Y. Jang, H. Yoo / Open Journal of Nursing 3 (2013) 420-425
424
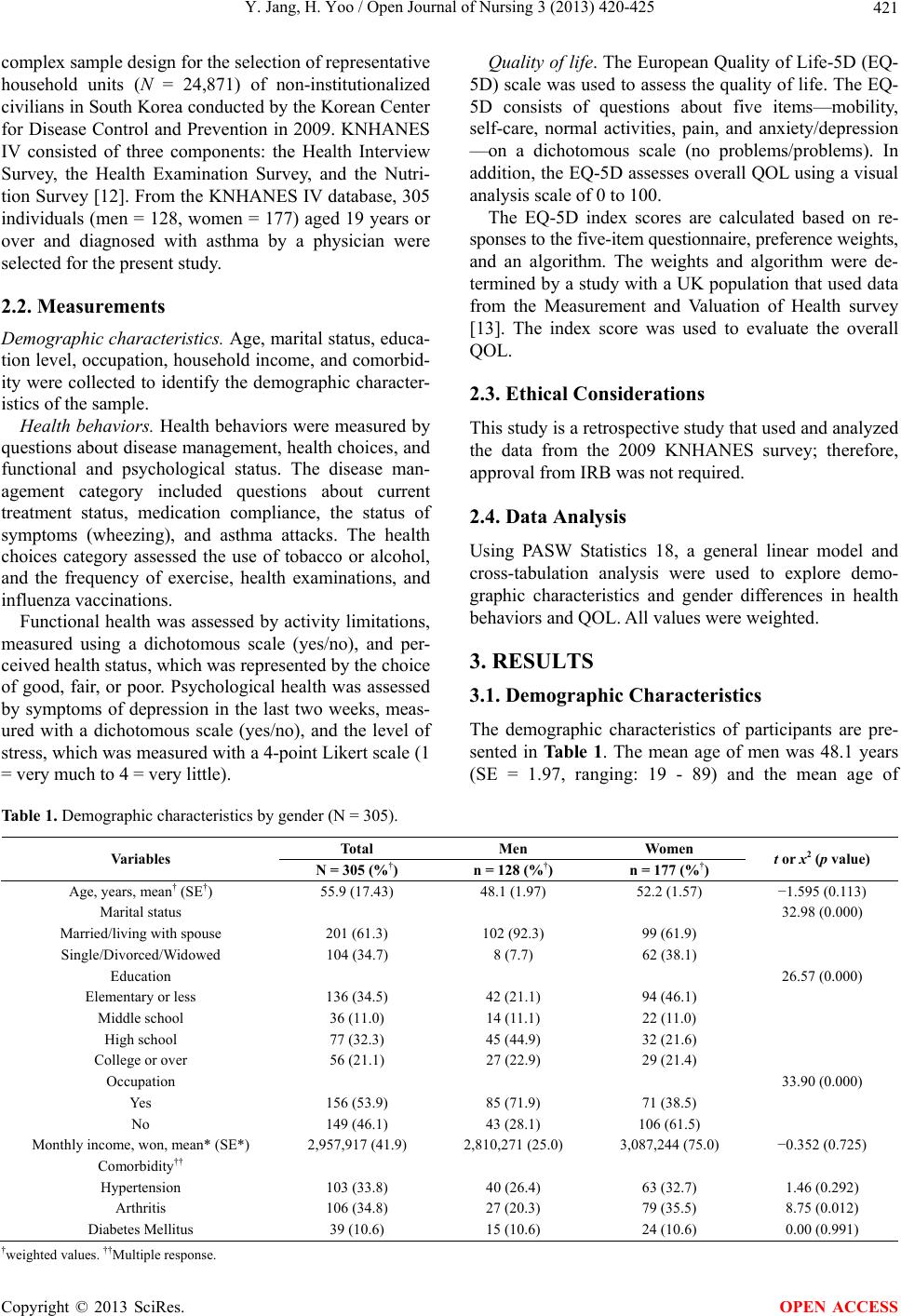
in disease management, health behaviors, and QOL in
Koreans with asthma. The mean age at diagnosis among
men was significantly lower than that of women in this
study. This result is consistent with previous studies
[14,15], which reported that the incidence of asthma
among women 35 years or older was increasing, and that
the number of women with asthma was higher than that
of men in individuals over 40 years of age [14]. The age
at diagnosis of asthma seems to differ by gender.
