 World Journal of Cardiovascular Diseases, 2013, 3, 433-441 WJCD http://dx.doi.org/10.4236/wjcd.2013.37068 Published Online October 2013 (http://www.scirp.org/journal/wjcd/) The implication of calcium score and pentraxin-3 in non-invasive identification of significant coron ary artery stenosis in chronic stable angina pectoris Habib Haybar1, Mohammad Davoodi2, Abtin Shahlaee3, Amir Eslami Shahr Babaki4*, Zahra Fazelinezhad2, Maryam Azarian5, Molook Salemzadeh6 1Cardiovascular Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran 2Radiology Group, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran 3Scientific Research Center, Tehran University of Medical Sciences, Tehran, Iran 4Sports Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran 5Biology Group, North Tehran Branch, Islamic Azad University, Tehran, Iran 6Golestan Hospital Clinical Research Development Unit, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran Email: *Takamoolsk@yahoo.com Received 22 July 2013; revised 25 August 2013; accepted 9 September 2013 Copyright © 2013 Habib Haybar et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Objective: Coronary Artery Disease (CAD) would continue to concern medical society in the foreseeable future. Determining the extent of coronary luminal stenosis is a key factor in management of CAD. Methods presently used are costly and pose certain dangers, ranging from nephrotoxicity to death. Long Pentraxin or Pentraxin-3 (PTX3) has been used to predict survival or atherosclerotic process, but not to identify coronary stenosis. Calcium Score has been used to this end with some success. Methods: Indi- viduals with chronic stable angina, without evidence of Myocardial Infarction (MI), who were categorized as intermediate-risk after completing a treadmill ex- ercise test, according to Duke Protocol, underwent cardiac catheterization. In addition, blood samples were drawn for coronary sinus PTX3, and also PTX3, uric acid, high-sensitivity C-reactive protein (hs- CRP), cholesterol, glucose and High-Density Lipo- protein (HDL) in peripheral circulation. Calcium Scores were calculated using Agatston Score and non- contrast multi-slice CT scan. Participants were di- vided according to the number of stenotic coronary arteries (patent, one-, two- and three-vessel disease). Results: We found that PTX3 levels in coronary sinus and femoral vein correlated with each other, after log-transforming the values. Also we found that PTX3 levels and Calcium Scores differed among in- dividuals with triple-vessel involvement and indi- viduals without significant stenosis in any of coronary arteries. No significant differences were observed, regarding hs-CRP levels. Conclusion: PTX3 levels in periphery correlate with those in coronary arteries, and this variable can be measured with a less invasive procedure. In addition to Calcium Score, PTX3 levels are different in our four groups. The combined con- tribution of PTX3 and calcium score may help us identify individuals with significant coronary artery stenosis without needing to perform cardiac cathe- terization in a select group of patient s. Keywords: Coronary Artery Disease; Calcium Score; Pentraxin-3; Long Pentraxin; hs-CRP; Non-Invasive 1. INTRODUCTION Coronary Artery Disease (CAD) is a leading cause of mortality worldwide [1]. Atherosclerosis of coronary ar- teries is by far the main etiology of Ischemic Heart Dis- ease (IHD) and plaque disruption superimposed by thrombosis is the major cause of Acute Coronary Syn- dromes (ACS) including Unstable Angina (UA) and Myocardial Infarction (MI) and sudden death [2,3]. Nearly half of IHD cases are initially manifested by the process of atherosclerosis in the absence of thrombosis, which is generally a benign condition and usually pre- sents itself as chronic stable angina. Chronic stable an- gina has a financial burden of reaching tens of billions of US dollars [4]. Duke treadmill score is a scoring system employed in conjunction with a standard exercise treadmill test to *Corresponding author. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 434 determine the prognosis of chronic stable angina when the diagnosis is uncertain [4]. In addition to helping quantify ischemia severity [5], Duke Score enables us to postpone cardiac catheterization in patients classified as low-risk. Nevertheless in intermediate-risk patients, at- tempts to quantify ischemia severity may prove incon- clusive [6]. Since patients in the intermediate-risk group are usually referred for cardiac catheterization, which is costly, needs expertise and is potentially hazardous, a search is going on to find newer methods and prediction models, with respect to coronary artery involvement [6-10]. Furthermore, considering that traditional models for atherosclerosis risk-stratification mainly determine the long-term risk of cardiac events, there is a trend to- wards biomarkers and their use for assessing short-term risk of cardiovascular events [11]. The significance of C-reactive protein (CRP) and high-sensitivity CRP (hs-CRP) and their implications in CAD remains controversial, some studies implying their