109/00016359209012748 [8] Kerdporn, D. and Sirirungrojying, S. (1999) A clinical study of oral tori in southern Thailand: Prevalence and the relation to parafunctional activity. European Journal of Oral Sciences, 107, 9-13. http://dx.doi.org/10.1046/j.0909-8836.1999.eos107103.x [9] Sirirungrojying, S. and Kerdpon, D. (1999) Relationship between oral tori and temporomandibular disorders. In- ternational Dental Journal, 49, 101-104. http://dx.doi.org/10.1111/j.1875-595X.1999.tb00516.x [10] Souza, E.A., Hotta, T.H. and Bataglion, C. (1996) Asso- ciation of a temporomandibular disorder and Eagle’s syn- drome: Case report. Brazilian Dental Journal, 7, 53-58. [11] Grossmann, E. and Paiano, G.A. (1998) Eagle’s syn- drome: A case report. The Journal of Craniomandibular Practice, 16, 126-130. http://dx.doi.org/10.5505/agri.2013.26779 [12] Ferreira de Albuquerque, R. Jr., Müller, K., Hotta, T.H. and Gonçalves, M. (2003) Temporomandibular disorder or Eagle’s syndrome? A clinical report. Journal of Pros- thetic Dentistry, 90, 317-320. http://dx.doi.org/10.1016/S0022-3913(03)00522-5 [13] Shankland, W.E. (2010) Anterior throat pain syndromes: Causes for undiagnosed craniofacial pain. The Journal of Craniomandibular Practice, 28, 50-59. [14] Fusco, D.J., Asteraki, S. and Spetzler, R.F. (2012) Ea- gle’s syndrome: Embryology, anatomy, and clinical ma- nagement. Acta Neurochirurgica, 154, 1119-1126. http://dx.doi.org/10.1007/s00701-012-1385-2 [15] Eagle, W.W. and Durham, N.C. (1949) Symptomatic elongated styloid process. Archives of Otolaryngology, 49, 490-503. http://dx.doi.org/10.1001/archotol.1949.03760110046003 [16] Hotta, T.H., Vicente, M.F., dos Reis, A.C., Bezzon, O.L., Bataglion, C. and Bataglion, A. (2003) Combination the- rapies in the treatment of temporomandibular disorders: A clinical report. Journal of Prosthetic Dentistry, 89, 536-539. [17] Leite, H.F., Niccoli Filho, W.D., Liberti, E.A., Madeira, M.C. and Simões, S. (1998) Prevalence of elongated sty- lohyoid ligament complex in human skulls. Revista Odontologica UNESP, 17, 145-151. [18] Rizzatti-Barbosa, C.M., Ribeir, M.C., Silva-Concilio, L.R., Di Hipolito, O., Ambrosano GM. (2005) Is an elon- gated stylohyoid process prevalent in the elderly? A ra- diographic study in a Brazilian population. Gerodon- tology, 22, 112-115. http://dx.doi.org/10.1111/j.1741-2358.2005.00046.x [19] Breault, M.R. (1986) Eagle’s syndrome: Review of the literature and implications in craniomandibular disorders. The Journal of Craniomandibular Practice, 4, 323-337. [20] Camarda, A.J., Deschamps, C. and Forest, D. (1989) Stylohyoid chain ossification: A discussion of etiology. Oral Surgery Oral Medicine Oral Pathology, 67, 508-514. http://dx.doi.org/10.1016/0030-4220(89)90264-8 [21] Krmpotić Nemanić, J., Vinter, I., Ehrenfreund, T. and Marusić, A. (2009) Postnatal changes in the styloid proc- ess, vagina processus styloidei, and stylomastoid foramen in relation to the function of muscles originating from the styloid process. Surgical and Radiologic Anatomy, 31, 343-348. http://dx.doi.org/10.1007/s00276-008-0450-2 [22] Helkimo, M. (1974) Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Svensk Tand- lakare