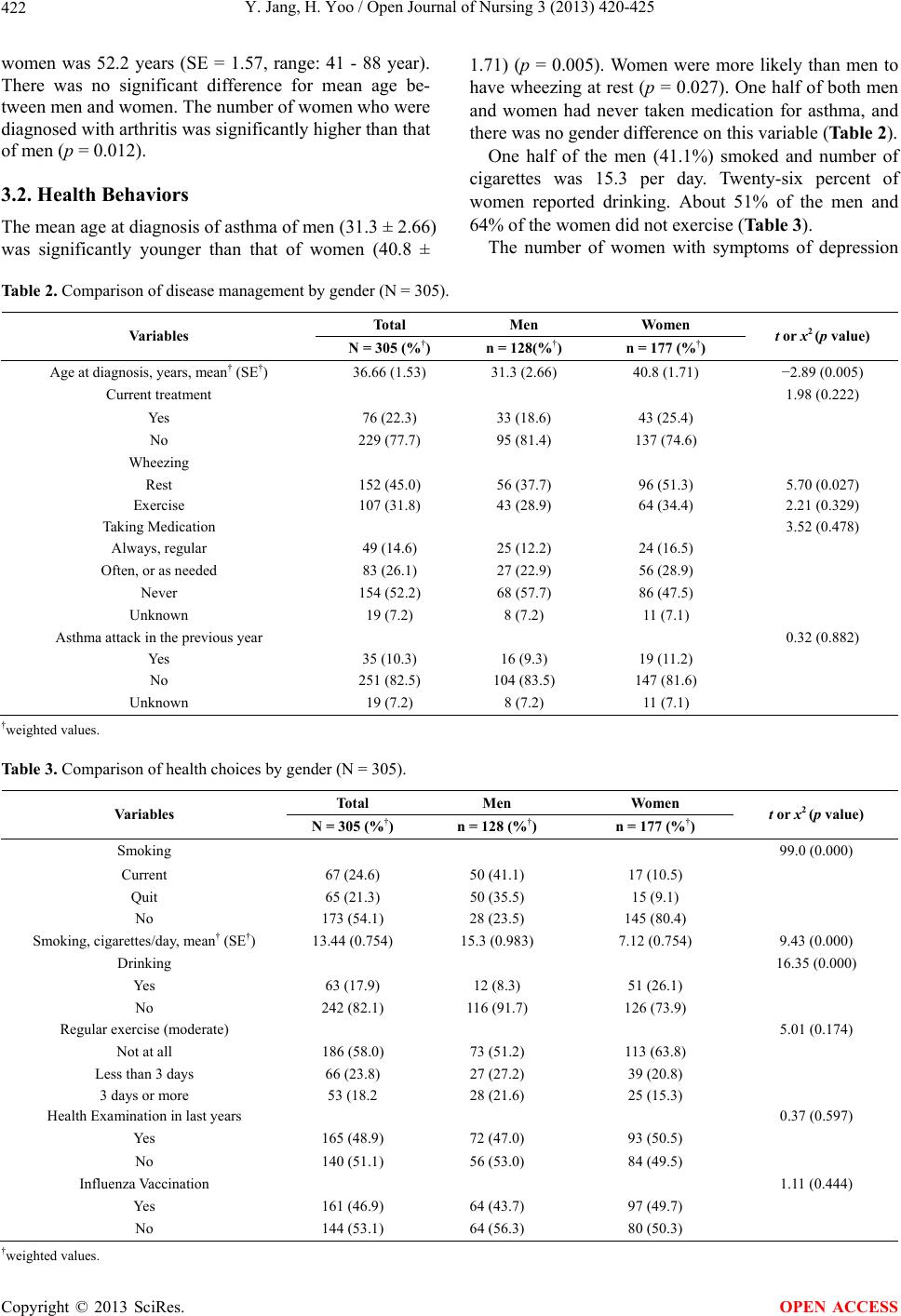
Both men and women had poor health behaviors in
this study, and there were gender differences in asthma
symptoms. Manfreda and his colleges [16] reported that
women experienced more symptoms, such as dyspnea
and wheezing, than men; therefore, women received
more medical treatments. In this study, more women also
reported wheezing at rest than men. However, although
51% women reported wheezing at rest, only 25% of this
sample received asthma treatments. Adherence to asthma
medication schedules was moderate for both men and
women and there were no significant gender differences.