levels as predictors of cardiac risk, and some indicating the contrary [8,12-14]. Pentraxin-3 (PTX-3), initially proposed as an early in- dicator of innate immunity and inflammatory response, is also expressed abundantly in cardiac tissue during in- flammatory processes, in the atherosclerotic lesions, in circulation in patients affected by arterial inflammation, especially those suffering from unstable angina. In- creased expression has also been observed in vitro from endothelial cells in response to inflammatory agents [15-17]. PTX-3 is thought to be released specifically in vascular insults, so it seems reasonable to assume that measuring its level would provide us with a more reliable assessment of the course and progression of the athero- sclerotic processes and corresponding lesions than more conventional and non-specific inflammatory markers like CRP. Furthermore, newly published work of Turkish car- diologists suggests that PTX-3 is more tightly associated with the complexity and severity of CAD than hs-CRP [18]. In a study on prognostic significance of long Pen- traxin in MI, this biomarker was shown to enable predic- tion of 3-month mortality probability after accounting for other factors [19]. Yet the association of PTX-3 with cardiovascular dis- eases as an entity, its associated risk factors, its incidence or its other associated conditions like the subclinical forms of cardiovascular disease has not been fully inves- tigated [20]. Furthermore, different studies suggest that PTX-3 acts rather locally, therefore, its levels in coro- nary vessels are related to cardiovascular disorders, in general. But obtaining blood samples from coronary vessels is nothing short of performing cardiac catheteri- zation. As a result, we sought to determine the relation- ship between PTX-3 levels in coronary sinus and periph- eral venous blood. Calcification of atherosclerotic lesions starts early as plaque formation in human body, albeit in small quanti- ties, but more advanced lesions are more commonly cal- cified [10]. Various methods for evaluating and quanti- fying this aspect of atherosclerotic process have been used. Spiral CT scanning has a reasonable (91% sensi- tiveity and 52% specificity compared with angiography, when looking for calcification) statistical and financial balanced utility [10]. However, it is still suggested to be used in conjunction to other more “traditionally” ac- cepted criteria [20]. To sum up, chronic stable angina affects a relatively large and growing population with a tremendous associ- ated cost which is going to increase in developing coun- tries. Risk assessment is somewhat problematic in a ma- jor group of these patients, the intermediate-risk group. We therefore evaluated the role of inflammation markers, specifically of pentraxin-3, hs-CRP and calcium score in patients with intermediate risk unstable angina who un- derwent coronary angiography to determine if there is a direct relationship between severity of CAD by an- giographic criteria and these parameters in this specific population. 2. METHODS 2.1. Overview The study is an observational study on patients with symptoms suggestive of chronic stable angina. Our main goal was to determine a reliable guide to help decide which intermediate-risk patients, classified in this risk stratum by Duke score, should undergo more invasive and costly procedures, most importantly cardiac cathe- terization. Participants underwent sampling from femoral vein, an interview for collecting demographic data and other relevant medical history, and cardiac catheterize- tion during the initial visit. The hypothesis tested was that a combination of laboratory data including serum level of inflammatory markers and certain imaging mo- dalities, which in our study is Multi-slice Computed Tomography (CT) scanning of heart to determine coro- nary Calcium Score, is superior to more traditional measures of risk determination like Duke scoring, espe- cially in those categorized as intermediate-risk cases. 2.2. Participants The study population consisted of fifty one females and forty nine males selected from patients who were seeking care from the Imam Khomeini Cardiology Clinic, in Ahvaz, Iran. The patients presented with symptoms sug- gesting chronic stable angina. All participants were clas- sified by Duke Score as intermediate-risk upon complet- ing a treadmill exercise test. None of the patients had an Electrocardiogram (ECG) diagnostic for MI, a history of Copyright © 2013 SciRes. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 435 MI or laboratory findings of MI, that is elevated levels of serum Creatinine Phosphokinase, muscle type B (CPKMB) and Troponin. The study design was passed on to and approved by both cardiology department of Jundishapur University of Medical Sciences, Ahvaz, Iran, and Medi- cal Ethics Committee of the university. Participants were informed of the study and all gave informed consent to be recruited to the study. 