L. C. N. ARAUJO ET AL.
230
changes in the production and metabolism of metallo-
proteinase [5,6], confirmed by statistical correlation be-
tween thickness and amount of bladder neck elastic fi-
bers (Table 3).
In vitro studies indicate that tobacco consumption pre-
vents collagen production and increases tropoelastin pro-
duction and activation of metalloproteinase, causing a
degradation of matrix proteins and a abnormal produc-
tion of elastic material, in its morphology and amount,
having as a consequence the increase of the number of
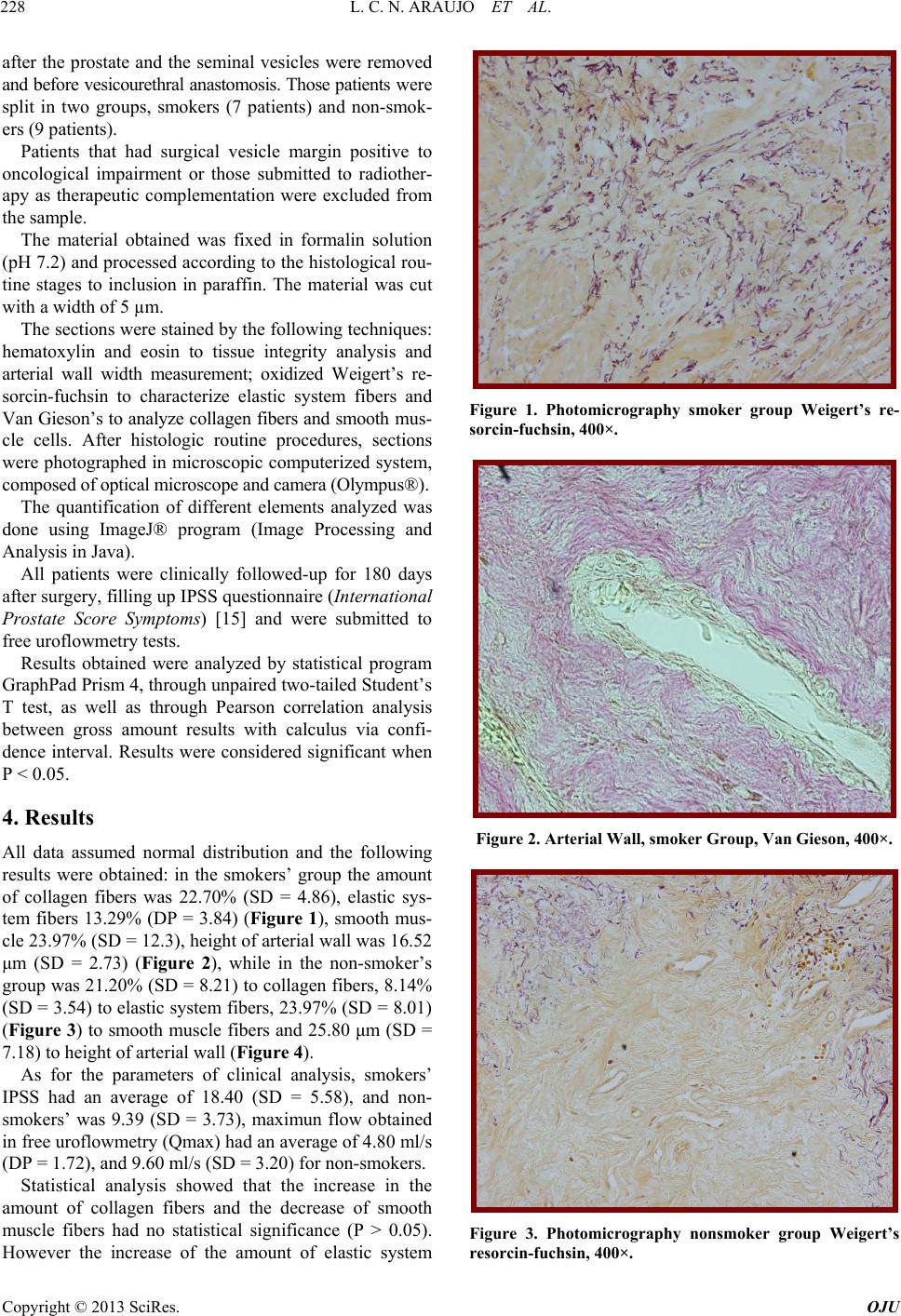
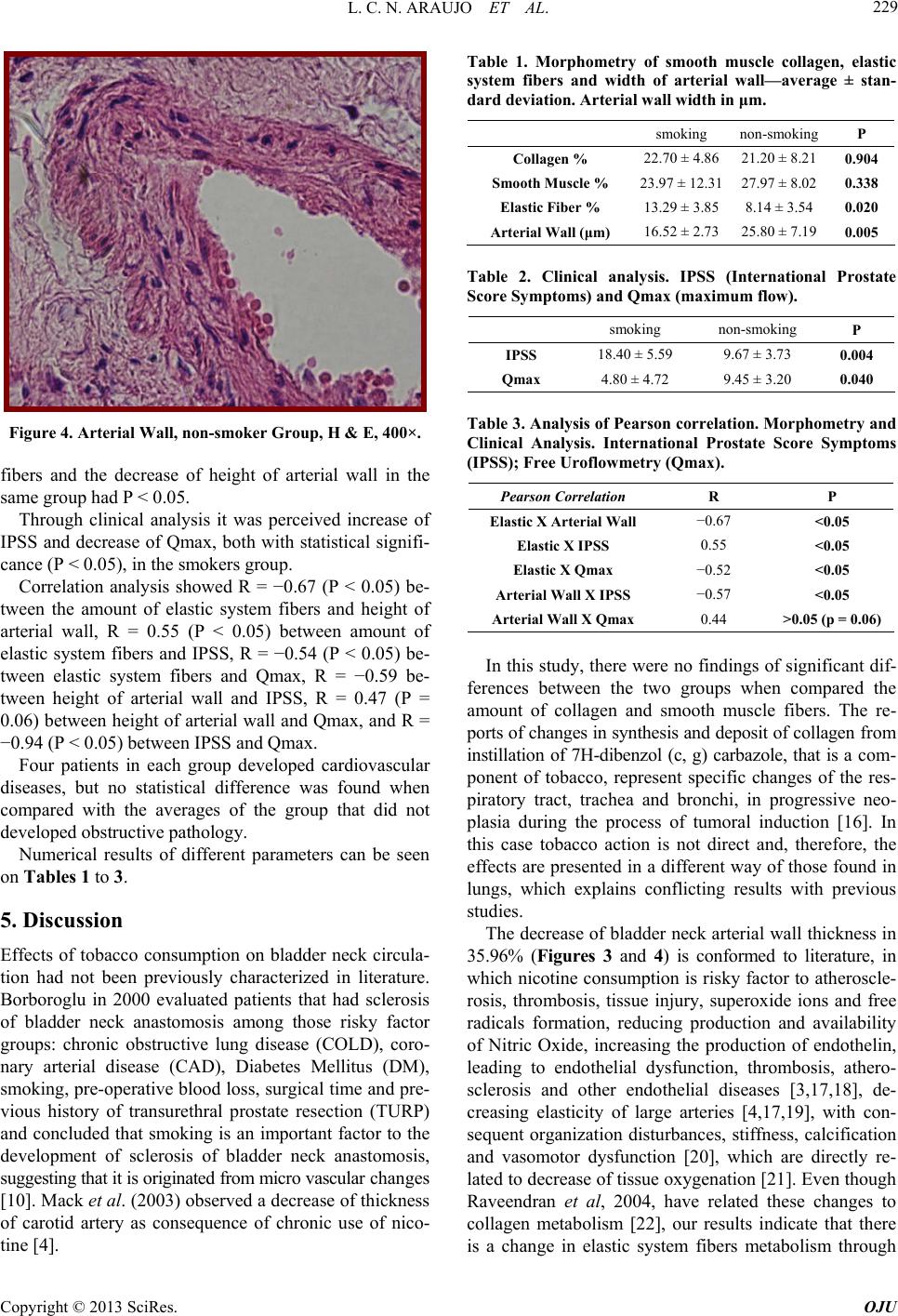
elastic system fibers in the skin [4-6]. In our results we
have seen an increase of 62.36% of elastic system fibers
in bladder neck tissue in smokers group when compared
to non-smokers (Figures 1 and 2). Morita, associated
these findings to early skin ageing [6].
Effect of smoking on the arterial system and conse-
quent formation of elastic system fibers may not be lim-
ited to bladder neck, being distributed in all bladder, with
an increase of elastic system fibers in all bladder wall
and its repercussions, being able to cause early ageing,
but there are no ways of getting definitive conclusions,
once there are no previous data in the literature on blad-
der ageing.
Not with standing the results in clinical data have been
statistically significant, they should be viewed with re-
strictions mainly by the number of participants and the
absence of data related to detrusor function provided by
uroflowmetry, once the study design was not meant to
morphological evaluation only, and as such there are no
previous data of bladder function in smokers. Gathered
data may be, in spite of statistical significance, a coinci-
dence, and are necessary future clinical studies to con-
firm the present findings. Results will be discussed only
in order to be compared to further.