Therefore, effective interventions to improve self-man-
agement of their disease should be developed for Kore-
ans with asthma.
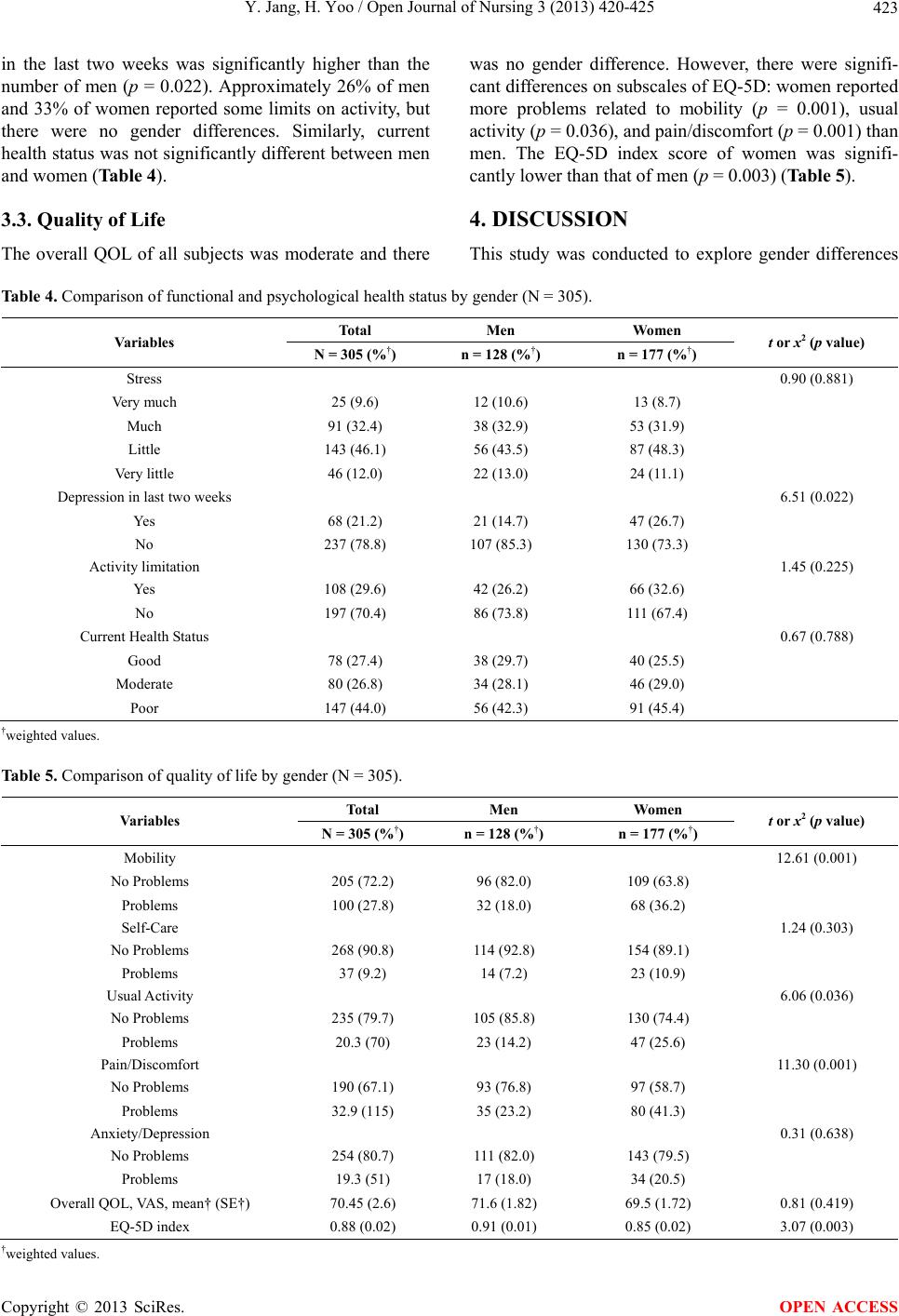
In psychological health status, the rate of women with
depression was significantly higher than that of men.