2.3. Measurements Demographic data and past medical history of partici- pants were collected by a trained interviewer using a pretested questionnaire. Each patient’s blood pressure was measured twice, each time from the right arm, in the sitting position, after a fifteen minute rest by the same examiner using a standard mercury sphygmomanometer. Mean of the two values was recorded as an individual’s blood pressure (BP). At the first visit blood samples were obtained between seven and nine in the morning (7-9 AM) after twelve to fourteen hours of overnight fasting. Blood samples were taken from the femoral vein before performing angiography and from the coronary sinus during the procedure; The JL-JR and MP catheters were used for blood sampling from coronary sinus. All sam- ples were centrifuged, kept at 70 degrees Celsius, and analyzed in the same laboratory at the Imam Khomeini Hospital, Ahvaz, and the analysis for all samples was performed on the day of collection. Samples were ana- lyzed for measuring plasma glucose, total cholesterol, HDL, Pentraxin-3, hs-CRP and uric acid. Glucose and total cholesterol measurements were performed with an enzymatic calorimetric assay using glucose oxidase and cholesterol esterase and cholesterol, respectively. Ana- lyses were performed using Pars Azmon kits (Pars Az- mon Inc., Tehran, Iran), Cusabio kits (Cusabio Biotech, Wuhan, Hubei Province, China), and a Selectra 2 auto- analyzer (Vital Scientific, Spankeren, Netherlands). In- tra-assay standard deviations were below 10% in all of the tests. All subjects underwent cardiac imaging with a Sei- mense Samatom Sensation 64-slice scanner. Imaging was performed with a 100-milliseconds scanning time and a single-slice thickness of 3 millimeters. A total of 40 slices were obtained during a single breath-holding pe- riod. Tomographic imaging was electrographically trig- gered at 60 percent of the interval between R waves. All area of calcification within the borders of a coronary artery with a minimal attenuation of 130 Hounsfield units was computed. A calcified coronary plaque was considered present if at least three consecutive pixels were measured (voxel size, 1.03 cubic millimeters). 2.4. Definitions A participant was diabetic if fasting plasma glucose concentration was ≥126 mg/dl on two separate occasions, or if the patient was on treatment with insulin or oral hypoglycemic agents. Smoking was defined as current smoking or having a history of habitual smoking. Hypertension was defined as diastolic blood pressure greater than or equal to 90 mmHg or systolic blood pressure greater than or equal to 140 mmHg or self-re- ported use of antihypertensive drugs. All patients underwent standard coronary angiography assessment through a femoral approach, with standard Seldinger techniques performed by the same cardiologist. Coronary artery stenosis was defined as 70% or more stenosis of the vessel’s diameter. The degree of coronary artery calcification was calcu- lated as described by Agatston et al . [21]. The sum of the scores for all arterial lesions provides an overall score for each subject. 2.5. Statistical Analyses Data are presented as mean ± standard deviation (SD) and frequency (%) for continuous and categorical vari- ables respectively. Continuous variables were checked for the normal distribution assumption using the Kol- mogorov-Smirnov statistics and those that did not satisfy the criteria were log-transformed to attain normal distri- bution. The study group was divided into two subgroups based on angiographic findings. Significant differences between groups were assessed with unpaired two sided Student’s t test or the Mann Whitney test for continuous variables. Heterogeneity of hs-CRP, PTX-3, and calcium score levels were evaluated using ANOVA or Kruskal- Wallis ANOVA (for unequal variances) to distinguish between patients with different degrees of coronary ar- tery disease. Categorical variables were tested with Fisher’s exact or chi square tests. The Pearson coefficient of correlation was used to assess correlations between variables with normal distribution. Significance was set at p < 0.05. In order to assess the diagnostic utility of calcium score and pentraxin levels and determine the optimal cutoff-points for predicting CAD, the receiver operator characteristic (ROC) curve analysis was used with an estimation of the variable’s sensitivity and specificity. The cutoff-point for each variable was assessed by the minimum value of 2 1 sensitivity1 specificity 2 [23] which repre- sented the maximum sum of sensitivity and specificity (MAXss) in each group. In addition to comparing those with CAD with those who had patent coronary arteries, we sought to determine the ability of the variables to distinguish patients with three-vessel disease from the rest of the participants. The area under curve (AUC) relates to the overall ability of using the calcium score and pentraxin level Copyright © 2013 SciRes. OPEN ACCESS 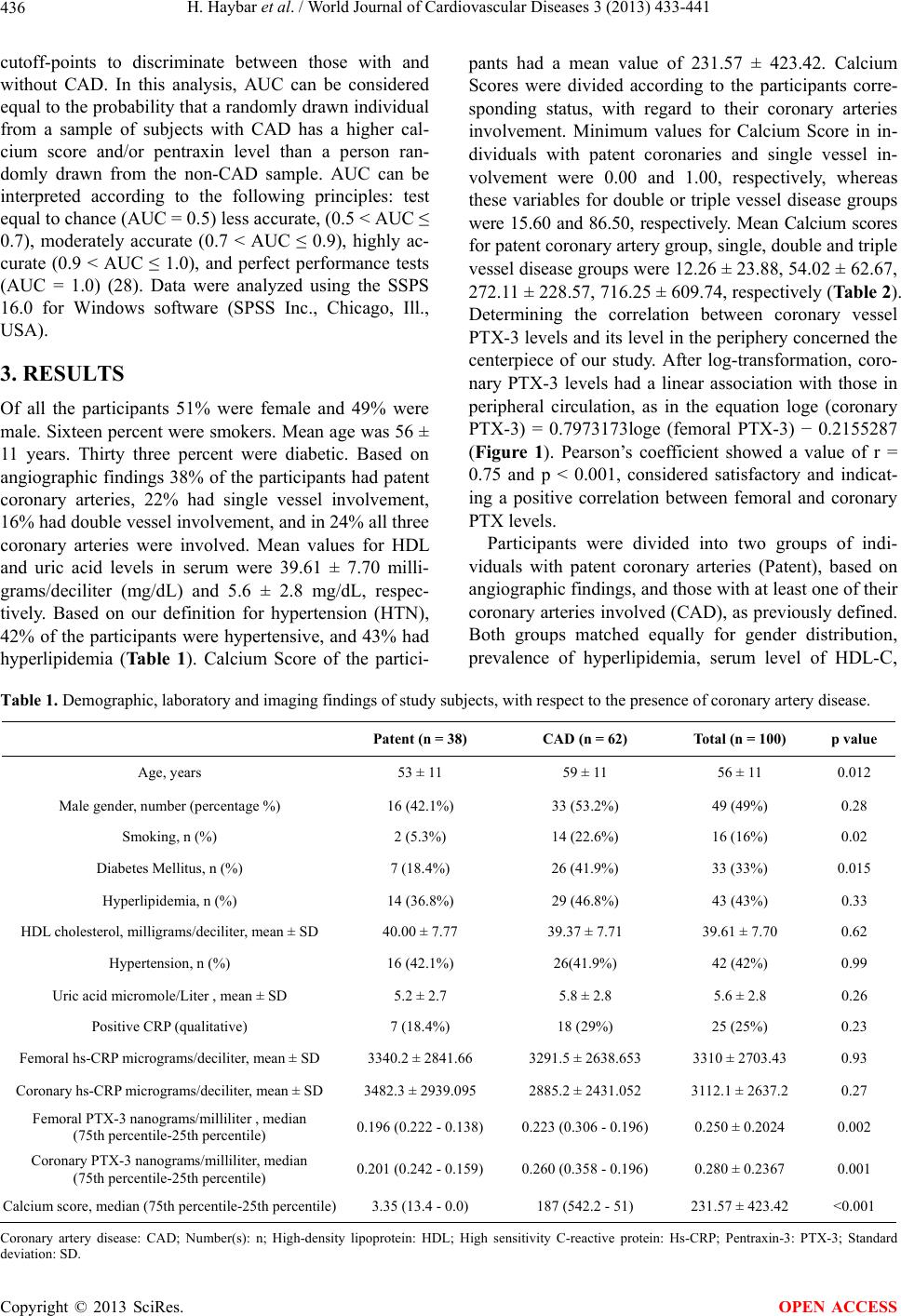 H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 Copyright © 2013 SciRes. 