Results found on clinical data supposedly indicated an
impact related to tobacco consumption both in IPSS re-
sult, with an increase of approximately 93%, as in Qmax
reduction, with a decrease of about 51%, which was re-
flected in a reduction of voiding function statistically
significant in smokers when compared to those that were
not exposed to nicotine.
Correlation analysis between quantitative data and clini-
cal results shows that there can be a strong connection
between clinical changes related to amount of elastic
system fibers. Even though there is a great limitation of
data, which leads to absence of definitions regarding de-
trusor behavior, as for number of specimens, there should
be a supposed early ageing that can happen to bladder
tissue as well as skin [6], which should explain the
changes that were found, with a probable reduction in
detrusor contractility, as results are related to smoking
and not with existence of cardiovascular diseases. But
stating a definitive conclusion will only be possible with
studies that evaluate detrusor function.
6. Conclusions
In the present study, smoking modified bladder neck ex-
tra-cell matrix of patients submitted to radical prostatec-
tomy with an increase of the amount of elastic system
fibers (P < 0.05).
It is also observed a decrease of arterial wall height in
the same group with statistical correlation (P < 0.05).
REFERENCES
[1] S. T. Hanna, “Nicotine Effect on Cardiovascular System
and Ion Channels,” Journal of Cardiovascular Pharma-
cology, Vol. 47, No. 3, 2006, pp. 348-358.
[2] U. John, S. E. Baumeister, C. Kessler and H. Volzke,
“Associations of Carotid Intima-Media Thickness, To-
bacco Smoking and Overweight with Hearing Disorder in
a General Population Sample,” Atherosclerosis, Vol. 195,
No. 1, 2007, pp. e144-e149.
http://dx.doi.org/10.1016/j.atherosclerosis.2007.04.007
[3] N. Lindenblatt, U. Platz, J. Hameister, E. Klar, M.D.
Menger and B. Vollmar, “Distinct Effects of Acute and
Chronic Nicotine Application on Microvascular Throm-
bus Formation and Endothelial Function in Male and Fe-
male Mice,” Langenbeck’s Archives of Surgery, Vol. 392,
No. 3, 2007, pp. 285-295.
http://dx.doi.org/10.1007/s00423-007-0173-6
[4] W. J. Mack, T. Islam, Z. R. H. Lee, Selzer, et al., “Envi-
ronmental Tobacco Smoke and Carotid Arterial Stiff-
ness,” Preventive Medicine, Vol. 37, No. 2, 2003, pp.
148-154.
http://dx.doi.org/10.1016/S0091-7435(03)00097-5
[5] M. Just, Ribera, M. Monso, E. Lorenzo, J. C. Lorenzo and
C. Ferrándiz, “Effect of Smoking on Skin Elastic Fibres:
Morphometric and Immunohistochemical Analysis,” Bri-
tish Journal of Dermatology, Vol. 156, No. 1, 2007, pp.
85-91.
http://dx.doi.org/10.1111/j.1365-2133.2006.07575.x
[6] A. Morita, “Tobacco Smoke Causes Premature Skin Ag-
ing,” Journal of Dermatological Science, Vol. 48, No. 3,
2007, pp. 169-175.
http://dx.doi.org/10.1016/j.jdermsci.2007.06.015
[7] H. Tanaka, Y. Ono, Y. Nakata, N. Shintani, et al., “To-
bacco Smoke Extract Induces Premature Skin Aging in
Mouse,” Journal of Dermatological Science, Vol. 46, No.
1, 2007, pp. 69-71.
http://dx.doi.org/10.1016/j.jdermsci.2006.11.009
[8] G. D. Batty, M. Kivimaki, G. D. Gray, M. G. Smith, et al.,
“Cigarette Smoking and Site-Specific Cancer Mortality:
Testing Uncertain Associations Using Extended Fol-
low-up of the Original Whitehall Study,” Annals of On-
cology, Vol. 191, No. 5, 2008, pp. 996-1002.
[9] S. Boorjian, J. E. Cowan, B. R. Konety, J. DuChane, et
al., “Bladder Cancer Incidence and Risk Factors in Men
with Prostate Cancer: Results from Cancer of the Prostate
Strategic Urologic Research Endeavor,” Journal of Urol-
ogy, Vol. 177, No. 3, 2007, pp. 883-887.
[10] P. G. Borboroglu, J. P. Sands, J. L. Roberts and C. L.
Copyright © 2013 SciRes. OJU