This result is consistent with the results of a previous
study that found women with mild asthma had more
episodes of anxiety and depression than men [17]. In
addition, Koreans women with asthma might be likely to
be more depressed than overall Korean populations even
though we did not compare depression between Korean
women with asthma and without asthma in this study.
However, Sung [18] reported that 13% of participants
were depressed in last two weeks and 3% of them were
diagnosed depression generally using national data,
while about 27% of women with asthma reported de-
pression in this sample. Interventions focusing on psy-
chological issues may need to be tailored more toward
women.
The overall QOL of this sample was moderate and a
gender difference was not observed. However, the EQ-
5D index score of women was significantly lower than
the score of men. The EQ-5D index scores of the par-
ticipants was lower than the scores of overall Koreans
aged 19 years or over and Koreans with osteoarthritis
and hypertension [19], and was similar to the scores of
Koreans with cancer and chronic obstructive pulmonary
disease [6]. The results of prior QOL studies are similar
to the results of this study; in those studies, the overall
QOL of patients with asthma was low, and women had a
lower QOL than men [10,20,21].
In the subscales of the EQ-5D, the number of women
reporting problems with mobility, usual activities, and
pain/discomfort was significantly higher than the number
of men. More women than men also reported problems
on the subscales of self-care and anxiety/depression,
even though there were no significant gender differences.
Sinclaire and Tolsma [21] found that women with asthma
were more likely to complain of discomfort, symptoms
of wheezing, and shortness of breath, which supports the
results of this study. Therefore, women with asthma
might need different symptom management and health
behavior strategies than men. Health care providers
should evaluate and address health status by gender for
individuals with asthma.
The study has some limitations. First, there is sam-
pling bias due to the use of the self-report instruments in
the KNHANES IV. Some of the information was subjec-
tive and might differ from a professional evaluation.
Second, the KNHANES IV used the EQ-5D to evaluate
QOL, which is useful when comparing QOL among peo-
ple with varying diseases and countries, but this instru-
ment lacks sensitivity in the assessment of specific issues
affecting people with asthma. Third, we did not compare
health status and health behaviors between Koreans with
asthma and without asthma. Because the differences s of
sample sizes between them was big, there was the lack of
statistical stability. Further study needs to examine the
difference between people with asthma and without asthma.
5. CONCLUSION
Although there are some limitations, this study found
gender differences in disease management, health status,
and QOL of Koreans with asthma. Women with asthma
were more likely to have psychological problems and
discomfort related to asthma symptoms than men. The
findings of this study are important for the development
of effective and gender-sensitive interventions aimed at
enhancing health status and QOL among patients with
asthma.
REFERENCES
[1] World Health Organization (2011) Asthma. 2011
http://www.who.int/respiratory/asthma/en/
[2] Center for Disease Control and Prevention (2011).
Asthma fast facts.
http://www.cdc.gov/asthma/pdfs/asthma_fast_facts_statis
tics.pdf
[3] Korea Ministry for Health Welfare and Family Affairs
(2011) Status of Chronic Disease in Korea. 2011
http://www.index.go.kr/egams/stts/jsp/potal/stts/PO_STT
S_IdxMain.jsp?idx_cd=1438&bbs=INDX_001
[4] Strine, T.W., et al. (2008) Impact of depression and anxi-
ety on quality of life, health behaviors, and asthma con-
trol among adults in the United States with asthma, 2006.
Journal of Asthma, 45, 123-133.
http://dx.doi.org/10.1080/02770900701840238
Copyright © 2013 SciRes. OPEN ACCESS