436 OPEN ACCESS cutoff-points to discriminate between those with and without CAD. In this analysis, AUC can be considered equal to the probability that a randomly drawn individual from a sample of subjects with CAD has a higher cal- cium score and/or pentraxin level than a person ran- domly drawn from the non-CAD sample. AUC can be interpreted according to the following principles: test equal to chance (AUC = 0.5) less accurate, (0.5 < AUC ≤ 0.7), moderately accurate (0.7 < AUC ≤ 0.9), highly ac- curate (0.9 < AUC ≤ 1.0), and perfect performance tests (AUC = 1.0) (28). Data were analyzed using the SSPS 16.0 for Windows software (SPSS Inc., Chicago, Ill., USA). 3. RESULTS Of all the participants 51% were female and 49% were male. Sixteen percent were smokers. Mean age was 56 ± 11 years. Thirty three percent were diabetic. Based on angiographic findings 38% of the participants had patent coronary arteries, 22% had single vessel involvement, 16% had double vessel involvement, and in 24% all three coronary arteries were involved. Mean values for HDL and uric acid levels in serum were 39.61 ± 7.70 milli- grams/deciliter (mg/dL) and 5.6 ± 2.8 mg/dL, respec- tively. Based on our definition for hypertension (HTN), 42% of the participants were hypertensive, and 43% had hyperlipidemia (Ta bl e 1 ). Calcium Score of the partici- pants had a mean value of 231.57 ± 423.42. Calcium Scores were divided according to the participants corre- sponding status, with regard to their coronary arteries involvement. Minimum values for Calcium Score in in- dividuals with patent coronaries and single vessel in- volvement were 0.00 and 1.00, respectively, whereas these variables for double or triple vessel disease groups were 15.60 and 86.50, respectively. Mean Calcium scores for patent coronary artery group, single, double and triple vessel disease groups were 12.26 ± 23.88, 54.02 ± 62.67, 272.11 ± 228.57, 716.25 ± 609.74, respectively (Table 2). Determining the correlation between coronary vessel PTX-3 levels and its level in the periphery concerned the centerpiece of our study. After log-transformation, coro- nary PTX-3 levels had a linear association with those in peripheral circulation, as in the equation loge (coronary PTX-3) = 0.7973173loge (femoral PTX-3) − 0.2155287 (Figure 1). Pearson’s coefficient showed a value of r = 0.75 and p < 0.001, considered satisfactory and indicat- ing a positive correlation between femoral and coronary PTX levels. Participants were divided into two groups of indi- viduals with patent coronary arteries (Patent), based on angiographic findings, and those with at least one of their coronary arteries involved (CAD), as previously defined. Both groups matched equally for gender distribution, prevalence of hyperlipidemia, serum level of HDL-C, Table 1. Demographic, laboratory and imaging findings of study subjects, with respect to the presence of coronary artery disease. Patent (n = 38) CAD (n = 62) Total (n = 100) p value Age, years 53 ± 11 59 ± 11 56 ± 11 0.012 Male gender, number (percentage %) 16 (42.1%) 33 (53.2%) 49 (49%) 0.28 Smoking, n (%) 2 (5.3%) 14 (22.6%) 16 (16%) 0.02 Diabetes Mellitus, n (%) 7 (18.4%) 26 (41.9%) 33 (33%) 0.015 Hyperlipidemia, n (%) 14 (36.8%) 29 (46.8%) 43 (43%) 0.33 HDL cholesterol, milligrams/deciliter, mean ± SD 40.00 ± 7.77 39.37 ± 7.71 39.61 ± 7.70 0.62 Hypertension, n (%) 16 (42.1%) 26(41.9%) 42 (42%) 0.99 Uric acid micromole/Liter , mean ± SD 5.2 ± 2.7 5.8 ± 2.8 5.6 ± 2.8 0.26 Positive CRP (qualitative) 7 (18.4%) 18 (29%) 25 (25%) 0.23 Femoral hs-CRP micrograms/deciliter, mean ± SD 3340.2 ± 2841.66 3291.5 ± 2638.653 3310 ± 2703.43 0.93 Coronary hs-CRP micrograms/deciliter, mean ± SD 3482.3 ± 2939.095 2885.2 ± 2431.052 3112.1 ± 2637.2 0.27 Femoral PTX-3 nanograms/milliliter , median (75th percentile-25th percentile) 0.196 (0.222 - 0.138) 0.223 (0.306 - 0.196) 0.250 ± 0.2024 0.002 Coronary PTX-3 nanograms/milliliter, median (75th percentile-25th percentile) 0.201 (0.242 - 0.159) 0.260 (0.358 - 0.196) 0.280 ± 0.2367 0.001 Calcium score, median (75th percentile-25th percentile) 3.35 (13.4 - 0.0) 187 (542.2 - 51) 231.57 ± 423.42 <0.001 Coronary artery disease: CAD; Number(s): n; High-density lipoprotein: HDL; High sensitivity C-reactive protein: Hs-CRP; Pentraxin-3: PTX-3; Standard deviation: SD.  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 437 Table 2. Calcium score in CAD. Calcium score Mean Standard deviation Maximum Minimum One-vessel 54.02 62.67 192.00 1.00 Two-vessel 272.11 228.57 673.70 15.60 Three-vessel 716.25 609.74 2657.30 86.50 Diagnosis Patent 12.26 23.88 127.30 .00 Coronary artery disease: CAD. Figure 1. Log-transformed femoral and coronary PTX. PTX; Pentraxin-3. prevalence of hypertension, serum level of uric acid, a positive qualitative CRP, and either of femoral or coro- nary artery hs-CRP levels. But a statistically significant difference existed between two groups regarding age distribution (p = 0.012), number of smokers (p = 0.02), and prevalence of DM (p = 0.015), both femoral (p = 0.013) and coronary (p = 0.001) artery PTX-3 levels and the Calcium Score (p < 0.001). Mean values and standard deviations of variables are provided in Ta bl e 1. Logistic regression was applied to account for the differences between age and prevalence of DM and smoking on comparing serum PTX-3 levels