Tidskrift, 67, 101-121. [23] Hotta, P.T., Hotta, T.H., Bataglion, C., Bataglion, S.A., de Souza Coronatto, E.A., Siéssere, S. and Regalo, S.C.H. (2010) Emg analysis after laser acupuncture in patients with temporomandibular dysfunction (TMD)-Implica- tions for practice. Complementary Therapies Clinical Practice, 16,158-160. http://dx.doi.org/10.1016/j.ctcp.2010.01.002 [24] Bajoria, A.A., Saldanha, S. and Shenoy, V.K. (2012) Evaluation of satisfaction with masticatory efficiency of new conventional complete dentures in edentulous pa- tients—A survey. Gerodontology, 29, 231-238. http://dx.doi.org/10.1111/j.1741-2358.2012.00634.x [25] de Felício, C.M., Mazzetto, M.O., de Silva, M.A., Ba- taglion, C. and Hotta, T.H. (2006) A preliminary protocol for multi-professional centers for the determination of signs and symptoms of temporomandibular disorders. The Journal of Craniomandibular Practice, 24, 258-264. [26] Downie, W.W., Leatham, P.A., Rhind, V.M., Wright, V., Branco, J.A. and Anderson, J.A. (1978) Studies with pain rating scales. Annals of the Rheumatic Diseases, 37, 378- 381. http://dx.doi.org/10.1136/ard.37.4.378 [27] Hugoson, A., Bergendal, T., Ekfeldt, A. and Helkimo, M. (1998) Prevalence and severity of incisal and occlusal tooth wear in an adult Swedish population. Acta Odon- tologica Scandinavica, 46, 255-265. http://dx.doi.org/10.3109/00016358809004775 Copyright © 2013 SciRes. OPEN ACCESS  T. H. Hotta et al. / Open Journal of Stomatology 3 (2013) 338-343 Copyright © 2013 SciRes. 343 OPEN ACCESS [28] Baba, K., Tsukiyama, Y., Yamazaki, M. and Clark, G.T. (2001) A review of temporomandibular disorder diagnos- tic techniques. Journal of Prosthetic Dentistry, 86, 184- 194. http://dx.doi.org/10.1067/mpr.2001.116231 [29] dos Reis, A.C., Hotta, T.H., Ferreira-Jeronymo, R.R., de Felício, C.M. and Ribeiro, R.F. (2000) Ear symptoma- tology and occlusal factors: A clinical report. Journal of Prosthetic Dentistry, 83, 21-24. http://dx.doi.org/10.1016/S0022-3913(00)70084-9 [30] Restrepo, C.C., Medina, I. and Patiño, I. (2011) Effect of Occlusal Splints on the Temporomandibular Disorders, Dental Wear and Anxiety of Bruxist Children. Eurean Journal of Dentistry, 5, 441-450. [31] Jain, D., Chauhan, J.S, Jain, S. and Goel, G. (2011) Elon- gated styloid process: An unusual cause of neck pain and difficulty in swallowing. Journal of Orofacial Pain, 25, 269-271. [32] Valerio, C.S., Peyneau, P.D., de Sousa, A.C., Cardoso, F.O., de Oliveira, D.R. and Taitson, P.F. (2012) Stylohy- oid syndrome: Surgical approach. Journal of Craniofacial Surgery, 23, e138-140. http://dx.doi.org/10.1097/SCS.0b013e31824cdb46 [33] Borges Tde, F., Regalo, S.C., Taba, M. Jr., Siéssere, S., Mestriner, W. Jr. and Semprini, M. (2013) Changes in masticatory performance and quality of life in individuals with chronic periodontitis. Journal of Periodontology, 84, 325-331. http://dx.doi.org/10.1902/jop.2012.120069 [34] Bonjardim, L.R., Gavião, M.B., Pereira, L.J. and Castelo, P.M. (2005) Bite force determination in adolescents with and without temporomandibular dysfunction. Journal of Oral Rehabilitation, 32, 577-583. http://dx.doi.org/10.1111/j.1365-2842.2005.01465.x
|