Modern Plastic Surgery, 2013, 3, 120-122
http://dx.doi.org/10.4236/mps.2013.34024 Published Online October 2013 (http://www.scirp.org/journal/mps)
Transdermal Nitroglycerine Patch: An Optional Device to
Reduce Flap Venous Congestion? A Case Report
Sara Di Lorenzo, Bartolo Corradino, Adriana Cordova
Department of Surgi cal Oncology, Pla stic Surgery Unit, University of Palermo, Palermo, Italy.
Email: saradilorenz@gmail.com, dilsister@libero.it
Received August 1st, 2013; revised September 1st, 2013; accepted September 8th, 2013
Copyright © 2013 Sara Di Lorenzo et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
Sometimes in free flap there is a venous congestion without an obstruction of the venous anastomosis or other organic
causes of reduction venous drainage (haematoma, seroma compressing the pedicle). In these cases the authors suggest
the application of nitrog lycerine patch in the cong ested area of the fla p few hours befor e the surgical ex ploration of the
anastomosis. If there is a fast improvement of the clinical feature of the flap, the surgical exploration could be avoided.
The authors underline that applying the nitroglycerin patch should not be regarded in any way as a therapy of a free flap
venous thrombosis but only as an useful device, an option to be taken only when the surgeon is undecided whether to
revisit the anastomosis or not.
Keywords: Free Flap Failure; Venous Congestion; Vascular Pedicle Thrombosis; Microsurgical Complications
1. Introduction
The majority of surgical complications after tissue trans-
fer surgery are related to vascular thrombosis, which
usually occur within 3 days of surgery, but sometimes
thrombosis can occur later.
There are many techniques available for evaluation of
flap viability. The most common technique is clinical
observation and Doppler vascular pedicle monitoring.
The clinical observation is very useful when the flap has
a skin island.
Venous thrombosis occurs more frequently because of
its low-flow, low-pressure nature, and because it may
evolve over se ver al h ours.
A venous congestion usually results in oedema and
darkening of the skin colour.
During early venous obstruction a needle stick will
cause a rapid bleeding of dark blood. The capacity to
understand and id entify the early signs of flap suff erance
is important in order to decide if surgical explorations,
and an additional pharmacological therapy or something
else are necessary.
If a flap’s vascular integrity is in question, if there is a
doubt of venous thrombo sis at the anastomosis, a prompt
surgical exploration is mandatory [1].
Surgical exploration is still mandatory when there are
haematoma and seroma that could make a compression
on the vascular pedicle.
Sometimes there is a venous congestion of the flap
without an obstruction of the venous vessel at the anas-
tomotic site. In the surgical exploration sometimes there
is no problem at the anastomotic site or other organic
causes of reduction venous drainage.
This kind of insufficient venous drainage may cause a
slow partial flap loss that may require further surgical
steps, multiple debridements to remove necrotic tissue
and prevent further complications as infections, and to
improve the outcome.
Authors expose their experience with a nitroglycerine
plaster applied on flap in order to reduce the venous
congestion of a free DIEP flap. It begun in the 5th day
after surgery.
2. Clinical Case
The patient is a 38-year-old female undergone a right
mastectomy for a ductal carcinoma and a quadrantec-
tomy on the left breast for a dysp lasia.
A delayed free Diep Flap reconstruction of the right
breast was performed using the internal mammary ves-
sels, as recipient vessels. The ischemia time was less than
2 hours.
The flap seemed well perfused.
The patient didn’t smoke and hadn’t risk factor or sys-
temic disease.
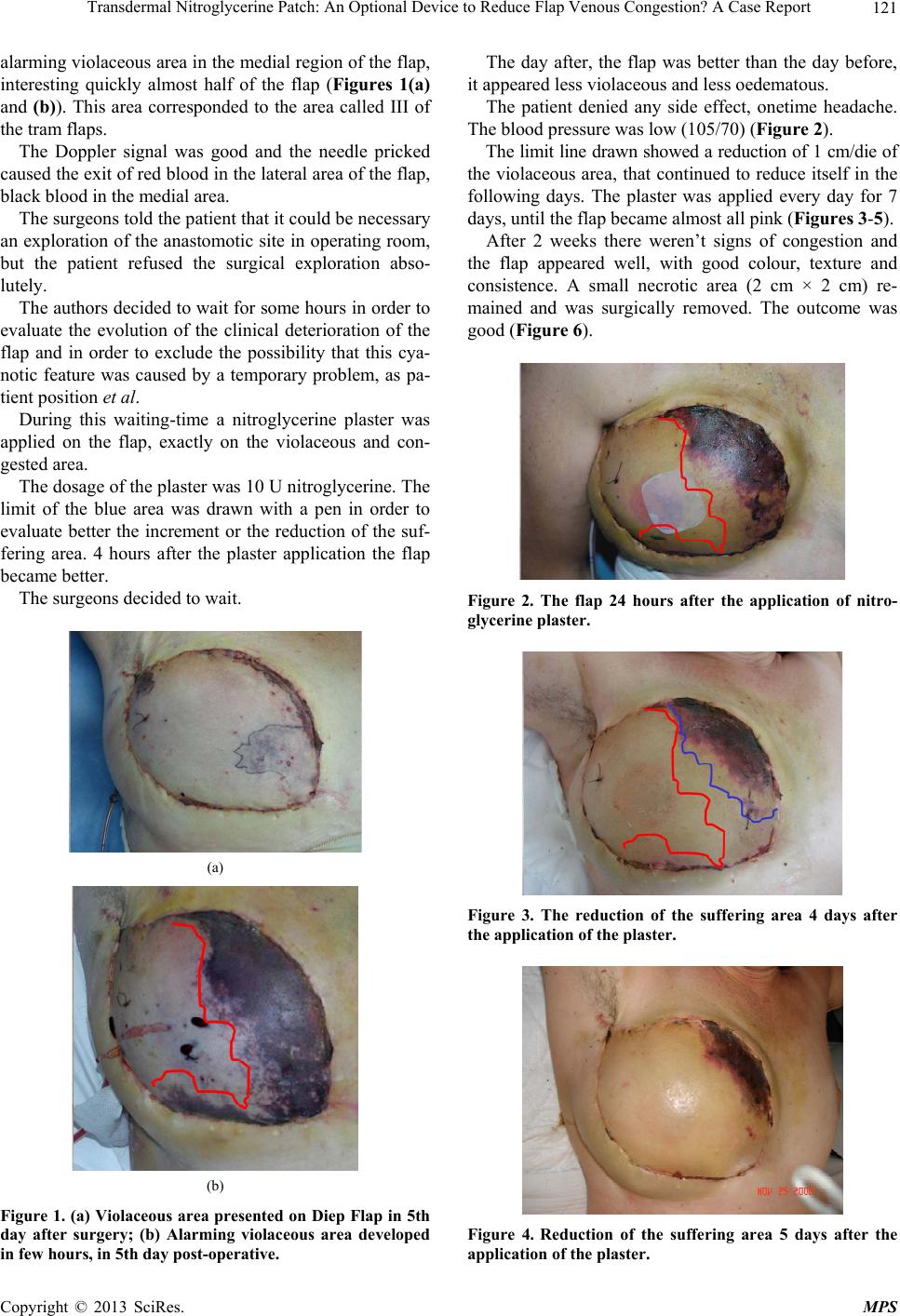
On 5th day after surgery the patient presented an
Copyright © 2013 SciRes. MPS