of coronary and femoral samples and calcium scores between the two groups with a confidence interval (CI) of 95 % (Table 3). Based on our hypotheses the differences between PTX-3 levels, hs-CRP levels and Calcium Score were important and invited further investigation. This time the CAD group was sub-divided into three groups of sin- gle-vessel disease, two-vessel disease and three-vessel disease, and a one-way ANOVA was performed. P values suggested that values for Calcium Score, and femoral vein and coronary sinus PTX-3 levels had a statistically significant difference (Ta bl e 4). Comparison of hs-CRP revealed no significant differences between the groups. Post hoc comparisons using the Tukey test revealed that calcium scores were significantly higher in the three vessel disease groups in comparison to all other groups (p < 0.001). Calcium score for the two vessel disease group also showed significantly higher values compared to that of the patent group (p < 0.05) but was not signifi- cantly higher than the one vessel disease group (p = 0.246). Femoral and coronary PTX-3 levels in the three vessel disease group were higher than the patent (p < 0.0001), one vessel disease (p < 0.01), and two vessel disease (p < 0.05) groups. The prevalence of disease was also assessed for pre- defined subgroups of patients with an Agatston Calcium Score smaller than 10, between 10 and 100, between 100 and 400 and greater than 400 based on a previous study by Rumberger and colleagues [24]. As shown in Table 5, with increasing calcium score the prevalence of signifi- cant CAD increased steeply. In patients with a CS <10 the prevalence of significant CAD was 24.2%, whereas in those with a CS >400 it was 100%. The ROC curve analysis revealed that the Calcium Score was a strong indicator of both CAD and three ves- sel involvement with an area under curve (AUC) of 0.913 (95% CI, 0.86 - 0.97) and 0.944 (95% CI, 0.90 - 0.98) respectively. The optimal cut-off point of Calcium Score for CAD and three vessel involvement were 34.65 (sensitivity of 80% and specificity of 92%) and 116.5 (sensitivity of 96% and specificity of 84%) respectively. To a less extent, femoral PTX-3 level was also an indi- cator of CAD and three vessel involvement with an area under curve (AUC) of 0.68 (95% CI, 0.57 - 0.79) and 0.83 (95% CI, 0.73 - 0.92) respectively. The optimal cut- off points of femoral PTX-3 for CAD and three vessel involvement were 0.22 (sensitivity of 58% and specific- ity of 74%) and 0.56 (sensitivity of 79% and specificity of 70%) respectively. A combination of hs-CRP, calcium score, and PTX-3 achieved an AUC of 0.893 (95% CI, 0.827 - 0.958) for CAD and 0.960 (95% CI, 0.926 - 0.995) for three-vessel involvement. 4. DISCUSSION All of the participants in this study were worried about Copyright © 2013 SciRes. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 438 Table 3. Comparison of CAD predictors between individuals with patent and stenotic coronary arteries, with and without adjustment for age, and presence of DM and smoking. Patent (mean ± SD) CAD (mean ± SD) OR (unadjusted) OR (adjusted) Calcium Score 12.26 ± 23.875 368.2 ± 493.0 1.04 (1.02 - 1.06) 1.03 (1.01 - 1.06) Log-transformed femoral PTX-3 −1.7 ± 0.36 −1.4 ± 0.5 4.6** (1.5 - 13.7) 3.7* (1.1 - 11.8) Log-transformed-coronary PTX-3 −1.6 ± 0.32 −1.3 ± 0.55 6.7** (2.1 - 21.6) 7** (1.9 - 26.2) Coronary artery disease: CAD; Diabetes mellitus: DM; Odds ratio: OR; Pentraxin-3: PTX-3; Standard deviation: SD; *p < 0.05; **p < 0.01. Table 4. Significance of differences between Pentraxin-3, Calcium score and high-sensitivity C-reactive protein among patients with varying numbers of involved coronary arteries. Patent One vessel disease Two vessel diseaseThree vessel disease ANOVA p Femoral hs-CRP micrograms/deciliter 3340 ± 2841.66 3842 ± 2824.730 2572 ± 2411.747 3266 ± 2595.461 0.567 Coronary hs-CRP micrograms/deciliter 3482 ± 2939.095 3125 ± 2519.943 2059 ± 1935.683 3217 ± 2605.439 0.346 Calcium Score 12.26 ± 23.88 54.02 ± 62.67 272.1 ± 228.57 716.25 ± 609.74 <0.0001 Femoral PTX-3 nanograms/milliliter 0.197 ± 0.083 0.21 ± 0.070 0.21 ± 0.070 0.398 ± 0.357 <0.0001 Coronary PTX-3 nanograms/milliliter 0.202 ± 0.060 0.24 ± 0.084 0.26 ± 0.166 0.45 ± 0.411 <0.0001 ANOVA indicates 1-way ANOVA for equal variances or Kruskal-Wallis ANOVA for unequal variances. Values are mean± SD. High-sensitivity C-reactive protein: Hs-CRP; Pentraxin-3: PTX-3. Table 5. Prevalence of disease based on Calcium Score. Disease Patent CAD CountPercent CountPercent <10 25 75.8% 8 24.2% <100 12 40.0% 18 60.0% <400 1 5.6% 17 94.4% Calcium score category >400 0 0.0% 18 100.0% Coronary artery disease: CAD. their health and wanted to know whether they were in a serious peril. Every clinician tries to console his or her patients in a scientifically justifiable manner and would therefore employ the most accurate means, however one must not forget that clinical practice is a delicate balance between ethical, medical, financial and more elements. Hence it is always prudent to develop cost-efficient, ac- curate and reliable medical methods. Demographically the participants in this study were not different from the patient population seeking medical attention in everyday clinical situations. Risk factors were not assessed in the present study; however those detected in our subjects correspond with established risk factors, indicated by other studies [25,26]. A cornerstone of what we propose is the point that serum PTX-3 levels in peripheral vessels, such as femoral vessels can be re- liably used instead of coronary level values. It enables us to measure a variable of our desired equation to predict coronary artery stenosis, without depending on interven- tional modalities. What is intriguing is the point that al- though Calcium Scores are different for different catego- ries of coronary artery involvement in general, this dif- ference is significant only when comparing a patient with all three of coronary arteries involved, with the rest, and also when comparing two-vessel disease group with pat- ent coronary group. We could assume Calcium Score by itself can predict the presence of a two or three-vessel involvement, but falls short of differentiating between individuals without any significant coronary artery in- volvement and those with CAD. One of the powers of the present study is that the gold standard of diagnosis, that is, coronary angiography was used to determine sig- nificant stenosis; as shown in other studies [26] due to artifact caused by extensive calcification, imaging mo- dalities like CT angiography may overestimate the extent of stenosis. Femoral venous PTX-3 levels were also different among four groups. However, PTX-3 is a more contro- versial issue and its role is not yet fully understood [26- 31]. Nevertheless PTX-3 levels were significantly higher in the individuals with three-vessel stenosis, than any other groups, and it seems to be a reliable indicator of significant coronary artery stenosis. Regardless of its utility in predicting mortality of pa- tients with CAD, as suggested by other studies [8,12-14], we found that serum levels of hs-CRP do not correlate with coronary artery stenosis. Our main objective was to be able to avoid unnecessary angiography in patients; Copyright © 2013 SciRes. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 439 whether we could predict significant coronary artery stenosis, ahead of performing cardiac catheterization. According to our findings serum levels of PTX-3 and Calcium Scores are much higher in individuals with sig- nificant stenosis of coronary arteries, than those with pa- tent vessels. Our argument is that if we consider enough variables, we may be able to predict the presence of sig- nificant coronary stenosis. Of course this holds true for patients within the intermediate-risk category based on a standard exercise test. As another study on a similar population had suggested [32], both coronary sinus and femoral arterial PTX-3 levels are independent predictors of CAD; also, a combined model of traditional CAD risk factors and femoral arterial PTX-3 levels would make net reclassification improvement indices 40% and 15% regarding cutpoint-free and cutpoint-based assumptions, respectively. Rumberger and colleagues [24] used 10, 100 and 400 intervals for Calcium Score as a basis for categorizing individuals in order to what. We used the same amounts and observed that indeed very few individuals without significant stenosis in any of their coronary arteries had Calcium Scores higher than 100. However similar argu- ment cannot be made about Calcium Score in patients with CAD. Calculating the Area under Curves considering both three-vessel disease and the rest of the participants, and presence of a significant stenosis in any of the coronary arteries versus patent vessels resulted in the conclusion that Calcium Score has a satisfactory ability in differen- tiating the two groups, in both of these settings. PTX-3 can also be used in the same manner. The calculated AUC for the combination of hs-CRP, PTX-3 and calcium score for different groups of patients, suggests that cal- cium score is a better predictor of CAD in our sample than a combination of hs-CRP, PTX-3 and calcium score; while among patients with three-vessel involvement, combined model had a slightly higher AUC, compared to calcium score alone (0.960 versus 0.944). This finding is compatible with other findings of our study, regarding individuals with three-vessel disease. 5. CONCLUSION PTX3 levels in peripheral vessels can reliably be used to predict coronary level values enabling prediction of coronary artery stenosis without depending on interven- tional modalities. Furthermore, Calcium Score calculated using multi-slice CT scanning, without contrast, is cheaper, safer and more available than angiography or CT angiography; however, its utility to determine pres- ence of significant coronary artery stenosis relies on us- ing additional inputs, such as serum PTX-3 levels. Still, the number of stenotic coronary arteries might limit the applicability of such combined models. 6. LIMITATIONS AND SUGGESTIONS A limitation of our study was that we did not have base- line values of PTX-3 of our patients for comparison. Another limitation is related to the point that calcifica- tion of blood vessels is a natural ongoing process in hu- man body, and can be altered by changes in metabolism, particularly that of calcium. As other authors [23] have pointed out, outside an arbitrary range for age, Calcium Score may fail to produce the expected results. It is advisable that future studies be designed to deter- mine the correlation between Calcium Score and per- centage of stenosis in the lumen of coronary arteries and whether it could be used to construct a model for pre- dicting the behavior of atherosclerotic process in coro- nary arteries. Although the mechanisms involved with PTX-3 are not the main foci of this study, determining the actual role of PTX-3 in MI plays an essential part in structuring risk-stratification models that incorporate this variable. That is, if there are variations in base-line level of PTX-3 due to acute MI, the period between PTX-3 measurement and onset of acute cardiac event can alter the results of any study significantly. 7. ACKNOWLEDGMENT Our special thanks go to members of Golestan Hospital Clinical Development Research Unit for helping us in submission and sub- mission consultancy Gholamreza Eskandari Joi and for data collection. REFERENCES [1] Murray, C. and Lopez, A. (1997) Global mortality, dis- ability, and the contribution of risk factors: Global Bur- den of Disease Study. The Lancet, 349, 1436-1442. http://dx.doi.org/10.1016/S0140-6736(96)07495-8 [2] Fuster, V., Badimon, L., Badimon, J.J. and Chesebro, J.H. (1992) The pathogenesis of coronary artery disease and the acute coronary syndrome. New England Journal of Medicine, 326, 242-250. http://dx.doi.org/10.1056/NEJM199201233260406 [3] Fuster, V. and Lewis, A. (1995) Conner memorial lecture. Mechanisms leading to myocardial infarction: Insights from studies of vascular biology. Circulation, 90, 2126- 2146. http://dx.doi.org/10.1161/01.CIR.90.4.2126 [4] Gibbons, R.J., Chatterjee, K., Daley, J., Douglas, J.S., Fihn, S.D, Gardin, J.M., et al. (1999) ACC/AHA/ACP- ASIM guidelines for the management of patients with chronic stable angina: Executive summary and recom- mendations: A report of the American College of Cardi- ology/American Heart Association Task Force on Prac- tice Guidelines (committee on management of patients with chronic stable angina). Circulation, 99, 2829-2848. http://dx.doi.org/10.1161/01.CIR.99.21.2829 [5] Braunwald, E. (1997) Unstable angina: Diagnosis and management-clinical practice guideline. DIANE Publish- Copyright © 2013 SciRes. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 440 ing, Darby. [6] Hessel, S.J., Adams, D.F. and Abrams, H.L. (1981) Com- plications of angiography. Radiology, 138, 273-281. [7] Kwok, J.M.F., Miller, T.D., Christian, T.F., Hodge, D.O. and Gibbons, R.J. (1999) Prognostic value of a treadmill exercise score in symptomatic patients with non-specific ST-T abnormalities on resting ECG. Journal of American Medical Association, 282, 1047-1053. http://dx.doi.org/10.1001/jama.282.11.1047 [8] Lodh, M., Goswami, B., Parida, A., Patra, S. and Saxena, A. (2012) Assessment of serum leptin, pregnancy-asso- ciated plasma protein A and CRP levels as indicators of plaque vulnerability in patients with acute coronary syn- drome. Cardiovascular Journal of Africa, 23, 330-335. http://dx.doi.org/10.5830/CVJA-2012-008 [9] Polonsky, T.S., McClelland, R.L., Jorgensen, N.W., Bild, D.E., Burke, G.L., Guerci, A.D., et al. (2010) Coronary artery calcium score and risk classification for coronary heart disease prediction. Journal of American Medical Association, 303, 1610-1616. http://dx.doi.org/10.1001/jama.2010.461 [10] Wexler, L., Brundage, B., Crouse, J., Detrano, R., Fuster, V., Maddahi, J., et al. (1996) Coronary artery calcifica- tion: Pathophysiology, epidemiology, imaging methods, and clinical implications. A statement for health profes- sionals from the American Heart Association. Circulation, 94, 1175-1192. http://dx.doi.org/10.1161/01.CIR.94.5.1175 [11] Vidula, H., Tian, L., Liu, K., Criqui, M.H., Ferrucci, L., Pearce, W.H., et al. (2008) Biomarkers of inflammation and thrombosis as predictors of near-term mortality in pa- tients with peripheral arterial disease: A cohort study. Annals of Internal Medicine, 148, 85-93. http://dx.doi.org/10.7326/0003-4819-148-2-200801150-0 0003 [12] Anderson, J.L., Carlquist, J.F., Muhlestein, J.B., Horne, B.D. and Elmer, S.P. (1998) Evaluation of C-reactive protein, an inflammatory marker, and infectious serology as risk factors for coronary artery disease and myocardial infarction. Journal of the American College of Cardiol- ogy, 32, 35-41. http://dx.doi.org/10.1016/S0735-1097(98)00203-4 [13] Cho, D.Y., Kim, K.N., Kim, K.M., Lee, D.J. and Kim, B.T. (2012) Combination of high-sensitivity C-reactive protein and homocysteine may predict an increased risk of coronary artery disease in Korean population. Chinese Medical Journal, 125, 569-573. [14] Savchenko, A.S., Imamura, M., Ohashi, R., Jiang, S., Kawasaki, T., Hasegawa, G., et al. (2008) Expression of Pentraxin 3 (PTX3) in human atherosclerotic lesions. The Journal of Pathology, 215, 48-55. http://dx.doi.org/10.1002/path.2314 [15] Klouche, M., Peri, G., Knabbe, C., Eckstein, H.H., Schmid, F.X., Schmitz, G., et al. (2004) Modified atherogenic lipoproteins induce expression of Pentraxin-3 by human vascular smooth muscle cells. Atherosclerosis, 175, 221-228. http://dx.doi.org/10.1016/j.atherosclerosis.2004.03.020 [16] Mantovani, A., Garlanda, C., Bottazzi, B., Peri, G., Doni, A. and Martinez de la Torre, Y., et al. (2006) The long Pentraxin PTX3 in vascular pathology. Vascular Phar- macology, 45, 326-330. http://dx.doi.org/10.1016/j.vph.2006.08.011 [17] Latini, R., Maggioni, A.P., Peri, G., Gonzini, L., Lucci, D., Mocarelli, P., et al. (2004) Prognostic significance of the long Pentraxin PTX3 in acute myocardial infarction. Circulation, 110, 2349-2354. http://dx.doi.org/10.1161/01.CIR.0000145167.30987.2E [18] Karakas, M.F., Buyukkaya, E., Kurt, M., Motor, S., Ak- cay, A.B., Buyukkasa, S., et al. (2013) Serum pentraxin 3 levels are associated with the complexity and severity of coronary artery disease in patients with stable angina pectoris. Journal of Investigative Medicine, 61, 278-285. [19] Jenny, N.S., Arnold, A.M., Kuller, L.H., Tracy, R.P. and Psaty, B.M. (2009) Associations of Pentraxin 3 with car- diovascular disease and all-cause death. Arteriosclerosis, Thrombosis, and Vascular Biology, 29, 594-599. http://dx.doi.org/10.1161/AT VBAHA.108.178947 [20] Hou Z.H., Lu, B., Gao, Y., Jiang, S.L., Wang, Y., Li, W., et al. (2012) Prognostic Value of coronary CT angiogra- phy and calcium score for major adverse cardiac events in outpatients. Journal of American College of Cardiology Cardiovascular Imaging, 5, 990-999. http://dx.doi.org/10.1016/j.jcmg.2012.06.006 [21] Greenland, P., Bonow, R.O., Brundage, B.H., Budoff, M.J., Eisenberg, M.J., Grundy, S.M., et al. (2007) ACCF/ AHA 2007 clinical expert consensus document on coro- nary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain. Journal of the American College of Cardiology, 49, 378-402. http://dx.doi.org/10.1016/j.jacc.2006.10.001 [22] Agatston, A.S., Janowitz, W.R., Hildner, F.J., Zusmer, N.R., Viamonte Jr., M. and Detrano, R. (1990) Quantifi- cation of coronary artery calcium using ultrafast com- puted tomography. Journal of the American College of Cardiology, 15, 827-832. http://dx.doi.org/10.1016/0735-1097(90)90282-T [23] Perkins, N.J. and Schisterman, E.F. (2006) The inconsis- tency of “optimal” cut-points using two ROC based crite- ria. American Journal of Epidemiology, 163, 670-675. http://dx.doi.org/10.1093/aje/kwj063 [24] Zweig, M.H. and Campbell, G. (1993) Receiver-operat- ing characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clinical Chemistry, 39, 561- 577. [25] Rumberger, J.A., Brundage, B.H., Rader, D.J. and Kon- dos, G. (1999) Electron beam computed tomographic coronary calcium scanning: A review and guidelines for use in asymptomatic persons. Mayo Clinic Proceedings, 74, 243-252. http://dx.doi.org/10.4065/74.3.243 [26] Tamon, R., Kou, Y., Yoshida, Y., Ogawa, Y. and Imaki, M. (2011) Study on the evaluation of serum hsCRP as predictor of the coronary artery disease by using Fram- ingham Risk Score (FRS). Journal of Analytical Bio- Science, 34, 324-330. [27] Soeki, T., Niki, T., Kusunose, K., Bando, S., Hirata, Y., Tomita, N., et al. (2011) Elevated concentrations of Pen- Copyright © 2013 SciRes. OPEN ACCESS  H. Haybar et al. / World Journal of Cardiovascular Diseases 3 (2013) 433-441 Copyright © 2013 SciRes. 441 OPEN ACCESS traxin 3 are associated with coronary plaque vulnerability. Journal of Cardiology, 58, 151-157. http://dx.doi.org/10.1016/j.jjcc.2011.04.005 [28] Norata, G.D., Marchesi, P., Pulakazhi Venu, K.V., Pasqualini, F., Anselmo, A., Moalli, F., et al. (2009) De- ficiency of the long Pentraxin PTX3 promotes vascular inflammation and atherosclerosis. Circulation, 120, 699- 708. http://dx.doi.org/10.1161/CIRCULATIONAHA.108.8065 47 [29] Leali, D., Inforzato, A., Ronca, R., Bianchi, R., Belleri, M., Coltrini, D., et al. (2012) Long pentraxin 3/tumor ne- crosis factor-stimulated gene-6 interaction: A biological rheostat for fibroblast growth factor 2-mediated angio- genesis. Arteriosclerosis, Thrombosis, and Vascular Bi- ology, 32, 696-703. http://dx.doi.org/10.1161/AT VBAHA.111.243998 [30] Norata, G.D., Garlanda, C. and Catapano, A.L. (2010) The long Pentraxin PTX3: A modulator of the immu- noinflammatory response in atherosclerosis and cardio- vascular diseases. Trends in Cardiovascular Medicine, 20, 35-40. http://dx.doi.org/10.1016/j.tcm.2010.03.005 [31] Norata, G.D., Marchesi, P., Pirillo, A., Uboldi, P., Chiesa, G., Maina, V., et al. (2008) Long pentraxin 3, a key com- ponent of innate immunity, is modulated by high-density lipoproteins in endothelial cells. Arteriosclerosis, Throm- bosis, and Vascular Biology, 28, 925-931. http://dx.doi.org/10.1161/AT VBAHA.107.160606 [32] Haybar, H., Assareh, A., Ghotbi, Y., Torabizadeh, M. and Bozorgmanesh, M. (2013) Incremental diagnostic value of circulating pentraxin in patients with intermediate risk of coronary artery disease. Heart, 99, 640-648. http://dx.doi.org/10.1136/heartjnl-2012-303560
|